

Abstract
Effective strategies are required to reduce the prevalence of overweight and obesity; however, the effectiveness of current weight loss programmes is variable. One contributing factor may be the difference in weight loss success between men and women. A systematic review was conducted to determine whether the effectiveness of weight loss interventions differs between men and women. Randomized controlled trials published up until March 2014 were included. Effect sizes (Hedges' g) were used to examine the difference in weight outcomes between men and women. A total of 58 studies met the eligibility criteria with 49 studies of higher quality included in the final data synthesis. Eleven studies that directly compared weight loss in men and women reported a significant sex difference. Ten of these reported that men lost more weight than women; however, women also lost a significant amount of weight. Analysis of effect sizes found small differences in weight loss favouring men for both diet (g = 0.489) and diet plus exercise (g = 0.240) interventions. There is little evidence from this review to indicate that men and women should adopt different weight loss strategies. Current evidence supports moderate energy restriction in combination with exercise for weight loss in both men and women.
Keywords: Sex differences, systematic review, weight loss
Introduction
Overweight and obesity are now the fifth leading risk factors contributing to global mortality (1). In 2012, the Organisation for Economic Co-operation and Development (OECD) reported that in many countries, one in two people is overweight or obese (2). Each year, approximately 2.8 million adults die as a direct result of being overweight or obese (1). With the prevalence continuing to rise both in Australia (3) and worldwide (1), effective population-based strategies to reduce this burden need to be identified. Overweight and obesity are defined by excessive accumulation of body fat (1), often contributing to the development of chronic diseases such as cardiovascular disease (CVD) and type 2 diabetes (4). Weight loss remains the primary strategy for reducing the risks associated with overweight and obesity, but the effectiveness of weight loss programmes is variable, within and between programmes (5). One possible explanation for this variation could be the difference in weight loss success between men and women and the lack of direct comparison between them.
There are a number of characteristics that differ between men and women that may contribute to the difference in weight loss success. Characteristics favouring greater weight loss in men include a greater percentage of muscle mass compared with fat mass, contributing to higher resting and total energy expenditure (6,7) and a greater potential impact of exercise on weight loss (8). On the contrary, women have higher concentrations of leptin, an appetite regulation hormone that reduces energy intake (9). While research supports these points, there is still no consensus on whether these physiological mechanisms lead to differences in weight loss success between men and women. Other considerations contributing to weight loss variability between men and women include the study design and nature of the lifestyle interventions implemented in the current weight loss interventions.
There are a number of systematic reviews that have investigated the effectiveness of lifestyle interventions with a focus on either men or women, or men and women combined (10–14), but this is the first to focus on the differences in weight loss between men and women. A systematic review published in 2012 sought to determine intervention characteristics associated with weight loss and maintenance in men (14). The review by Young et al. found that a prescribed energy-restricted diet, frequent contact and group face-to-face contact were features associated with weight loss success in men. Young et al. also conducted a meta-analysis that demonstrated that weight loss interventions were effective compared with no-intervention controls (14). Another systematic review, published in 2013, sought to determine the effectiveness of weight management programmes in young women (13) and found that just over 60% of the studies (n = 8) reported a significant weight loss in the intervention groups compared with controls. However, with few studies identified, the authors could not determine a particular type of intervention that was more beneficial for weight loss (13). Of the studies conducting reviews of men and women combined, reduced energy diets, diet plus exercise, weight loss medications and weight loss surgery have been found to be effective for weight loss, with advice-only or exercise-only interventions less effective (10–12). Although pharmacotherapy and surgical interventions have been shown to result in large weight losses (15–18), the safety of weight loss medications and the sustainability of surgery as a population-based strategy have come under scrutiny, along with the cost of these options, both short- and long-term (19). Therefore, this current review will address only lifestyle interventions, such as diet and exercise, along with meal replacements and nutritional supplements, given these are widely used in conjunction with lifestyle interventions.
Although published literature on weight loss interventions is vast, there is still no consensus on which lifestyle interventions are best for weight loss, particularly for men or women. Therefore, the aim of this review was to determine whether the effectiveness of particular weight loss interventions differs between men and women, and if they do, which are more effective for men or for women.
