

Abstract
Our aim was to examine the rates and predictors of father attendance at nurse home visits in replication sites of the Nurse-Family Partnership (NFP). Early childhood programs can facilitate father involvement in the lives of their children, but program improvements require an understanding of factors that predict father involvement. The sample consisted of 29,109 low-income, first-time mothers who received services from 694 nurses from 80 sites. We conducted mixed-model multiple regression analyses to identify population, implementation, site, and nurse influences on father attendance. Predictors of father attendance included a count of maternal visits (B = 0.12, SE = 0.01, F = 3101.77), frequent contact between parents (B = 0.61, SE = 0.02, F = 708.02), cohabitation (B = 1.41, SE = 0.07, F = 631.51), White maternal race (B = 0.77, SE = 0.06, F = 190.12), and marriage (B = 0.42, SE = 0.08, F = 30.08). Random effects for sites and nurses predicted father-visit participation (2.7 & 6.7% of the variance, respectively), even after controlling for population sociodemographic characteristics. These findings suggest that factors operating at the levels of sites and nurses influence father attendance at home visits, even after controlling for differences in populations served. Further inquiry about these influences on father visit attendance is likely to inform program-improvement efforts.
Father involvement in the lives of children, such as being physically available to the child; engaging in nurturing, caregiving, and mentoring behaviors; and ensuring the provision of adequate financial resources for basic needs is associated with adaptive child health and development (Amato & Rivera, 1999; Bronte-Tinkew, Carrano, Horowitz, & Kinukawa, 2008; Dubowitz et al., 2001; Sarkadi, Kristiansson, Oberklaid, & Bremberg, 2008; White & Gilbreth, 2001). A sizeable literature has shown that these relationships hold for residential biological fathers, and some evidence has suggested that nonbiological fathers (i.e., social and stepfathers) also provide protective influences (Bzostek, 2008; Dubowitz et al., 2001; Jayakody & Kalil, 2002). When fathers engage in antisocial behavior or are impaired by psychopathology, beneficial child outcomes are not found; rather, increased risks are evident (Blazei, Iacono, & McGue, 2008; Jaffee, Moffitt, Caspi, & Taylor, 2003; Kane & Garber, 2004; Marmorstein, Malone, & Iacono, 2004).
Importance of Including Fathers in Early Childhood Prevention Programs
Early childhood home-visiting programs are ideally poised to help mothers and fathers learn adaptive parenting behaviors that contribute to healthy child development (Olds, Sadler, & Kitzman, 2007). Prevention focused early childhood home visitation programs have, historically, worked almost exclusively mothers, including fathers and other important caregivers as possible (Duggan et al., 2004; Sar, Antle, Bledsoe, Barbee, & Van Zyl, 2010; Smith, Duggan, Bair-Merritt, & Cox, 2012). Over the past decade, fatherhood and home-visitation advocates have argued that prevention programs should increase their outreach to fathers and family members to enhance program engagement, support all care-givers, and promote family achievement of program goals (e.g., Guterman, 2012; Korfmacher et al., 2008; Sar et al., 2010). Key components of the rationale supporting program-improvement efforts to increase father engagement stem from references to broader developmental and intervention research showing that both parents uniquely affect child outcomes, the transition to parenting is a key opportunity to impact parents' relationships and coparenting, and these factors are positively associated with adaptive family environment and life-course outcomes that ultimately benefit the child (Sar et al., 2010).
Outcomes Associated With Father Involvement in Early Childhood Prevention Programs
Two recent reviews have summarized outcomes of father involvement in, broadly defined, early childhood prevention and intervention programs (Panter-Brick et al., 2014; Smith et al., 2012). Those reviews have concluded that father involvement in prevention and intervention programming is mixed. Conclusions are limited by significant study heterogeneity (i.e., programs, populations), study methods that do not readily allow for the disag-gregation of effects attributable to father involvement, and outcome data on paternal functioning and parenting that are rarely available (Panter-Brick et al., 2014; Smith et al., 2012). Notable encouraging trends from individual outcome studies of father involvement in broadly defined parenting programs (e.g., often from interventions that were delivered in parenting groups and with latency and older children) have found that compared to mother-alone groups, groups comprised of fathers and mothers have stronger and longer lasting impacts (e.g., Bakermans-Kranenburg, van IJzendoorn, & Juffer, 2003; Cowan, Cowan, Pruett, Pruett, & Wong, 2009; Lundahl, Tollefson, Risser, & Lovejoy, 2008) or see impacts only among cohabiting couples (Hahlweg, Heinrichs, Kuschel, Bertram, & Naumann, 2010). Mixed findings also have been seen regarding the impact of father program participation on domestic violence outcomes (Bugental, 2004; Duggan et al., 2004).
Specifically, the Hawaii Healthy Start trial found an increase in father involvement for the subgroup of mothers who had violent partners with little involvement at intake and without evidence of diminished violence (Duggan et al., 2004). By contrast, Bugental (2004) found that families in the the cogntive skill enhanced model of home visitation reported signficantly less family violence as compared with those receiving traditional home visitation.
General Predictors of Early Childhood Father Involvement with Parenting
In young and low-income families, such as those targeted by home-visitation programs, father involvement is often limited because romantic unions tend to be short-lasting and because paternal involvement declines after couples separate (Braver et al., 1993; Bronstein, Stoll, Clauson, Abrams, & Briones, 1994; Carlson, McLanahan, & England, 2004; Wood & Covington, 2014). The pattern of declining paternal involvement is especially prevalent among parents who were not married at the time of their child's birth (Ryan, Kalil, & Ziol-Guest, 2008).
The literature on correlates of father participation in early childhood parenting programs typically has found greater father involvement to be inversely associated with mothers', fathers' and families' levels of risks (e.g., being unmarried, parental separation, nonresident fathering, low financial security, low education, low maternal program engagement, low use of other community services, low maternal appraisals of paternal caregiving, low paternal caregiving skills) (Fagan, 1999; Gavazzi & Schock, 2004; Gavidia-Payne & Stoneman, 1997; Lengua et al., 1992; Raikes, Green, At-water, Kisker, Constantine, & Chazan-Cohen, 2006; Raikes, Summers, & Roggman, 2005; Roggman, Boyce, Cook, & Cook, 2002; Spoth & Redmond, 1993; Spoth, Redmond, Hockaday, & Shin, 1996).
Research on Father Involvement in Early Childhood Home-Visitation Programs
Rates of Attendance
The early childhood home-visitation literature has limited studies that address the proportion of fathers who participated in the intervention (i.e., percent of participation), how frequently fathers attended intervention sessions (i.e., rates of attendance), and factors associated with greater and lesser amounts of father participation (i.e., predictors) (Duggan et al., 2004; Smith et al., 2012). Studying baseline participation, levels of attendance, and factors that predict greater program participation during intervention delivery is an important step prior to picking points of entry to retool interventions to increase father participation (McCurdy & Daro, 2001; Spoth, Redmond, Kahn, & Shin, 1997).
