

Abstract
Background: To identify and characterize the concomitant ligamentous and meniscal injuries in floating knee. Methods: A total of 37 cases of floating knee were enrolled. Arthroscopic or open surgical examination of the knee, Lachman test, posterior drawer’s test, and varus and valgus stress tests under anesthesia were carried out to determine the incidence of knee injury. Results: Through arthroscopic and open surgical examinations, a medial meniscal tear was detected in 14 (37.8%) cases and a lateral meniscal tear in 11 (29.7%). Twenty-one (56.8%) patients had anterior cruciate ligament (ACL) injury including complete injury in 6 and incomplete injury in 15 cases. Three (8.1%) patients had posterior cruciate ligament (PCL) tear, including complete injury in 1 and incomplete injury in 2. Varus and valgus stress tests revealed that 10 (27.0%) and 7 (18.9%) patients had medial and lateral collateral ligament (MCL and LCL) laxity, respectively. Lachman test showed positive in 8 (21.6%) cases. Posterior drawer test showed positive in 3 (8.1%) cases. Twenty-six (70.3%) patients had knee ligamentous injuries. ACL injury was the most common ligamentous injury. ACL injury in 15 (71.4%) cases was associated with meniscal injury, including medial meniscal injury in 9 (42.9%) and lateral meniscal injury in 6 (28.6%). Conclusion: Physicians should pay attention to the concomitant ligamentous and meniscal injuries in floating knee. Careful clinical examination with aid of arthroscopic examination is helpful for the early diagnosis and treatment of these injuries.
Keywords: Arthroscopy, floating knee, tibia fracture, meniscal injury, ligamentous injury
Introduction
Floating knee, referring to ipsilateral fractures of the femur and tibia, is usually associated with several complications and high mortality. Road traffic accident accounts for majority of the cases and this is followed by fall from height [1]. This injury is caused by high-energy trauma with extensive skeletal and soft tissue damage, and they are often associated with potentially life-threatening injuries of the head, chest, and abdomen [2,3]. Because considerable amount of energy is required to cause the floating knee injuries, ipsilateral knee ligamentous and meniscal injuries may occur simultaneously. Whenever a patient is received in a trauma unit, clinician’s attention usually focus on life-threatening injuries, open wounds, and radiologically visible fracture/fractures. Knee ligamentous and meniscal injuries are mostly not visible in plain radiographs taken in the emergency, which are likely to be overlooked or entirely missed by clinicians. Such associated knee injuries may potentially lead to significant morbidity to the patient, especially if they are unrecognized and untreated. This study was to identify and characterize the concomitant ligamentous and meniscal injuries in floating knee.
Materials and methods
From May 2008 to October 2012, 37 patients with floating knees were recruited into present study. The inclusion criteria were as follows: 1) patients had indications for surgery; 2) patients had no history of previous injuries to the knees; 3) patients had no major limb vascular injuries and compartment syndrome. The mean age of 37 patients was 38.6 years (range: 18-56 years), and there were 31 males (83.8%). The injuries were ascribed to high energy trauma: motor vehicle accident (n = 33) and fall from height (n = 4). The floating knee injuries were classified according to the Fraser classification [4]: Type I (n = 27), Type IIa (n = 4), Type IIb (n = 5) and Type IIc (n = 1) injuries.
Once the disease condition was stabilized, attempt was made to stabilize fractures of the femur and tibia. Open reduction and internal fixation (ORIF) was the common treatment. Management of femoral fracture was done using plate fixation in 20 patients and intramedullary nailing in 17 (anterograde nailing in 9 and retrograde nailing in 8). Management of tibial fracture was done using external fixation in 17 patients, plate fixation in 13 and intramedullary nailing in 7.
After fracture fixation, clinical examination of the knee and arthroscopy under the anesthesia were performed to determine the concomitant ligamentous and meniscal injuries. All the patients underwent a thorough physical examination of the involved limb. Varus and valgus stress tests were used to clinically assess medial and lateral collateral ligament (MCL and LCL), respectively. Lachman’s test and posterior drawer’s test were employed to clinically evaluate the anterior and posterior cruciate ligaments (ACL and PCL), respectively. Clinical assessments were done to compare both knees in the same patient. In 10 patients, the knees had to be exposed for internal fixation and a direct examination of the joint was performed. Therefore, there was no need to perform arthroscopic evaluation in these cases. Additionally, arthroscopy was performed in remaining 27 cases through standard anterolateral and anteromedial portals using normal saline as distension and irrigation fluid. When the visualization of any compartment was difficult, additional portals were made. All the clinical assessments were carried out by a single trained orthopaedic surgeon.
