

Abstract
Aldosterone synthase is a mitochondrial enzyme that catalyzes the conversion of 11-deoxycorticosterone to the potent mineralocorticoid aldosterone. The gene encoding aldosterone synthase, CYP11B2, is associated with essential hypertension. But if the genetic variations in aldosterone synthesis could influence the antihypertensive response to Valsartan is not clear. A Chinese sample of 502 persons (217 women) was studied, which was divided into the hypertensive group (EH) of 345 persons and the normotensive group (NB) of 157 persons. Subjects were genotyped through the use of the polymerase chain reaction for the diallelic polymorphisms in CYP11B2. 98 persons of the essential hypertension group received 4 weeks therapy with valsartan. Blood pressure, 24-hour ambulatory blood pressure, biochemical index were also determined. The frequency of CC+CT genotypes in hypertensive group was significantly higher than that in normotensive group (P<0.05), the frequency of C allele of gene CYP11B2 (-344T/C) in hypertensive group was significantly higher than that in normotensive group (P<0.01). The descending values of SBP (systolic blood pressure), DBP (diastolic blood pressure), MAP (mean arterial pressure), 24 h SBP (mean SBP of 24 hours), 24 h DBP (mean DBP of 24 hours), 24 h MAP (mean arterial pressure of 24 hours) of CC+CT genotype group were significantly higher than those of the TT genotype group (P<0.05). The aldosterone synthase CYP11B2 (-344T/C) gene polymorphism is associated with essential hypertension in Chinese. And the aldosterone synthase CYP11B2 (-344T/C) gene polymorphism may be the predictor of the antihypertensive response to Valsartan.
Keywords: Genetics, CYP11B2, aldosterone, blood pressure monitoring, hypertension, antihypertensive response
Introduction
A number of constitutional and environmental factors have been identified that influence blood pressure. These include age, body size, physical activity, salt intake, and alcohol consumption. People who have family history would more likely suffer from Hypertension. So it is inferred that inherited factors are also important. Moreover, if the same drug given to the patients, we could observe the different antihypertensive effects. So maybe there is some relativity between antihypertensive results and genetic backgrounds. To date, several gene polymorphisms were studied, such as ACE I/D gene [1], a-adducin gene [2], eNOS gene [3], ATIR gene [4], et al. Among them, the CYP11B2 gene encodes a key enzyme of the aldosterone biosynthesis-aldosterone synthase. Because the renin-angiotensin system (RAS) is a major regulator of intravascular volume and blood pressure. A key effector of the RAS is aldosterone, the primary human mineralocorticoid, which acts on the distal nephron to regulate sodium resorption, potassium excretion, and intravascular volume. So the associations between the genetic variations in aldosterone synthase gene and hypertension would thus be of significant interest. Several studies about the relationship between CYP11B2 (-344T/C) polymorphism and essential hypertension have been reported, with controversial results. Whereas some studies have found that the T-allele is more common in hypertension and subjects with increased urinary aldosterone excretion rate [5,6], others have demonstrated no significant difference between either allele with hypertension [7,8]. It was also suggested that the C allele might be associated with genetic predisposition to hypertension in China [9]. Several factors such as gender, age and ethnicity could be involved in the phenotypic expression of this polymorphism. Some studies evaluated the impact of -344T/C polymorphism of the CYP11B2 on the severity of hypertension and the response to antihypertensive drugs [10,11]. For example, studies have suggested that CYP11B2 (-344T/C) gene polymorphism is associated with the antihypertensive response to ACE inhibitors [12]. But whether the genotypes could affect the antihypertensive response to angiotensin-receptor-inhibiter is not clear. The present study was designed to investigate the association between -344T/C polymorphism of the CYP11B2 gene and the genetic predisposition to essential hypertension. Furthermore, we observed the antihypertensive response to valsartan in Chinese patients with essential hypertension.
Materials and methods
Subject
The study population was selected at our outpatient clinic from 1999 to 2003. The blood pressures (BP) of these 501 subjects were measured on more than 2 separate occasions with subjects under no drug treatment. A normotensive control group (NB) was composed of 156 subjects (67 women) whose average age was 49.03±10.41. The criteria for normotension were BP <140/90 mmHg. The remaining 345 subjects had systolic BP ≥140 mmHg or diastolic BPs ≥90 mmHg; no family history of hypertension, no history of cardiomyopathy, valvular heart disease, congenital heart disease, diabetes mellitus and renal failure or other serious diseases. These 345 subjects (150 women) whose average age was 48.32±9.12 comprised a hypertensive group (EH). There were no significant differences in age and gender distribution across the two groups. 98 persons were selected from the hypertensive group randomly, who took valsartan (80 mg) at 8 am everyday for 4 weeks. This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Capital Medical University. Written informed consent was obtained from all participants.
