

Abstract
This case report describes a distal ureteral atresia along with ureteropelvic junction obstruction which occurred in a 19-month-old female child. It is easily to be misdiagnosed as mere ureteropelvic junction obstruction and omitted the combined diagnosis of distal ureteral atresia. Dismembered pyeloplasty was done in local hospital after admission, however with the result of recurrent fever when clamp the left nephrostomy tube and Antegrade urography demonstrated distal ureteral atresia. After two months, boari flap reconstruction was performed for the patient in the Second Xiangya Hospital of Central South University, and the child had good rehabilitation in the end. To our knowledge, this is the first case report on distal ureteral atresia associated with ureteropelvic junction obstruction.
Keywords: Distal ureteral atresia, ureteropelvic junction obstruction, rare entity
Introduction
Distal Ureteral Atresia is a rare disease usually associated with a non-functioning kidney [1]. Its combination with another urinary abnormality is even rarer [2]. We here report a case of a 19-month-old female child, who was misdiagnosed as ureteropelvic junction obstruction, presenting with a left renal hydronephrosis because of upper and middle ureteral dilatation is not obvious, in fact distal ureteral atresia with ureteropelvic junction obstruction. To our knowledge, in the English literature, this is the first case report on distal ureteral atresia associated with ureteropelvic junction obstruction.
Case report
A 19-month-old female child, who presented with left flank discomfort and had no history of trauma, was admitted to local hospital for further investigation. Contrasted Computed Tomography showed that hydronephrosis with delayed enhancement in left kidney, renal parenchymal thickness can be fair (Figure 1). Magnetic resonance urography (MRU) indicated ureteropelvic junction obstruction (Figure 2). After dismembered pyeloplasty in local hospital, the child had recurrent fever when clamp the left nephrostomy tube. Antegrade urography demonstrated that left double J had not arrived at the bladder, mild dilatation of the upper, middle ureter and distal ureteral atresia (Figure 3).
Figure 1.
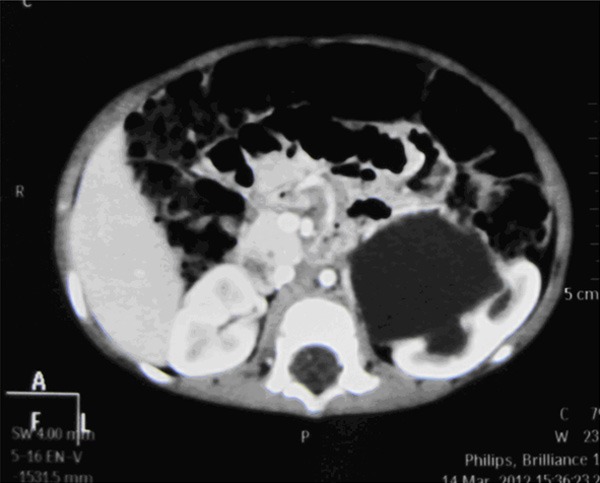
CT showed that hydronephrosis with delayed enhancement in left kidney.
Figure 2.
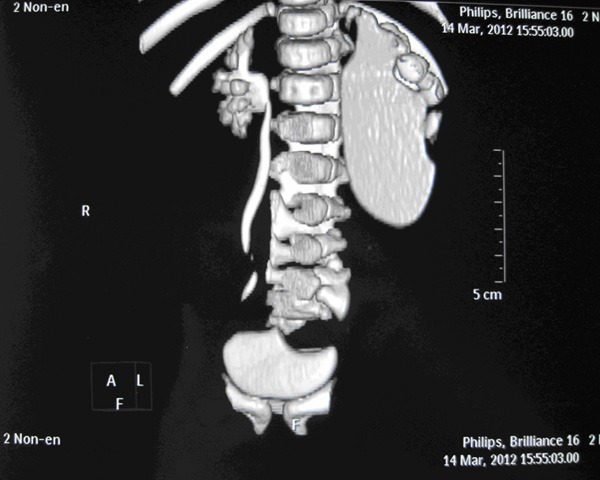
MRU indicated ureteropelvic junction obstruction in left kidney.
Figure 3.