Results
A total of 37 patients were enrolled into this study. Through arthroscopy and open surgical examination, a medial meniscal tear was detected in 14 (37.8%) patients (Figure 1) and a lateral meniscal tear in 11 (29.7%). Twenty-one (56.8%) patients had ACL injury, including complete injury in 6 and incomplete injury in 15. Three (8.1%) patients had PCL tear, complete tear in 1 and incomplete injury in 2. Varus and valgus stress tests revealed that 10 (27.0%) and 7 (18.9%) patients had MCL and LCL laxity, respectively. Lachman test showed positive in 8 (21.6%) cases and posterior drawer test positive in 3 (8.1%). The incidence of concomitant knee ligamentous and meniscal injuries is presented in Table 1.
Figure 1.
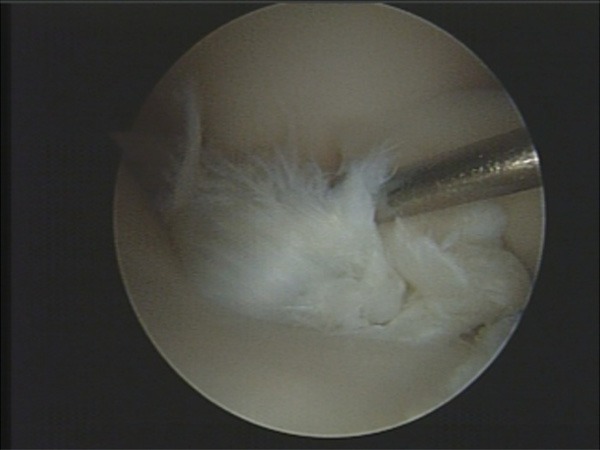
The posterior 1/3 of medial meniscal tear.
Table 1.
Incidence and types of concomitant knee ligamentous and meniscal injuries
| Item | n (%) |
|---|---|
| Arthroscopic findings | |
| Medial meniscal tear | 14 (37.8%) |
| Lateral meniscal tear | 11 (29.7%) |
| ACL injury | 21 (56.8%) |
| Complete injury | 6 (16.2%) |
| Incomplete injury | 15 (40.5%) |
| PCL injury | 3 (8.1%) |
| Complete injury | 1 (2.7%) |
| Incomplete injury | 2 (5.4%) |
| Stress tests | |
| MCL laxity | 10 (27.0%) |
| LCL laxity | 7 (18.9%) |
| Positive Lachman test | 8 (21.6%) |
| Positive posterior drawer test | 3 (8.1%) |
In our study, twenty-six (70.3%) patients had knee ligamentous injuries. ACL injury was the most common ligamentous injury. ACL injury in 15 cases (71.4%) was associated with the meniscal injury, including medial meniscal injury in 9 (42.9%) (Figure 2) and lateral meniscal injury in 6 (28.6%).
Figure 2.
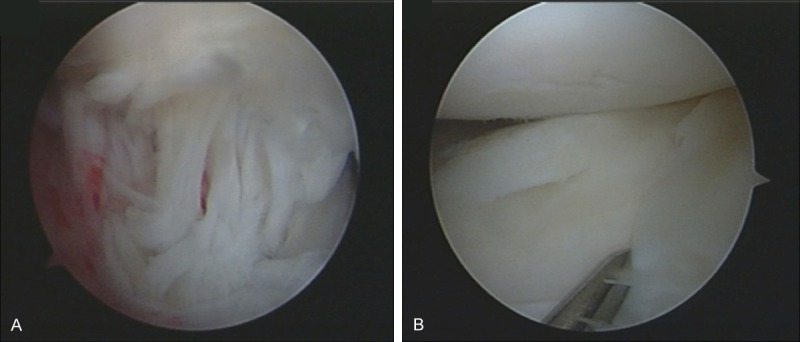
ACL injury associated with meniscal tear. A. Complete ACL injury; B. The posterior third of medial meniscal radial tear.
Discussion
The floating knee was introduced for the first time by Blake and McBryde [3] in 1975. It is usually caused by high energy trauma and likely a part of polytrauma. An expanding population, increasing number of motor vehicles on limited infrastructure of most cities in developing countries and various modes of treatments have made the floating knee injury a concern from both medical and socio-economic standpoints [5]. As expected, patients examined in this study had a high incidence of concomitant knee ligamentous and meniscal injuries. This may be a diagnostic enigma in floating knee due to difficulty in the clinical assessment of the knee in the presence of fractures of both knees. These injuries are easily missed due to the “distracting” nature of the floating knee injuries [6]. One should suspect the ligamentous and meniscal injuries of the knee when floating knee is present [7].