Resting brachial artery cuff blood pressure was averaged over 3 measurements. That blood pressure was defined as CBP (clinic blood pressure). The 24-hour ambulatory blood pressure monitoring (ABPM) was performed. MAP (Mean arterial pressure) = DBP (Diastolic blood pressure) + (SBP (systolic blood pressure)-DBP)/3. The fasting blood glucose (FBG), triglycerides (TG), total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), uric acid (UA), creatinine (CRE), alanine aminotransferase (ALT) were measured.
DNA extraction
DNA was extracted from whole blood using modified Miller’s protocol [13]. Firstly, nucleated cells obtained from anticoagulated blood were re-suspended in 15 ml polypropylene centrifugation tubes with 3 ml of nuclei lysis buffer. Secondly, the cell lysates were digested overnight at 37°C. Thirdly, NaCl was added to each tube and shaken vigorously for 15 seconds, followed by centrifugation at 2500 rpm for 15 minutes. At last, DNA was transferred to another tube and precipitated DNA strands were ready for use.
PCR analysis
CYP11B2 were amplified from about 20 ng of each DNA sample by the polymerase chain reaction in 20 μL reactions containing 0.2 U Taq DNA polymerase, 1× concentration of the supplied buffer, 0.2 mmol/L concentration of each deoxynucleotide triphosphate, and 10 pmol of each primer (Boehring Ingelheim). After initial denaturation at 94°C for 5 minutes; 33 cycles of 94°C for 45 seconds, 55°C annealing for 45 seconds, and 72°C extension for 1 minutes; 72°C extension for 10 minutes in the end. Subjects were genotyped for the -344 promoter polymorphism using primers 5’-aaggagggatacaaattacataca-3’ (sense) and 5’-gaaaaggcgtggggtct g -3’ (antisense) [14]. Then, 5 μL from each reaction (consisting mainly of a 384-bp product) was digested with 10 U of restriction endonuclease Hae III (Boehring Ingelheim) in the supplied buffer for 2 hours at 37°C. Reactions were subjected to electrophoresis in 1% agarose gels [15].
Statistical analysis
Numerical data were analyzed by an unpaired t test or one-way ANOVA. Frequency data and the Hardy-Weinberg principle were analyzed by the x2 test. Two-tailed values of P<0.05 were considered statistically significant. To examine the independent contribution of CYP11B2 gene polymorphisms to hypertension, while adjusting for the effects of other clinical characteristics, we used a logistic analysis. For hypertension, a baseline logistic model was developed by applying backward stepwise selection with the following factors as covariates: gender, body mass index (BMI), blood lipid, and polymorphisms of the CYP11B2 gene. Backward selection was used, and a P value of 0.05 or greater was required for a variable to be removed from the model.
Results
Polymorphism of CYP11B2 (-344T/C)
The polymorphism of CYP11B2 (-344T/C) is located in the transcriptional regulatory region, or promoter, of CYP11B2, 344 nucleotides before the start of the protein coding sequence. This position can be either a cytosine (-344C) or thymidine (-344T). Persons homozygous for C, heterozygous for C and T, or homozygous for T will be referred to as having the genotypes -344CC, -344CT, or -344TT, respectively. The PCR reaction was 384 bp fragments. The -344T allele lacks a Hae III site (GGCC) present in the -344C allele, so -344T alleles were detected as Hae III fragments of 327 bp and -344C alleles as fragments of 256 bp (plus smaller fragments in each case). So the electrophoresis results of -344TT genotype had 327 bp fragments; the results of -344CC genotype had 256 bp fragments; the results of -344CT genotype had both 327 bp and 256 bp fragments (Figures 1, 2).
Figure 1.
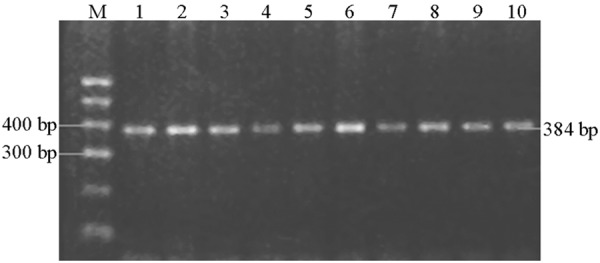
The PCR results.