The Smith et al. (2012) review of father involvement in maltreatment prevention programs (Not all were early childhood home-visiting interventions.) found considerable variability in rates of paternal participation, but the majority of studies reviewed (i.e., 12 of 17) reported 30% participation or less (range = 3–27%). By contrast, father participation in the Early Head Start home-visiting program was 32% (Raikes et al., 2005), 50% participation was reported during the Hawaii Healthy Start trial (Duggan et al., 2004), and unpublished data from the Nurse-Family Partnership (NFP) trial in Denver, Colorado recorded father participation at 58% (Holmberg & Olds, 2008). Some pilot programs and program improvement efforts focused on increasing father involvement have reported participation rates of 85% (Cornille, Barlow, & Cleveland, 2005; Guterman, 2012; Heinicke et al., 2000). Consistent operational definitions and methods for studying father participation across programs is a topic that deserves attention as this work moves forward.
Frequency of Father Program Attendance
Duggan et al. (2004) were one of the first groups to report on paternal attendance in home visitin,g and Hawaii Healthy Start Program fathers attended an average 2.4 (4.7) of the families' 13.6 (12.3) home visits during the first program year (i.e., child age 12 months). The NFP reported that during the trial in Denver, fathers participated in an average of 0.7 (0.1) of the mothers' 6.5 (2.8) prenatal home visits and 1.5 (0.2) of the mothers' 21.3 (1.0) infancy home visits (Korfmacher, O'Brien, Hiatt, & Olds, 1999).
Predictors of Father Engagement and Participation
Predictors of father home-visit engagement in the Hawaii trial included parent cohabitation and the frequency of parent contact at baseline, but the direction and magnitude of effects differed depending on the parents' relationship status at intake (Duggan et al., 2004). Among cohabiting couples, lower father participation was associated with father employment, greater domestic violence, and heavy alcohol use. Among noncohabiting couples who maintained frequent contact at intake, men's violence toward their romantic partners was associated with greater father participation. Among couples with low contact at intake, fathers attended very few visits, and their participation was not associated with any baseline variables (Duggan et al., 2004).
Given the small number of studies that have focused on rates and predictors of father participation in early childhood home-visitation programs, various methods have been used in studying father attendance in early childhood home visitation. Studies such as Duggan et al. (2004) have used home-visitor encounter data to report involvement for the full sample of participants. Other studies have used retrospective reports of father engagement based on surveys (e.g., Raikes et al., 2005; Roggman et al., 2002) or restricted analyses to subsamples of the families served, such as when fathers participated in other services (e.g., Wakabayashi, Guskin, Watson, McGilly, & Klinger, 2011).
Implementation, Organizational, and Program-Model Correlates of Father Attendance
Program-level factors associated with father attendance have included variables representing higher quality implementation and models or conditions where there is systematic outreach to fathers; each of which is associated with greater paternal involvement (Green, 2003; Raikes et al., 2005). Larson (1980) found that families starting home visitation in pregnancy, relative to families starting the intervention at child age 6 weeks and controls, had higher levels of father participation. Provider and organizational factors are known to relate to the quality of home visitation (Hicks, Larson, Nelson, Olds, & Johnston, 2008) and likely relate to paternal program attendance, but have not been previously studied in models that hold family-level characteristics constant (Fagan, 2007; McCurdy & Daro, 2001).
A frequently cited reason for why fathers do not participate in early childhood programs is that they face barriers to attending (e.g., work/school schedule, jobs with no paid time off) (Ghate, Shaw, & Hazel, 2000; Macleod, 2008; McAllister, Wilson, & Burton, 2004; Palm & Fagan, 2008). While home-visiting programs do attempt to reduce some of these barriers by reaching families in their homes, intervention models and implementing sites likely vary in the extent to which they make father involvement a priority. On the other hand, a particular challenge which may lead some programs, implementing sites, or providers to resist further father engagement relates to justifiable concerns about the possible damaging effects to children by facilitating the engagement of fathers who are antisocial or engage in intimate partner violence (Blazei et al., 2008; Duggan et al., 2004).
The NFP
Overview
The NFP is a program of prenatal and infancy home visitation by nurses for low-income, first-time mothers and their families. The NFP has been tested in three randomized controlled trials and since 1997 has been offered for public investment outside of research settings. Program participants enroll as early in pregnancy as possible, and home visits continue to child age 2 years (Olds, 2007).
Findings from randomized controlled trials of the NFP show replicated impacts on prenatal health, interpregnancy intervals, maternal employment, children's injuries, rates of marriage, father availability, and family reliance on public assistance (Olds, 2007). Replicated program impacts on child functioning include reduced behavior problems and increased cognitive and language abilities through school entry, especially among children born to mothers with fewer psychological resources to cope with living in poverty (Olds, 2007).
Dissemination of the NFP in communities, outside of the research trials, began in 1996. In this context, implementation is conducted with considerable effort to ensure service delivery with fidelity to the model tested in the trials (Olds, Hill, O'Brien, & Racine, 2003). Responsibility for community replication rests with the NFP's National Service Office, which provides site development, nurse professional training, fidelity monitoring, and quality assurance consultation to ensure that families benefit from the community-based program in ways similar to those who were enrolled in the randomized trials (Olds, 2002).
NFP community-replication fidelity monitoring
In the NFP, nurses collect information about participants at regular intervals and record features of each home visit using a standardized encounter form. At registration and every 6 months' postpartum, nurses collect information on participant mothers' demographic and relationship characteristics (i.e., marital and romantic partner status, cohabitation, etc.). After each home visit, nurses record who attended, what curriculum content was addressed (i.e., Personal Health, Environmental Health, Life Course, Maternal Role/Parenting, Friends and Family), and rate participants' levels of engagement, understanding, and conflict with the material covered. Data such as visit completion rates and demographics of families served are regularly analyzed while other aspects such as quality of engagement have not been as thoroughly evaluated. This information is later entered into a Web-based Client Information System (CIS) by office staff and securely uploaded to the NFP National Service Office for analysis. Data items collected on participants and program implementation in the community CIS are nearly identical to the corresponding data gathered in the trials (Korfmacher et al., 1999). These integrated data-collection efforts allow for quantified monitoring of services delivered and for comparisons to intervention-delivery data from the trials to ensure fidelity to the model tested in the trials. NFP encounter forms also provide a sensitive and reliable accounting of actual participant engagement (including fathers).
Father involvement in the NFP program model
As articulated in the initial description of the program model (Olds, 1980) and augmented in later trials, NFP nurses are trained to encourage mothers to invite fathers to home visits and attempt to schedule sessions when fathers can attend. Nurses follow the mother's lead in determining how often fathers attend, based in part on the degree to which the mother believes her relationship with the father can be healthy for her and her baby. Fathers are especially encouraged to join exercises that engage parents in discussions about family goals, positive communication skills, healthy relationships, and sharing parenting responsibilities. The goals of these exercises are learning sensitive caregiving, finding ways to increase social support and healthy communication, and developing strategies to decrease stress and conflict (Olds, 1980). Fathers, especially those who cannot attend particular home visits, are provided materials with father-friendly content (i.e., Dad's Days handouts) at regular intervals throughout the intervention (e.g., monthly in infancy).