MRI has proven to be valuable in the detection of soft tissue injuries of the knee because of its sensitivity and specificity [8]. However, Rethnam et al. [6] did not recommend MRI for the assessment of knee ligament injuries in floating knee patients. In the presence of a floating knee, to perform MRI prior to surgical stabilization of the fractures would cause problems in patients with unstable hemodynamics. After surgical stabilization of the fractures, there may be interference artefacts from the metal work, preventing proper visualization of the knee ligaments. Therefore, a clinical assessment under anesthesia followed by a diagnostic arthroscopy is the best strategy for the assessment of ligament injuries in these patients [6].
Emami Meybodi et al. [9] investigated 40 patients with ipsilateral femoral fractures and 2 patients with bilateral femoral fractures by arthroscopy, and reported medial meniscus injury in 12 (27%) knees and lateral meniscus injury in 3 (7%). In our series, 37.8% of medial meniscus injury and 29.7% of lateral meniscal tears were associated with floating knee injuries, which were higher than that reported by Emami Meybodi et al [9]. Furthermore, complex and radial tears were more common.
Walling et al. [10] evaluated 24 American patients with fractures of the femoral shaft. They found 33% had ligament injuries of the ipsilateral knee. Paul et al. [11] reported 21 patients with fractures of the ipsilateral femur and tibia, and over 50% of patients suffered from concomitant ipsilateral knee injuries. Szalay et al. [12] examined 110 Australian patients with 114 femoral shaft fractures and reported ligament laxity in 27% of patients. In addition, they investigated other 33 patients with 34 ipsilateral femoral and tibial fractures. In this group, 53% of patients had knee ligament laxity; leading to the conclusion that knee ligament injury is more common in the simultaneous femoral and tibial fractures than in the single femoral fractures. The incidence of ligament injury in our study (70.3%) was relatively higher than that reported by Walling et al.. Floating knee requires stronger force to cause fracture of two strongest bones in the body, and thus it is not surprising that there are much more concomitant ligamentous injuries than femoral shaft fractures. Meticulous examination of the knee at the time of floating knee injury is strongly advocated [13].
Kumar et al. [14] retrospectively investigated 41 patients with femoral shaft fractures, and reported that the incidence of ACL injury was 31.7% and ACL injury the most common injury. In our study, ACL injury was detected in 21 (56.8%) cases and also the most common injury. Thus, careful clinical examinations should be performed to indentify ACL injury. Lachmann test has the sensitivity of almost 100% in the diagnosis of anterior cruciate ligament tear when it is performed under anesthesia [15]. Nevertheless, our results showed Lachman test was negative in the majority of subjects who suffered from ACL injuries. Positive Lachman test was observed in only 6 patients with complete ACL injuries and 2 patients with incomplete ACL injuries. Thirteen patients with incomplete ACL injuries had negative Lachman test. It has been reported that it is difficult to identify partial ACL tears by a physical examination [16,17]. Our study also proved that results from Lachman test had a low consistence with those from arthroscopic examination and thus Lachman test has a limited application in detecting incomplete tears. Arthroscopic examination should be performed if ACL injury is highly suspicious, even in the face of an evidently normal physical examination.
Kumar et al. [14] investigated a total of 93 cases of lower limb long bone fractures by arthroscopy and found only 15.4% of ACL injuries were an isolated type and 69.2% were associated with either a medial or a lateral meniscal injury. In our study, ACL injury in 15 (71.4%) cases was associated with meniscal injury, of which 9 (42.9%) had medial meniscal injury and 6 (28.6%) had lateral meniscal injury. Our findings suggest a higher incidence of meniscal injuries related to ACL injury in floating knee.
In summary, based on our observations, concomitant ligamentous and meniscal injuries are rather common in floating knee. Therefore, clinicians should pay attention to concomitant ligamentous and meniscal injuries in floating knee. Careful clinical examination with aid of arthroscopic examination is helpful for the early diagnosis and treatment of injured tissues. Recognition of ligamentous and meniscal injuries of the knee in acute phase is essential for the optimal treatment and prognosis.
Disclosure of conflict of interest
None.