Figure 2.
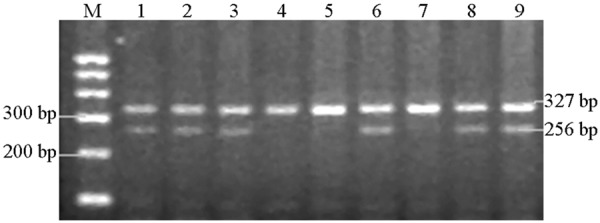
The electrophoresis results of polymorphisms of CYP11B2 (-344T/C) gene.
Distribution of genotypes
The results showed that there were C and T alleles in both essential hypertension group (EH group) and normotensive group (NB group). There were TT, TC and CC genotypes in both groups. After x2 test, the distribution of genotypes of two groups was compatible with Hardy-Weinberg equilibrium (P>0.05).
There were significant differences in the frequencies of different genotypes across EH and NB groups (P<0.05). The frequency of CC+CT genotypes in the EH group was significantly higher than that in the NB group, the frequency of C allele in the EH group was significantly higher than that in the NB group (P<0.01, Table 1).
Table 1.
Associations between CYP11B2 (-344T/C) genotype and essential hypertension
| Groups | Frequencies of different Genotypes | Frequencies of alleles | |||
|---|---|---|---|---|---|
|
| |||||
| CC | CT | TT | C | T | |
| EH group (n=345) | 15.1% (52) | 51.9% (179)* | 33% (114)* | 41.1% (283) | 58.9% (407)# |
| NB group (n=156) | 8.3% (13) | 46.8% (73) | 44.9% (70) | 31.7% (99) | 68.3% (213) |
Compared with NB group (P<0.05);
compared with NB group (P<0.01).
Logistic analysis
The logistic analysis showed that the C allele of CYP11B2 (-344T/C) gene independently predicted the essential hypertension if age, gender, blood lipid, blood pressure, BMI was forced into the equation (P=0.006).
Associations between CYP11B2 (-344T/C) gene polymorphism and antihypertensive response to valsartan
There were no significant differences in systolic and diastolic blood pressure across the CC+CT genotype group and the TT genotype group before drug treatment (P>0.05). The descending values of systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), mean SBP of 24 hours (24 h SBP), mean DBP of 24 hours (24 h DBP), mean MAP of 24 hours (24 h MAP) of CC+CT genotype group were significantly higher than those of TT genotype group after 4 weeks of antihypertensive treatment by valsartan (P<0.05, Table 2).
Table 2.
Associations between CYP11B2 (-344T/C) gene polymorphism and antihypertensive response to valsartan
| CC+CT (n=65) | TT (n=33) | P | |
|---|---|---|---|
| CSBP (mmHg) | 149.58±12.38 | 146.56±13.48 | P>0.05 |
| CDBP (mmHg) | 95.42±8.50 | 96.50±7.38 | P>0.05 |
| cMAP (mmHg) | 113.47±8.81 | 113.19±8.24 | P>0.05 |
| 24 h SBP (mmHg) | 137.60±11.44 | 135.27±11.86 | P>0.05 |
| 24 h DBP (mmHg) | 83.47±7.73 | 84.45±6.71 | P>0.05 |
| 24 h MAP (mmHg) | 101.52±8.24 | 101.39±7.60 | P>0.05 |
| ΔcSBP(mmHg) | 16.38±8.37 | 11.65±5.10 | P<0.01 |
| ΔcDBP (mmHg) | 9.69±4.76 | 6.35±4.85 | P<0.01 |
| ΔcMAP (mmHg) | 11.92±4.85 | 8.12±4.25 | P<0.01 |
| Δ24 h SBP (mmHg) | 14.80±7.19 | 10.40±4.29 | P<0.01 |
| Δ24 h DBP (mmHg) | 6.19±4.62 | 4.04±3.50 | P<0.05 |
| Δ24 h MAP (mmHg) | 9.06±3.88 | 6.16±2.52 | P<0.01 |
ΔBP: The descending values of the blood pressure after therapy.