Nurses are prompted to routinely assess intimate partner violence at different points in the intervention and support mothers in coping with domestic violence by developing safety plans and distancing themselves from dangerous men (Olds, 2002). In part because domestic violence was found to moderate the program's impact on child abuse (Eckenrode et al., 2000), recent program-improvement efforts have sought to improve assessment of intimate partner violence and elaborate strategies that nurses can use to help mothers address these issues (Donelan-McCall, Eckenrode, & Olds, 2009; Jack et al., 2012; Olds et al., 2013).
Community-based NFP father-involvement initiatives
NFP sites across the country have added fatherhood services to the NFP model by cultivating multi-agency collaborations (e.g., fatherhood programs) or developing within-site service augmentations (e.g., mental health, intimate partner violence, breast-feeding). While significant NFP program augmentations require careful iterative development and testing (Olds et al., 2013), a number of the sites have initiated efforts to increase father involvement by offering relatively simple program extensions (e.g., hosting family cookouts, offering resource fairs, partnering with other agencies in the community) or initiating additional services. Agencies such as the organization delivering NFP services in the Bronx, New York also offers the Bronx Fatherhood Program (http://www.vnsny.org/our-services/by-location/bronx). The Guilford Child Development Center in North Carolina has obtained funding to support a fatherhood caseworker and a healthy relationship class facilitator who split time between supporting families in the NFP and families enrolled in Early Head Start and Head Start (C.R. Britt, personal communication, August 15, 2006). Further, individual sites have allowed nurses to develop supplemental fatherhood materials as part of continuing their own graduate-level education (Kollowa, 2005).
NFP trials process and outcome data related to fathers
During the NFP trial in Denver, there were three arms in the study design: a comparison condition, a NFP nurse home-visitation condition, and a paraprofessional home-visitation condition. The paraprofessional-delivered intervention used an adapted version of the NFP program model (Olds, 2007). Nurses completed significantly more home visits with fathers in attendance than did para-professional home visitors (Korfmacher et al., 1999). Data from across the NFP trials also showed that nurse-visited families had increased rates of marriage, father cohabitation, and longer persisting parental romantic ties, as compared to families randomized to the control condition (Olds, 2007).
Father home-visit participation in the NFP trials and community replication
An unpublished report comparing father-visit participation in the Memphis, Tennessee and Denver trials, and from community replication sites has found that father-visit participation was slightly higher in community replication and the Denver trial than that observed in Memphis, even after statistically controlling for differences in the characteristics of populations served and the number of visits completed with mothers (Holmberg & Olds, 2008). Specifically, there were 1.4 (0.27) paternal visits for the Memphis trial versus 2.2 (0.27) for the Denver trial and 2.4 (0.02) paternal visits attended in community replication versus; that is, Memphis versus Denver, p = .03, effect size = .29; Memphis versus Community, p < .001, effect size = .24. While these differences are small and the sample sizes vary greatly, these results suggest that the NFP is doing at least as well in engaging fathers in community-replication sites as it did in the original trials.
Research Questions
This study sought to identify influential factors in father home-visit participation in community replication. We examined the extent to which father-visit participation was predicted by specific population characteristics, features of program implementation, and nurses and sites as random effects in 80 NFP community-replication sites. To accomplish the study, we addressed two questions:
RQ1: What are the predictors of father home-visit attendance in community-replication sites?
Based on results from earlier analyses conducted on the Denver trial (Holmberg & Olds, 2008) and correlates of father attendance in studies of other home-visitation programs (e.g., Duggan et al., 2004; Raikes et al., 2005; Roggman et al., 2002), we hypothesized that the count of father home-visit attendance would be predicted by the number of home visits completed with the mother, mothers' age (i.e., over 18 years), maternal White race, being married, frequent contact with the biological father, the mother identifying the biological father as her romantic partner, and mother's cohabitation with her partner. We further hypothesized that earlier program enrollment (i.e., gestational age at program initiation) may give nurses more time to engage fathers in the intervention and relate to higher father participation. We hypothesized that intimate partner violence would relate to reduced father involvement, in part due to the guidance provided to nurses around helping mothers develop a safe distance from dangerous partners. We also hypothesized that nurses with greater experience would be more mature and have greater comfort integrating fathers into home visits and thus relate to higher paternal program participation. We hypothesized that random effects for sites and nurses would be strongly associated with father home-visit attendance, due to differences in implementing agencies varying emphasis to this aspect of the program model. Nurse race/ethnicity was added to account for part of the hypothesized random effect for nurse, but no a priori hypotheses were made as to the magnitude of that influence.
RQ2: How varied is average father home-visit participation among sites, after statistical adjustment to control for differences among sites in maternal and family characteristics and for the random effect of nurses?
Method
Samples
As seen in Table 1, we analyzed home-visit implementation in 80 community-replication sites, which included 694 nurses and 29,109 families enrolled in the program between 1996 and 2007. In each of these sites, data were analyzed on all cases with a live birth and an index child age of greater than 12 months. Sites were located in 19 states across the continental United States (i.e., 31 sites were located in the West, 15 in the Midwest, 5 in the South, and 29 in the Northeast). All samples were comprised of young (i.e., mean maternal age = 19 years), low-income parents in which the mother had no previous live birth. Analyses for these studies were approved by the Colorado Multiple Institutional Review Board.
Table 1. Sociodemographic Characteristics of Community-Enrolled Nurse-Family Project Participants and Frequency of Home Visits Completed.
| Population of Participants (N = 29,109) | Individual Sites (N = 80) | ||
|---|---|---|---|
|
|
|
||
| M (SD) | Range | Range of Ms (SD) | |
| Participant Characteristics | |||
| Maternal Age (years) | 19.2 (3.9) | 10.0–44.0 | 17.0 (2.4)–23.6 (4.9) |
| %Maternal Age ≤18 Years | 51.2 (49.9) | 9.5 (29.4)–82.6 (38.0) | |
| Maternal Education (years) | 10.6 (1.7) | 2–13 | 9.4 (2.0)–11.4 (0.9) |
| Maternal Race/Ethnicity | |||
| %African American | 23.6 (42.5) | 0.0 (0.0)–91.9 (27.5) | |
| %White | 38.6 (48.7) | 0.0 (0.0)–95.0 (21.9) | |
| %Hispanic | 27.0 (44.4) | 0.0 (0.0)–81.3 (39.1) | |
| %Married | 12.4 (32.9) | 0.0 (0.0)–34.3 (47.5) | |
| %Mother Has a Romantic Partner | 77.5 (41.8) | 62.2 (48.7)–92.5 (26.7) | |
| %Partner Is the Biological Father | 92.5 (26.4) | 82.0 (38.4)–98.5 (12.5) | |
| %Mother Lives With Partner | 37.0 (48.3) | 15.8 (37.5)–69.4 (46.2) | |
| %Mother Lives With Parent(s) | 37.7 (48.5) | 10.5 (30.8)–54.8 (50.0) | |
| Contact With Biological Father | 10.0 (1.0) | 7.8–10.6 | 9.6 (1.3)–10.3 (0.8) |
| Gestational Age at Registration | 19.6 (7.0) | 0.0–40.0 | 16.7 (6.4)– 22.1 (6.6) |
| %History of a Mental Health Condition | 7.0 (25.8) | 0.0 (0.0)–25.4 (43.7) | |
| %Hurt by Partner Since Pregnant | 7.2 (25.9) | 0.0 (0.0)–13.5 (34.3) | |
| %Afraid of Any Partner | 6.8 (25.2) | 0.0 (0.0)–13.3 (31.6) | |
| Nurse Characteristics | |||
| Nurse Practice Experience (years) | 15.6 (9.1) | 0.0–30.0 | 4.9 (6.7)–26.5 (3.5) |
| %Nurse Race/Ethnicity White | 75.7 (42.9) | 0.0 (0.0)–100 (0.0) | |
| Home Visits Attendedb | |||
| Mother | 21.1 (11.7)c | 1.0–47.0 | 14.1 (8.9)c–26.5 (11.7)c |
| Father | 2.4 (4.3)c | 0.0–32.0 | 0.4 (1.0)c–5.2 (6.3)c |
Participants enrolled in dissemination sites between 1996 and 2006.