References
- 1.Nouraei MH, Hosseini A, Zarezadeh A, Zahiri M. Floating knee injuries: Results of treatment and outcomes. J Res Med Sci. 2013;18:1087–1091. [PMC free article] [PubMed] [Google Scholar]
- 2.Veith RG, Winquist RA, Hansen ST Jr. Ipsilateral fractures of the femur and tibia. A report of fifty-seven consecutive cases. J Bone Joint Surg Am. 1984;66:991–1002. [PubMed] [Google Scholar]
- 3.Blake R, McBryde A Jr. The floating knee: Ipsilateral fractures of the tibia and femur. South Med J. 1975;68:13–16. [PubMed] [Google Scholar]
- 4.Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br. 1978;60-B:510–515. doi: 10.1302/0301-620X.60B4.711798. [DOI] [PubMed] [Google Scholar]
- 5.Dwyer AJ, Paul R, Mam MK, Kumar A, Gosselin RA. Floating knee injuries: long-term results of four treatment methods. Int Orthop. 2005;29:314–318. doi: 10.1007/s00264-005-0679-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rethnam U, Yesupalan RS, Nair R. Impact of associated injuries in the floating knee: a retrospective study. BMC Musculoskelet Disord. 2009;10:7. doi: 10.1186/1471-2474-10-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van Raay JJ, Raaymakers EL, Dupree HW. Knee ligament injuries combined with ipsilateral tibial and femoral diaphyseal fractures: the “floating knee”. Arch Orthop Trauma Surg. 1991;110:75–77. doi: 10.1007/BF00393877. [DOI] [PubMed] [Google Scholar]
- 8.Kostov H, Stojmenski S, Kostova E. Reliability Assessment of Arthroscopic Findings Versus MRI in ACL Injuries of the Knee. Acta Inform Med. 2014;22:111–114. doi: 10.5455/aim.2014.22.111-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Emami Meybodi MK, Ladani MJ, Emami Meybodi T, Rahimnia A, Dorostegan A, Abrisham J, Yarbeygi H. Concomitant ligamentous and meniscal knee injuries in femoral shaft fracture. J Orthop Traumatol. 2014;15:35–39. doi: 10.1007/s10195-013-0255-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Walling AK, Seradge H, Spiegel PG. Injuries to the knee ligaments with fractures of the femur. J Bone Joint Surg Am. 1982;64:1324–1327. [PubMed] [Google Scholar]
- 11.Paul GR, Sawka MW, Whitelaw GP. Fractures of the ipsilateral femur and tibia: emphasis on intra-articular and soft tissue injury. J Orthop Trauma. 1990;4:309–314. doi: 10.1097/00005131-199004030-00013. [DOI] [PubMed] [Google Scholar]
- 12.Szalay MJ, Hosking OR, Annear P. Injury of knee ligament associated with ipsilateral femoral shaft fractures and with ipsilateral femoral and tibial shaft fractures. Injury. 1990;21:398–400. doi: 10.1016/0020-1383(90)90129-i. [DOI] [PubMed] [Google Scholar]
- 13.Rethnam U, Yesupalan RS, Nair R. The floating knee: epidemiology, prognostic indicators & outcome following surgical management. J Trauma Manag Outcomes. 2007;1:2. doi: 10.1186/1752-2897-1-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kumar B, Borgohain B, Balasubramanian S, Sathyanarayana V, Muthusamy M. Risks of concomitant trauma to the knee in lower limb long bone shaft fractures: A retrospective analysis from a prospective study population. Adv Biomed Res. 2014;3:49. doi: 10.4103/2277-9175.125764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jonsson T, Althoff B, Peterson L, Renstrom P. Clinical diagnosis of ruptures of the anterior cruciate ligament: a comparative study of the Lachman test and the anterior drawer sign. Am J Sports Med. 1982;10:100–102. doi: 10.1177/036354658201000207. [DOI] [PubMed] [Google Scholar]
- 16.Donaldson WF 3rd, Warren RF, Wickiewicz T. A comparison of acute anterior cruciate ligament examinations. Initial versus examination under anesthesia. Am J Sports Med. 1985;13:5–10. doi: 10.1177/036354658501300102. [DOI] [PubMed] [Google Scholar]
- 17.Umans H, Wimpfheimer O, Haramati N, Applbaum YH, Adler M, Bosco J. Diagnosis of partial tears of the anterior cruciate ligament of the knee: value of MR imaging. AJR Am J Roentgenol. 1995;165:893–897. doi: 10.2214/ajr.165.4.7676988. [DOI] [PubMed] [Google Scholar]