Discussion
Our results indicated that the CYP11B2 (-344T/C) Gene Polymorphism was associated with essential hypertension; the frequency of C allele of hypertensive group was significantly higher than that of normotensive control group. The mechanism might be that the mutation is located in the promoter of the aldosterone synthase gene, which is immediately adjacent to a binding site for a transcription factor (SF-1). In vitro, the -344C allele binds SF-1 approximately four times as strongly as does the -344T allele [16], which is consistent with an effect on expression of CYP11B2. The difference of the efficiency of combination might influence the reaction to angiotensin II, which could result in the difference of the efficiency of transcription. The persons with C allele might have the higher efficiency of transcription, which resulted in the more aldosterone synthase that could increase the aldosterone level. So the intravascular volume increased, that could increase blood pressure [17]. Pojoga et al. [18] reported that the plasma aldosterone level of the patients with CC genotype was significantly higher than that of the patients with CT genotype, which was higher than that of the patients with TT genotype. Tamaki et al. [19] reported that the ratio of the plasma aldosterone compared with plasma rennin of the patients with C allele was significantly higher than that of the patients who had no C allele. All the studies could approve this mechanism.
The study on the association between the CYP11B2 (-344T/C) gene polymorphism and antihypertensive response to benazepril indicated that the descending value of blood pressure in patients with CC genotype was higher than that in patients with other genotypes [12]. Another study suggested that ACE and CYP11B2 genes influence the response to hydrochlorothiazide in Han Chinese hypertensive patients [20]. But the studies on the antihypertensive response to valsartan were few. Our study indicated that the CYP11B2 (-344T/C) gene polymorphism was a predictor of antihypertensive response to valsartan and the descending value of SBP and DBP in patients with C allele was significantly higher than that in patients with no C allele after 4 weeks’ therapy. The genotypes might influence the response to valsartan because of the change of the quantity of aldosterone synthase that resulted in the different level of aldosterone. Valsartan could break the combination of angiotensin II and the receptor, which could intensively restrain the synthesis of aldosterone. The patients with C allele had the higher level of aldosterone, so they had the more intensive restraining of the synthesis of aldosterone under the therapy by the same dose of valsartan. So the antihypertensive response to valsartan in patients with C allele was better than that in patients with other genotypes.
Disclosure of conflict of interest
None.
References
- 1.Rasyid H, Bakri S, Yusuf I. Angiotensin-converting enzyme gene polymorphisms, blood pressure and pulse pressure in subjects with essential hypertension in a South Sulawesi Indonesian population. Acta Med Indones. 2012;44:280–283. [PubMed] [Google Scholar]
- 2.Beeks E, Janssen RG, Kroon AA, Keulen ET, Geurts JM, de Leeuw PW, de Bruin TW. Association between the alpha-adducin Gly460Trp polymorphism and systolic blood pressure in familial combined hyperlipidemia. Am J Hypertens. 2001;14:1185–1190. doi: 10.1016/s0895-7061(01)02216-6. [DOI] [PubMed] [Google Scholar]
- 3.Soudani NY, Fakhoury RM, Kaissi SS, Zgheib NK. The role of genetic polymorphisms in endothelial nitric oxide synthase and beta2-adrenergic receptors with risk of hypertension in a sample of Lebanese people. Saudi Med J. 2014;35:255–260. [PubMed] [Google Scholar]
- 4.Shahin DS, Irshaid YM, Saleh AA. The A(1166)C polymorphism of the AT1R gene is associated with an early onset of hypertension and high waist circumference in Jordanian males attending the Jordan University Hospital. Clin Exp Hypertens. 2014;36:333–339. doi: 10.3109/10641963.2013.827698. [DOI] [PubMed] [Google Scholar]