Registration to child age 12 months.
Adjusted for gestational age at registration.
Sources of Information and Variables
Data sources
Data were derived from the NFP CIS, which provides information on family sociodemographic characteristics and what occurred at home visits. No information was collected from individual fathers. The community CIS dataset used for this study represents family participation in nearly all sites operating through 2006. The exception was that data were not available for one state-based implementation site that has its own management information system.
Variables
Variables were created across each of the samples to represent the following sociodemographic characteristics measured at registration during pregnancy: (a) mother's age in years; (b) percent of teen mothers (i.e., ≤18 years vs. older); (c) mother's years of education completed; (d) maternal self-reported race/ethnicity; (e) maternal marital status (legally married vs. not); (f) whether the child's biological father was the mother's current romantic partner; and (g) whether the mother was cohabiting with her partner, her parent, or neither. Variables also were created to characterize how often the mother had seen the father of the child in the week preceding registration; estimated gestational age at registration; whether the mother reported ever experiencing a mental health disorder; whether she had been injured by intimate partner violence during pregnancy; and whether she was afraid of any previous partner. In addition, nurse-level variables were created to represent individual nurse experience in nursing (years) and race/ethnicity (White/other).
Variables representing the count of home visits attended were calculated separately for mothers and fathers from intake through child age 12 months. To reduce the influence of outliers, the count of mother's visits was truncated for mothers at 47 visits and fathers at 32 visits (Dixon & Tukey, 1968).
The CIS did not systematically track background information about the biological father or nonbiological, social fathers who attended home visits and filled a parental role (Gavazzi & Schock, 2004). We describe both types of male caregivers as the “father” for purposes of this article. The count of home visits attended by fathers during pregnancy and the first year of the child's life served as the dependent variable.
Statistical Analyses
To address RQ1, we first used semipartial bivariate regression analyses (i.e., controlling for maternal home visits completed, gestational age at registration, and sites and nurses as random effects) to identify predictors of father home-visit attendance from the list of potential predictors. We then entered all of the significant re-gressors into a backward stepwise regression analysis to identify a final parsimonious model representing the unique predictors of father-visit attendance. Variables entered the list of predictors if the semipartial bivariate regression p value was <.0001 and were retained if, after controlling for other variables, the variable remained significant at p < .0001.
We addressed RQ2 using a generalized linear mixed model that regressed father-visit participation on sites (as a fixed effect) while introducing statistical controls for nurses as random effects and maternal age, White race/ethnicity, marriage, and cohabitation with the partner as fixed effects. We plotted means and SEs for the 80 sites to illustrate the variation found among sites after statistical control for covariates. Random and fixed estimations of the site effects were nearly identical for both fixed and random assumptions.
Results
Table 1 displays the univariate statistics for each of the study variables in the sample overall and the range of means and SDs at individual sites. Table 2 displays the significant (p < .0001) semi-partial regression coefficients for the predictors of father home-visit attendance in community-replication sites. Table 3 shows those regressors that remained significant after the backward stepwise regression analyses. Specifically, the final model included the number of maternal visits, B = 0.12, SE = 0.01, F = 3101.77, frequency of contact with the child's biological father, B = 0.61, SE = 0.02, F = 708.02, maternal cohabitation with the father, B = 1.41, SE = 0.07, F = 631.51, maternal White race, B = 0.77, SE = 0.06, F = 190.12, and being married, B = 0.42, SE = 0.08, F = 30.08. The variance accounted for by the random effects for sites and nurses within sites was attenuated when the other variables were entered into the model, but remained highly significant and accounted for a large portion of the variance (i.e., 2.7 and 6.7%, respectively).
Table 2. Predictors of father-visit participation: community sample.
| Fixed Effects | B | SE B | F |
|---|---|---|---|
| Intervention Process | |||
| Maternal Home Visits—Overall | 0.12 | <0.01 | 3245.87* |
| Maternal Demographic Status | |||
| Age ≤18 Years | −0.35 | 0.05 | 52.79* |
| Education | 0.12 | 0.01 | 74.85* |
| Race/Ethnicity | |||
| African American | −0.94 | 0.07 | 196.52* |
| White | 0.91 | 0.06 | 266.57* |
| Hispanic | −0.50 | 0.07 | 57.52* |
| Gestational Age at Enrollment | −0.02 | <0.01 | 20.0* |
| History Mental Health Condition | 0.33 | 0.09 | 12.96* |
| Maternal & Couple Functioning | |||
| Marital Status | 1.58 | 0.07 | 481.48* |
| Partner Is Biological Father | 1.96 | 0.05 | 1553.34* |
| Cohabitation With Child's Father | 2.13 | 0.05 | 2040.28* |
| Cohabitation With Parents | −1.28 | 0.05 | 721.38* |
| How Often See Biological Father | 0.90 | 0.02 | 1786.08* |
| Hurt by Partner Since Pregnant | −0.63 | 0.11 | 35.31* |
| Afraid of Partner | −0.10 | 0.01 | 71.73* |
| Provider | |||
| Nurse Experience (years) | 0.01 | <0.01 | 0.03* |
| Nurse Race/Ethnicity (White/Other) | 0.40 | 0.12 | 11.00* |
|
| |||
| Provider & Site Random Effects | Variance | SE | |
|
| |||
| Nursesa | 1.31 | 0.10 | – |
| Sitesa | 0.92 | 0.19 | – |
Note. All analyses control statistically for gestational age at registration, count of maternal visits completed, and random effects for sites and nurses within sites.
Random effect.
p < .0001.
Table 3. Unique Predictors of Father-Visit Participation in the Community Sample (n = 27,685).
| B | SE B | F | |
|---|---|---|---|
| Fixed Effects | |||
| Maternal Visits to Child Age 12 Months | 0.12 | <0.01 | 3101.77* |
| Frequently Saw Biological Father | 0.61 | 0.02 | 708.02* |
| Cohabitation With Father | 1.41 | 0.07 | 631.51* |
| Maternal White Race/Ethnicity | 0.77 | 0.06 | 190.12* |
| Married | 0.42 | 0.08 | 30.08* |
|
| |||
| Random Effects | Variance | SE | %Variance Accounted For |
|
| |||
| Nurses Within Sites | 1.01 | 0.08 | 6.7* |
| Sites | 0.41 | 0.10 | 2.7* |
p < .0001.