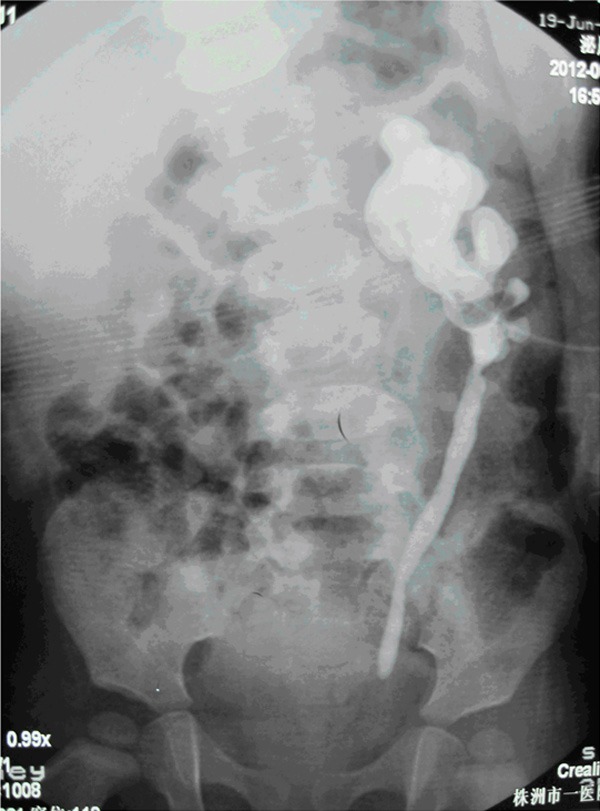
The Antegrade urography demonstrated that left double J had not arrived at the bladder, mild dilatation of the upper, middle ureter and distal ureteral atresia.
After two months, boari flap reconstruction was performed for the patient in our hospital and recovered well postoperatively. Intraoperative findings showed atresia of ureter length up to 5 cm long. Histopathological examination of the atresia part of the ureter shows a lot of lymphocytes and neutrophil infiltration and marked thickening of the smooth muscle (Figure 4).
Figure 4.
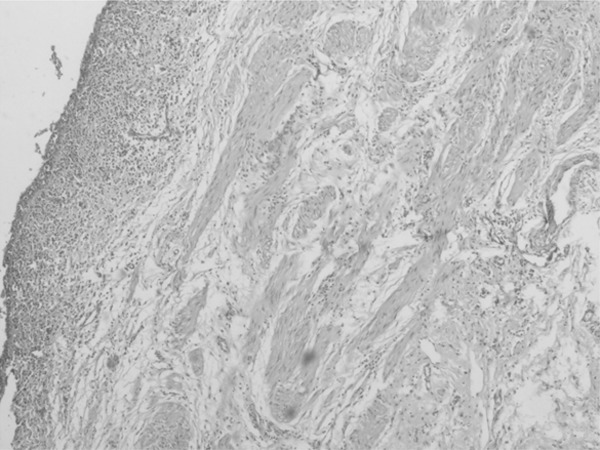
Histopathological examination of the atresia part of the ureter shows a lot of lymphocytes and neutrophil infiltration and marked thickening of the smooth muscle (H&E; original magnification, × 40).
Discussion
Distal ureteral atresia, one of the rarest congenital anomalies, represents a failure of the ureter to communicate with the bladder, and is commonly associated with a nonfunctioning kidney [3]. In this case, the renal parenchymal thickness was good when diagnosis was done because of the expanded extrarenal pelvis offset majority obstruction pressure, although there was a renal calyceal dilatation deformation. In general, the ureteral part above atresia should be obviously dilatation if the kidney is functional. In this case, ureteropelvic junction obstruction leads to the unobvious expansion of ureteral part above atresia, which caused the initial misdiagnosis. Although UPJ obstruction may also be resulted from acquired lesions such as vesicouretal reflux and megaloureter, which can lead to upper tract dilation with subsequent elongation, tortuosity, and kinking of the ureter [4], we would not consider the above situation in this circumstance. Ureteral atresia and UPJ obstruction are separate entities in this case. The two entities appeared simultaneously in the same patient, which is believed as the fist report in English literature by now.
In conclusion, we reported the first case of distal ureteral atresia with UPJ obstruction in a female child. Although distal ureteral atresia with UPJ obstruction is extremely rare, this entity should be suspect when the single disease cannot explain all symptoms or signs, especially ureteral catheter was placed unfavorably. There is no better way to diagnose preoperatively including MRU. Retrograde or Antegrade urography remains the gold standard for diagnosis of the disease.
Disclosure of conflict of interest
None.
References
- 1.Zundel S, Szavay P, Schaefer JF, Amon O, Fuchs J. Single kidney and ureteral atresia in a newborn girl: a treatment concept. J Pediatri Urol. 2011;7:576–8. doi: 10.1016/j.jpurol.2011.02.002. [DOI] [PubMed] [Google Scholar]
- 2.Morozumi M, Ogawa Y, Fujime M, Kitagawa R. Distal ureteral atresia associated with crossed renal ectopia with fusion: recovery of renal function after release of a 10-year ureteral obstruction. Int J Urol. 1997;4:512–5. doi: 10.1111/j.1442-2042.1997.tb00295.x. [DOI] [PubMed] [Google Scholar]
- 3.Karanastasis D, Antoniou N, Tsagatakis E, Sakalis K, Stenos I. Distal ureteral atresia associated with ipsilateral renal dysplasia. Scand J Urol Nephrol. 1992;26:77–9. doi: 10.3109/00365599209180401. [DOI] [PubMed] [Google Scholar]
- 4.Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA. Management of upper urinary tract obstruction. 10th edition. Philadelphia: WB Saunders; 2012. Campell-Walsh Urology; pp. 1122–3. [Google Scholar]