- 5.Hlubocká Z, Jáchymová M, Heller S, Umnerová V, Danzig V, Lánská V, Horký K, Linhart A. Association of the -344T/C aldosterone synthase gene variant with essential hypertension. Physiol Res. 2009;58:785–792. doi: 10.33549/physiolres.931450. [DOI] [PubMed] [Google Scholar]
- 6.Cheng X, Xu G. Association between aldosterone synthase CYP11B2 polymorphism and essential hypertension in Chinese: A meta-analysis. Kidney Blood Press Res. 2009;32:128–140. doi: 10.1159/000215738. [DOI] [PubMed] [Google Scholar]
- 7.Kato N, Sugiyama T, Morita H, Kurihara H, Furukawa T, Isshiki T, Sato T, Yamori Y, Yazaki Y. Comprehensive analysis of the renin- angiotensin gene polymorphisms with relation to hypertension in the Japanese. J Hypertens. 2000;18:1025–1032. doi: 10.1097/00004872-200018080-00006. [DOI] [PubMed] [Google Scholar]
- 8.Tsujita Y, Iwain N, Katsuya T, Higaki J, Ogihara T, Tamaki S, Kinoshita M, Mannami T, Ogata J, Baba S. Lack of association between genetic polymorphism of CYP11B2 and hypertension in Japanese: the Suita Study. Hypertens Res. 2001;24:105–9. doi: 10.1291/hypres.24.105. [DOI] [PubMed] [Google Scholar]
- 9.Tang W, Wu H, Zhou X, Cheng B, Dong Y, He L, Yu H, Xu L, Lu J, Li K, Xiao C. Association of the C-344T polymorphism of CYP11B2 gene with essential hypertension in Hani and Yi minorities of China. Clin Chim Acta. 2006;364:222–225. doi: 10.1016/j.cccn.2005.07.006. [DOI] [PubMed] [Google Scholar]
- 10.Li Y, Yang P, Wu SL, Yuan JX, Wu Y, Zhao DD, Xu S, Zhao LP, Sun MJ, Chu LM, Lu DS. Effect of CYP11B2 gene -344T/C polymorphism on renin-angiotensin-aldosterone system activity and blood pressure response to hydrochlorothiazide. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2012;29:68–71. doi: 10.3760/cma.j.issn.1003-9406.2012.01.017. [DOI] [PubMed] [Google Scholar]
- 11.Taverne K, de Groot M, de Boer A, Klungel O. Genetic polymorphisms related to the renin-angiotensin-aldosterone system and response to antihypertensive drugs. Expert Opin Drug Metab Toxicol. 2010;6:439–460. doi: 10.1517/17425250903571670. [DOI] [PubMed] [Google Scholar]
- 12.Nordestgaard BG, Kontula K, Benn M, Dahlöf B, de Faire U, Edelman JM, Eliasson E, Fyhrquist F, Hille DA, Ibsen H, Lyle PA, Berg K, Sandberg M, Sethi AA, Wong PH, Os I. Effect of ACE insertion/deletion and 12 other polymorphisms on clinical outcomes and response to treatment in the LIFE study. Pharmacogenet Genomics. 2010;20:77–85. doi: 10.1097/FPC.0b013e328333f70b. [DOI] [PubMed] [Google Scholar]
- 13.Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16:1215. doi: 10.1093/nar/16.3.1215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhang G, Miller WL. The human genome contains only two CYP11B (P450c11) genes. J Clin Endocrinol Metab. 1996;81:3254–3256. doi: 10.1210/jcem.81.9.8784078. [DOI] [PubMed] [Google Scholar]
- 15.Hua Q, Li DB. Associations between gene polymorphism of endothelial nitric oxide synthase and essential hypertension and antihypertensive response of valsartan. J Hypertens. 2004;12:331–334. [Google Scholar]
- 16.White PC, Hautanen A, Kupari M. Aldosterone synthase (CYP11B2) polymorphisms and cardiovascular function. J Steroid Biochem Mol Biol. 1999;69:409–12. doi: 10.1016/s0960-0760(99)00071-0. [DOI] [PubMed] [Google Scholar]
- 17.Freel EM, Connell JM. Mechanisms of hypertension: the expanding role of aldosterone. J Am Soc Nephrol. 2004;15:1993–2001. doi: 10.1097/01.ASN.0000132473.50966.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pojoga L, Gantier S, Blanc H, Guyene TT, Poirier O, Cambien F, Benetos A. Genetic determination of plasma aldosterone levels in essential hypertension. Am J Hypertens. 1998;11:856–860. doi: 10.1016/s0895-7061(98)00048-x. [DOI] [PubMed] [Google Scholar]
- 19.Tamaki S, Iwai N, Tsujita Y, Kinoshita M. Genetic polymorphism of CYP11B2 gene and hypertension in Japanese. Hypertension. 1999;33:266–270. doi: 10.1161/01.hyp.33.1.266. [DOI] [PubMed] [Google Scholar]
- 20.Li Y, Zhou Y, Yang P, Niu JQ, Wu Y, Zhao DD, Wu SL. Interaction of ACE and CYP11B2 genes on blood pressure response to hydrochlorothiazide in Han Chinese hypertensive patients. Clin Exp Hypertens. 2011;33:141–146. doi: 10.3109/10641963.2010.531838. [DOI] [PubMed] [Google Scholar]