Figure 1 illustrates this substantial variation in average father home-visit participation among sites, adjusting for differences in populations served, implementation, and variation attributable to individual nurses. The median site averaged 2.25 visits with fathers from pregnancy through child age 12 months. Across sites, after demographic characteristics were adjusted, mean father home-visit attendance ranged from 0.13 to 4.35 visits per family.
Figure 1.
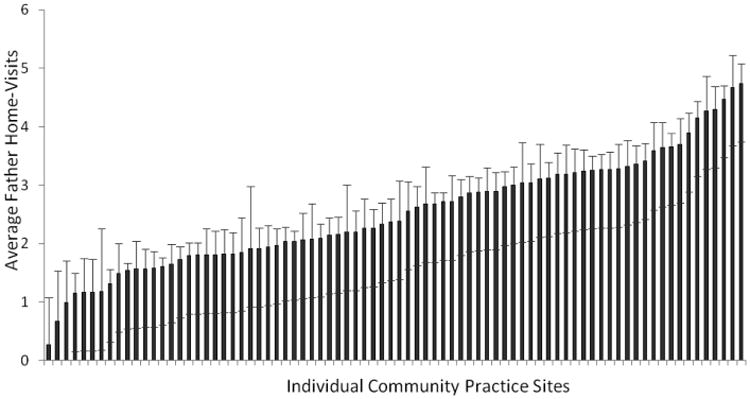
Population-adjusted average father home-visit participation at replication sites. For ease of generating this figure, sites were added to the final model as fixed effects; covariates included count of mother visits, maternal cohabitation with the father, mother's contact with the father at registration, maternal race/ethnicity, being married, and a random effect of individual nurses within sites.
Discussion
Father home-visit participation was associated with maternal and family sociodemographic characteristics such as the number of maternal home visits completed; maternal cohabitation with a partner; mother's frequent contact with the biological father in the week prior to program registration; maternal White, non-Hispanic race; and being married. Even after statistical adjustments controlled for differences in the sociodemographic characteristics of the populations served, the random effects of nurses and sites accounted for large effects. Although NFP sites and nurses all delivered the same program model and were continuously monitored for fidelity, there was considerable variation in sites' average father home-visit participation.
This study was unique in several ways. First, the visit-by-visit recording of intervention delivery by nurse home visitors provided a complete accounting of actual father participation. Previous studies have been limited by the use of dichotomous variables that represented father involvement as none or engagement in one or more activities (Fagan, 1999; Raikes et al., 2005; Roggman et al., 2002), and some have reported using retrospective report of father participation based on staff and participant interviews and surveys (Raikes et al., 2005; Roggman et al., 2002). Second, the simultaneous collection of information on family sociodemographic characteristics, nurses, and sites allowed us to identify the magnitude of multiple levels of influence on father home-visit attendance.
There were important limitations to our study. Foremost is the correlational nature of the analyses, which limits attribution of causality. Data collected on family sociodemographic circumstances, for example, were restricted. We would have liked to be able to contrast participation by biological fathers and subsequent maternal partners (i.e., social fathers), but the CIS did not distinguish them. While potentially interesting data have been collected in the CIS to represent the qualitative ratings by nurses after visits (e.g., participant engagement and learning), the foundational psychometric work has not yet been completed on those variables to justify and interpret analyses contrasting visits with mother-alone visits versus those where mothers and fathers attend together. There also was limited information about the mothers served, such as the quality of the parents' relationships. It has become increasingly evident in the literature that mothers encourage greater involvement by fathers who have greater relationship potential and social resources (Waller & Swisher, 2006). Similarly, fathers with greater social and personal resources are more involved with their child's developmental and educational programming (Duursma, Pan, & Raikes, 2008; Roggman et al., 2002). Knowing more about fathers' personal resources would have been helpful.
Father participation in NFP home visits has been low relative to that of mothers (i.e., roughly 1 paternal visit for every 10 maternal visits), but there is evidence that paternal involvement increased after the trial in Memphis, as seen in the Denver trial and community replication (Holmberg & Olds, 2008). The modest, but significant, increase in father home-visit participation likely resulted from the purposeful focus on increasing paternal involvement and the creation of additional paternal-role content prior at the start of the Denver trial (Olds, Kitzman, Cole, & Robinson, 1997). The relative increase in participation by fathers also may relate to changing social trends regarding fathers spending more time caring for their children (Sullivan, Coltrane, Mcannally, & Altintas, 2009; Yeung, Sandberg, Davis-Kean, & Hofferth, 2001) and the increased availability of social programs to support fathers around care for their young children (Palm & Fagan, 2008).
Many of the maternal and family sociodemographic factors found to predict father home-visit participation replicate findings from other studies of paternal participation in early childhood programs (Fagan, 1999; Raikes et al., 2005; Roggman et al., 2002) and studies of father involvement with caregiving (Gavin et al., 2002; Kalil, Ziol-Guest, & Levine-Coley, 2005; Rhein et al., 1997; Roye & Balk, 1996). The maternal and family characteristics predictive of paternal program participation represent two broad factors: (a) maternal personal resources (e.g., being old enough to cohabi-tate or be married, greater program engagement) and (b) relationship quality/investment in the partner (i.e., cohabitation, frequent contact with the biological father partner, being married). From these findings, important questions emerge: To what degree are these family-level influences malleable? Could program-mediated changes in these factors (e.g., relationship quality) result in increased father program participation (e.g., during the latter part of the program)?
The additional sociodemographic predictor retained in our final multivariate model, one that has not received as much attention in the literature, was maternal race/ethnicity. With the data available in the CIS, it is not clear why large differences by race/ethnicity continue to be evident after other sociodemographic characteristics (e.g., home visits completed, contact with partner prior to registration, marriage and cohabitation) were held constant. Studies often have found that differences in father–child engagement by race/ethnicity are better accounted for by structural influences (e.g., marriage, cohabitation, multigenerational households) (e.g., Cabrera, Ryan, Mitchell, Shannon, & Tamis-LeMonda, 2008) and that many other factors are interrelated with race/ethnicity (Lu et al., 2010).
One important null finding also warrants brief discussion. In the NFP community-based sample, seen in Table 2, the semipar-tial regression coefficients for intimate partner violence variables were significant and negatively associated with father home-visit attendance. Those variables were not retained in the final model, presented in Table 3, suggesting a lack of association between intimate partner violence variables and father home-visit attendance. There are justifiable concerns about a program encouraging involvement by violent and antisocial men (Duggan et al., 2004). The lack of association seen in these analyses may reflect the program's standard guidance from nurses to help mothers make safe decisions for themselves around involvement with dangerous men. As was found in Early Head Start, higher risk men also may avoid involvement in social service programs (e.g., Roggman et al., 2002). Of course, underreporting of intimate partner violence, especially in the context of face-to-face interview assessment strategies (e.g., MacMillan et al., 2009) also may have influenced our ability to detect an association.
Provider and organizational factors have been postulated to be important factors in father program involvement (Fagan, 2007; Korfmacher et al., 2008; McCurdy & Daro, 2001). Agencies that emphasize and dedicate resources to father engagement have found greater paternal involvement (Fagan, 1999; Raikes et al., 2005). Our study found that, together, nurses and sites accounted for more than 9% of the variation in father participation. One might expect that site effects would be the stronger influence. As described earlier, some NFP sites have developed collaborations, augmentations, and strategies to further engage fathers. Our findings showed that variation at the level of the nurses was more than three times as influential as that for sites. We did assess the degree to which some individual nurse characteristics (i.e., age, race/ethnicity) and professional experience (i.e., years in nursing, maternal–child experience) related to father participation, but the effects were small and not retained in the final model.
Developing a better understanding of what accounts for differences among nurses (e.g., the ability to remain interpersonally available to the mother and father in the same visit, attitudes about the role of fathers in the program, skill in advocating for father involvement, comfort in working with fathers) will be important next steps for research in this area. Studying sites with relatively high and low adjusted father participation, as seen in Figure 1, using mixed (i.e., qualitative and quantitative) methodologies may elucidate what policies, strategies, beliefs, content, or training account for the large differences observed.
Father participation in early childhood parenting programs is associated with improved father–child engagement and maternal and child health and development (Bagner & Eyberg, 2003; Fagan, 2007; Lundahl et al., 2008; Raikes et al., 2005). These findings suggest that the beneficial effects of the NFP and other home-visitation programs could be bolstered by increased focus on healthy father participation.
Conclusion
Father home-visit participation in the NFP is infrequent relative to that of mothers. Maternal personal resources and indicators of the quality of the parents' relationship predicted greater paternal involvement. The relatively large portions of variance explained by sites and nurses in predicting father participation suggest that organizational, team, and nurse factors need to be understood more completely, and are promising targets of intervention for increasing safe, nurturing father involvement in home visits.
Acknowledgments
This article was supported in part by Grant 5T32MH015442, an institutional NRSA Postdoctoral Research Training Program, for Dr. John Holmberg. We thank Maureen McClatchy for her assistance with the data files, Mike Knudtson for his statistical consultation, the NFP National Service Office for allowing us to access the data for the analyses presented, and the families who participated in the program. The Prevention Research Center for Family and Child Health (PRC), directed by Dr. Olds at the University of Colorado School of Medicine, provides a royalty free license to the Nurse Family Partnership National Service Office, established in the US to implement the NFP with fidelity to the model's core elements; it has a contract with the NFP to conduct research to improve the NFP program and its implementation. Dr. Olds is employed by this center. Dr. Olds is the founder of the NFP. The PRC also has license agreements with other societies to develop and conduct the program with fidelity to the NFP program model, and consultancy agreements with other governments and entities to support the implementation of the NFP. Revenue generated from these agreements is placed into a pool of funds at the PRC to support research on improving the NFP program model. None of these revenues is used to augment individuals' University salaries.
References
- Amato PR, Rivera F. Paternal involvement and children's behavior problems. Journal of Marriage and Family. 1999;61(2):375–384. [Google Scholar]
- Bagner DM, Eyberg SM. Father involvement in parent training: When does it matter? Journal of Clinical Child & Adolescent Psychology. 2003;32(4):599–605. doi: 10.1207/S15374424JCCP3204_13. [DOI] [PubMed] [Google Scholar]
- Bakermans-Kranenburg MJ, van IJzendoorn MH, Juffer F. Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin. 2003;129:195–215. doi: 10.1037/0033-2909.129.2.195. [DOI] [PubMed] [Google Scholar]
- Blazei RW, Iacono WG, McGue M. Father-child transmission of antisocial behavior: The moderating role of father's presence in the home. Journal of the American Academy of Child & Adolescent Psychiatry. 2008;47(4):406–415. doi: 10.1097/CHI.0b013e3181642979. [DOI] [PubMed] [Google Scholar]
- Braver SL, Wolchik SA, Sandler IN, Sheets VL, Fogas B, Bay RC. A longitudinal study of noncustodial parents: Parents without children. Journal of Family Psychology. 1993;7(1):9–23. [Google Scholar]
- Bronstein P, Stoll MF, Clauson J, Abrams CL, Briones M. Fathering after separation or divorce: Factors predicting children's adjustment. Family Relations. 1994;43(4):469–479. [Google Scholar]
- Bronte-Tinkew J, Carrano J, Horowitz A, Kinukawa A. Involvement among resident fathers and links to infant cognitive outcomes. Journal of Family Issues. 2008;29(9):1211–1244. [Google Scholar]
- Bugental DB. Finding ways to reduce the prevalence of child maltreatment among fathers: A comment on the alternative approaches. Clinical Psychology: Science and Practice. 2004;11:112–115. [Google Scholar]
- Bzostek SH. Social fathers and child well-being. Journal of Marriage and Family. 2008;70(4):950–961. [Google Scholar]
- Cabrera NJ, Ryan RM, Mitchell SJ, Shannon JD, Tamis-LeMonda CS. Low-income nonresident father involvement with their toddlers: Variation by fathers' race and ethnicity. Journal of Family Psychology. 2008;22(4):643–647. doi: 10.1037/0893-3200.22.3.643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson M, McLanahan S, England P. Union formation in fragile families. Demography. 2004;41(2):237–261. doi: 10.1353/dem.2004.0012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cowan PA, Cowan CP, Pruett MK, Pruett K, Wong JJ. Promoting fathers' engagement with children: Preventive interventions for low-income families. Journal of Marriage and Family. 2009;71:663–679. [Google Scholar]
- Cornille TA, Barlow LO, Cleveland AD. DADS Family Project: An experiential group approach to support fathers in their relationship with their children. Social Work with Groups. 2005;28(2):41–57. [Google Scholar]
- Dixon WJ, Tukey JW. Approximate behavior of the distribution of Winsorized T (Trimming/Winsorization 2) Technometrics. 1968;10(1):83–98. [Google Scholar]
- Donelan-McCall N, Eckenrode J, Olds DL. Home visiting for the prevention of child maltreatment: Lessons learned during the past 20 years. Pediatric Clinics of North America. 2009;56(2):389–403. doi: 10.1016/j.pcl.2009.01.002. [DOI] [PubMed] [Google Scholar]
- Dubowitz H, Black MM, Cox CE, Kerr MA, Litrownik AJ, Rad-hakrishna A, et al. Father involvement and children's functioning at age 6 years: A multisite study. Child Maltreatment. 2001;6(4):300–309. doi: 10.1177/1077559501006004003. [DOI] [PubMed] [Google Scholar]
- Duggan A, Fuddy L, McFarlane E, Burrell L, Windham A, Hig-man S, et al. Evaluating a statewide home visiting program to prevent child abuse in at-risk families of newborns: Fathers' participation and outcomes. Child Maltreatment. 2004;9(1):3–17. doi: 10.1177/1077559503261336. [DOI] [PubMed] [Google Scholar]
- Duursma E, Pan BA, Raikes H. Predictors and outcomes of low-income fathers' reading with their toddlers. Early Childhood Research Quarterly. 2008;23(3):351–365. [Google Scholar]
- Eckenrode J, Ganzel B, Henderson CR, Jr, Smith E, Olds DL, Powers J, et al. Preventing child abuse and neglect with a program of nurse home visitation: The limiting effects of domestic violence. Journal of the American Medical Association. 2000;284(11):1385–1391. doi: 10.1001/jama.284.11.1385. [DOI] [PubMed] [Google Scholar]
- Fagan J. Predictors of father and father figure involvement in pre-Kindergarten Head Start. Philadelphia: National Center on Fathers and Families; 1999. [Google Scholar]
- Fagan J. Research on children's environmental programmatic efforts pertaining to fatherhood. Applied Developmental Science. 2007;11(4):260–265. [Google Scholar]
- Gavazzi S, Schock A. A multi-method study of father participation in family-based programming. In: Day RD, Lamb ME, editors. Conceptualizing and measuring father involvement. Mahwah, NJ: Erlbaum; 2004. pp. 149–184. [Google Scholar]
- Gavidia-Payne S, Stoneman Z. Family predictors of maternal and paternal involvement in programs for young children with disabilities. Child Development. 1997;68(4):701–717. [PubMed] [Google Scholar]
- Gavin LE, Black MM, Minor S, Abel Y, Papas MA, Bentley ME. Young, disadvantaged fathers' involvement with their infants: An ecological perspective. Journal of Adolescent Health. 2002;31(3):266–276. doi: 10.1016/s1054-139x(02)00366-x. [DOI] [PubMed] [Google Scholar]
- Ghate D, Shaw C, Hazel N. Fathers at the centre: Family centres, fathers and working with men. London: Policy Research Bureau; 2000. [Google Scholar]
- Green S. Reaching out to fathers: An examination of staff efforts that lead to greater father involvement in early childhood programs. Early Childhood Research & Practice. 2003;5(2) [Google Scholar]
- Guterman N. Promoting father involvement in home visiting services for vulnerable families: A pilot study. Pew Center on the States. 2012 doi: 10.1016/j.chiabu.2017.10.017. Available at: http://www.pewtrusts.org/∼/media/legacy/uploadedfiles/pcs_assets/2013/FatherInvolvementexecutivesummarypdf.pdf. [DOI] [PubMed]
- Hahlweg K, Heinrichs N, Kuschel A, Bertram H, Naumann S. Long-term outcome of a randomized controlled universal prevention trial through a positive parenting program: Is it worth the effort? Child and Adolescent Psychiatry and Mental Health. 2010;4(1):14. doi: 10.1186/1753-2000-4-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinicke CM, Goorsky M, Moscov S, Dudley K, Gordon J, Schneider C, Guthrie D. Relationship-based intervention with at-risk mothers: Factors affecting variations in outcome. Infant Mental Health Journal. 2000;21(3):133–155. [Google Scholar]
- Hicks D, Larson C, Nelson C, Olds DL, Johnston E. The influence of collaboration on program outcomes in the Colorado Nurse-Family Partnership. Evaluation Review. 2008;32(5):453–477. doi: 10.1177/0193841X08315131. [DOI] [PubMed] [Google Scholar]
- Holmberg JR, Olds DL. Thinking about fathers in the Nurse Family Partnership program. Paper presented at the annual conference for the Society for Prevention Research; San Francisco. 2008. May, [Google Scholar]
- Jack SM, Ford-Gilboe M, Wathen CN, Davidov DM, McNaughton DB, Coben JH, et al. Development of a nurse home visitation intervention for intimate partner violence. BMC: Health Services Research. 2012;12(1):50. doi: 10.1186/1472-6963-12-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaffee SR, Moffitt TE, Caspi A, Taylor A. Life with (or without) father: The benefits of living with two biological parents depend on the father's antisocial behavior. Child Development. 2003;74(1):109–126. doi: 10.1111/1467-8624.t01-1-00524. [DOI] [PubMed] [Google Scholar]
- Jayakody R, Kalil A. Social fathering in low-income, African American families with preschool children. Journal of Marriage and Family. 2002;64(2):504–516. [Google Scholar]
- Kalil A, Ziol-Guest KM, Levine-Coley R. Perceptions of father involvement patterns in teenage-mother families: Predictors and links to mothers' psychological adjustment. Family Relations. 2005;54(2):197–211. [Google Scholar]
- Kane P, Garber J. The relations among depression in fathers, children's psychopathology, and father–child conflict: A meta-analysis. Clinical Psychology Review. 2004;24(3):339–360. doi: 10.1016/j.cpr.2004.03.004. [DOI] [PubMed] [Google Scholar]
- Kollowa K. Father involvement lesson plan. Paper presented at the University of Phoenix; Lone Tree, CO. 2005. Sep, [Google Scholar]
- Korfmacher J, Green B, Staerkel F, Peterson C, Cook G, Roggman L, et al. Parent involvement in early childhood home visiting. Child & Youth Care Forum. 2008;37(4):171–196. [Google Scholar]
- Korfmacher J, O'Brien R, Hiatt S, Olds DL. Differences in program implementation between nurses and paraprofessionals providing home visits during pregnancy and infancy: A randomized trial. American Journal of Public Health. 1999;89(12):1847–1851. doi: 10.2105/ajph.89.12.1847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson CP. Efficacy of prenatal and postpartum home visits on child health and development. Pediatrics. 1980;66(2):191–197. [PubMed] [Google Scholar]
- Lengua LJ, Roosa MW, Schupak-Neuberg E, Michaels ML, Berg CN, Weschler LF. Using focus groups to guide the development of a parenting program for difficult-to-reach, high-risk families. Family Relations. 1992;41(2):163–168. [Google Scholar]
- Lu MC, Jones L, Bond MJ, Wright K, Pumpuang M, Maidenberg M, et al. Where is the F in MCH? Father involvement in African American families. Ethnicity & Disease. 2010;20:S2–49. [PubMed] [Google Scholar]
- Lundahl BW, Tollefson D, Risser H, Lovejoy MC. A meta-analysis of father involvement in parent training. Research on Social Work Practice. 2008;18(2):97–106. [Google Scholar]
- Macleod F. Why fathers are not attracted to family learning groups? Early Child Development and Care. 2008;178(7):773–783. [Google Scholar]
- MacMillan HL, Wathen CN, Jamieson E, Boyle MH, Shannon HS, Ford-Gilboe M, et al. Screening for intimate partner violence in health care settings: A randomized trial. Journal of the American Medical Association. 2009;302(5):493–501. doi: 10.1001/jama.2009.1089. [DOI] [PubMed] [Google Scholar]
- Marmorstein NR, Malone SM, Iacono WG. Psychiatric disorders among offspring of depressed mothers: Associations with paternal psychopathology. American Journal of Psychiatry. 2004;161(9):1588–1594. doi: 10.1176/appi.ajp.161.9.1588. [DOI] [PubMed] [Google Scholar]
- McAllister CL, Wilson PC, Burton J. From sports fans to nurturers: An Early Head Start Program's evolution toward father involvement. Fathering: A Journal of Theory, Research, & Practice about Men as Fathers. 2004;2(1):31–59. [Google Scholar]
- McCurdy K, Daro D. Parent involvement in family support programs: An integrated theory. Family Relations. 2001;50(2):113–121. [Google Scholar]
- Olds D, Donelan-McCall N, O'Brien R, MacMillan H, Jack S, Jenkins T, et al. Improving the Nurse–Family Partnership in community practice. Pediatrics. 2013;132(Suppl. 2):S110–S117. doi: 10.1542/peds.2013-1021I. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olds DL. Improving formal services for mothers and children. In: Belsky JSSH, editor. Protecting children from child abuse and neglect. San Francisco: Jossey-Bass; 1980. pp. 173–197. [Google Scholar]
- Olds DL. Prenatal and infancy home visiting by nurses: From randomized trials to community replication. Prevention Science. 2002;3(3):153–172. doi: 10.1023/a:1019990432161. [DOI] [PubMed] [Google Scholar]
- Olds DL. Preventing crime with prenatal and infancy support of parents: The Nurse-Family Partnership. Victims & Offenders. 2007;2(2):205–225. doi: 10.1080/14043850802450096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olds DL, Hill PL, O'Brien R, Racine DMP. Taking preventive intervention to scale: The nurse-family partnership. Cognitive and Behavioral Practice. 2003;10(4):278–290. [Google Scholar]
- Olds DL, Kitzman HJ, Cole R, Robinson J. Theoretical foundations of a program of home visitation for pregnant women and parents of young children. Journal of Community Psychology. 1997;25(1):9–25. [Google Scholar]
- Olds DL, Sadler L, Kitzman H. Programs for parents of infants and toddlers: Recent evidence from randomized trials. Journal of Child Psychology and Psychiatry. 2007;48(3–4):355–391. doi: 10.1111/j.1469-7610.2006.01702.x. [DOI] [PubMed] [Google Scholar]
- Palm G, Fagan J. Father involvement in early childhood programs: Review of the literature. Early Child Development and Care. 2008;178(7):745–759. [Google Scholar]
- Panter-Brick C, Burgess A, Eggerman M, McAllister F, Pruett K, Leckman JF. Practitioner Review: Engaging fathers— Recommendations for a game change in parenting interventions based on a systematic review of the global evidence. Journal of Child Psychology and Psychiatry. 2014;55(11):1187–1212. doi: 10.1111/jcpp.12280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raikes H, Green BL, Atwater J, Kisker E, Constantine J, Chazan-Cohen R. Involvement in Early Head Start home visiting services: Demographic predictors and relations to child and parent outcomes. Early Childhood Research Quarterly. 2006;21(1):2–24. [Google Scholar]
- Raikes H, Summers J, Roggman L. Father involvement in Early Head Start Programs. Fathering:A Journal of Theory, Research, and Practice about Men as Fathers. 2005;3(1):29–58. [Google Scholar]
- Rhein LM, Ginsburg KR, Schwarz DF, Pinto-Martin JA, Zhao H, Morgan AP, et al. Teen father participation in child rearing: Family perspectives. Journal of Adolescent Health. 1997;21(4):244–252. doi: 10.1016/S1054-139X(97)00115-8. [DOI] [PubMed] [Google Scholar]
- Roggman LA, Boyce LK, Cook GA, Cook J. Getting dads involved: Predictors of father involvement in Early Head Start and with their children. Infant Mental Health Journal. 2002;23(1–2):62–78. [Google Scholar]
- Roye CF, Balk SJ. The relationship of partner support to outcomes for teenage mothers and their children: A review. Journal of Adolescent Health. 1996;19(2):86–93. doi: 10.1016/1054-139X(95)00278-Z. [DOI] [PubMed] [Google Scholar]
- Ryan RM, Kalil A, Ziol-Guest KM. Longitudinal patterns of nonresident fathers' involvement: The role of resources and relations. Journal of Marriage and Family. 2008;70(4):962–977. [Google Scholar]
- Sar BK, Antle BF, Bledsoe LK, Barbee AP, Van Zyl MA. The importance of expanding home visitation services to include strengthening family relationships for the benefit of children. Children and Youth Services Review. 2010;32(2):198–205. [Google Scholar]
- Sarkadi A, Kristiansson R, Oberklaid F, Bremberg S. Fathers' involvement and children's developmental outcomes: A systematic review of longitudinal studies. Acta Pædiatrica. 2008;97(2):153–158. doi: 10.1111/j.1651-2227.2007.00572.x. [DOI] [PubMed] [Google Scholar]
- Smith TK, Duggan A, Bair-Merritt MH, Cox G. Systematic review of fathers' involvement in programmes for the primary prevention of child maltreatment. Child Abuse Review. 2012;21:237–254. [Google Scholar]
- Spoth R, Redmond C. Study of participation barriers in family-focused prevention: Research issues and preliminary results. International Quarterly of Community Health Education. 1993;13:365–388. doi: 10.2190/69LM-59KD-K9CE-8Y8B. [DOI] [PubMed] [Google Scholar]
- Spoth R, Redmond C, Hockaday C, Shin CY. Barriers to participation in family skills preventive interventions and their evaluations: A replication and extension. Family Relations. 1996;45(3):247–254. [Google Scholar]
- Spoth R, Redmond C, Kahn JH, Shin C. A prospective validation study of inclination, belief, and context predictors of family-focused prevention involvement. Family Process. 1997;36(4):403–429. doi: 10.1111/j.1545-5300.1997.00403.x. [DOI] [PubMed] [Google Scholar]
- Sullivan O, Coltrane S, Mcannally L, Altintas E. Father-friendly policies and time-use data in a cross-national context: Potential and prospects for future research. ANNALS of the American Academy of Political and Social Science. 2009;624(1):234–254. [Google Scholar]
- Wakabayashi T, Guskin KA, Watson J, McGilly K, Klinger LL., Jr The Parents as Teachers Promoting Responsible Fatherhood Project: Evaluation of “Dads in the Mix,” an exemplary site. 2011 Feb 25; Available at: http://www.parentsasteachers.org/images/stories/documents/Parents_as_Teachers_Fatherhood_Project_White_Paper.pdf.
- Waller MR, Swisher R. Fathers' risk factors in fragile families: Implications for “healthy” relationships and father involvement. Social Problems. 2006;53(3):392–420. [Google Scholar]
- White L, Gilbreth JG. When children have two fathers: Effects of relationships with stepfathers and noncustodial fathers on adolescent outcomes. Journal of Marriage and Family. 2001;63(1):155–167. [Google Scholar]
- Wood RG, Covington R. Evidence from the Building Strong Families Evaluation Limited father involvement: Which families are most at risk? Princeton, NJ: Mathematica Policy Rsearch; 2014. [Google Scholar]
- Yeung WJ, Sandberg JF, Davis-Kean PE, Hofferth SL. Children's time with fathers in intact families. Journal of Marriage and Family. 2001;63(1):136–154. [Google Scholar]