Methods
Study selection
Only randomized controlled trials (RCTs) were eligible for inclusion. Studies were required to have included both male and female participants, ≥18 years of age, with a body mass index (BMI [kg m−2]) ≥ 25, and to report weight change for both men and women separately. Studies were included if participants had existing co-morbidities associated with overweight and obesity such as type 2 diabetes and CVD, but excluded if they were taking medications known to influence weight (e.g. hypoglycaemic agents) or were diagnosed as having an eating disorder. Studies were required to have a primary aim of weight loss. Eligible interventions included diet (whole foods, meal replacements or natural supplements) and/or physical activity (PA) prescriptions. Interventions that were surgical or used pharmacological agents as methods of weight loss were excluded. This review considered overweight/obesity-related outcomes such as change in weight (kg), change in BMI (kg m−2), change in waist circumference (cm), percent weight loss and percent body fat loss.
Search strategy
Published and unpublished studies until March 2014 were identified from a literature search of nine online databases. Databases included Medline, Embase, PsycINFO, CINAHL, Web of Science, Scopus, Cochrane Library, DARE, and Dissertations and Theses. Bibliographies of selected studies were also searched. The undertaking of this review adhered to PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines (20). The first phase of study identification included assessment of study inclusion based upon the title and abstract. Full texts were retrieved for those papers seen to meet inclusion criteria from the title and abstract. Two assessors independently decided on inclusions based upon the full texts. If there was disagreement, a third independent reviewer was used.
Search terms included (overweight OR ‘over weight’ OR obes*), (‘weightloss’ OR ‘weightchange’ OR ‘weightreduc*’), (‘randomisedcontrolledtrial’ OR ‘clinicaltrial’ OR ‘randomizedcontrolledtrial’), (male* AND female*).
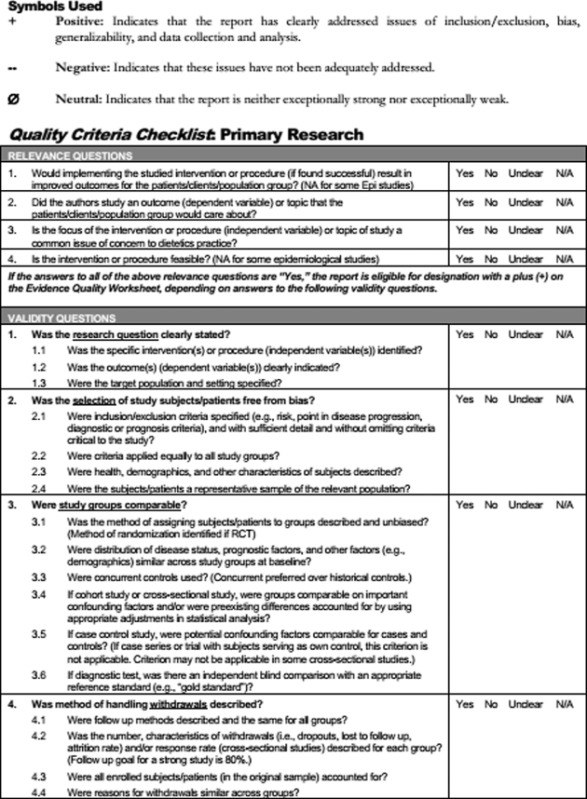
Assessment of methodological quality
Two independent reviewers assessed the methodological quality of studies using a critical appraisal tool from the American Dietetic Association (Appendix 1) (21). A third reviewer was consulted if there was discrepancy. If most (six or more) of the answers to the validity questions were ‘No’, the study was designated with a minus (−); if the answers to questions 2, 3, 6 and 7 did not indicate that the study was exceptionally strong, the report was designated with a neutral (Ø) symbol; and if most of the answers to the all validity questions were ‘Yes’ (including criteria 2, 3, 6, 7 and at least one additional ‘Yes’), the study was designated with a plus symbol (+).
Data collection and synthesis
Data extraction was performed by one reviewer using a standardized form developed by the researchers. Extraction was checked for accuracy and consistency by a second reviewer. Participant and intervention characteristics were extracted as well as data in relation to weight-related outcomes. All data were described in narrative synthesis, and where possible, effect sizes for the effect of interventions on the difference in absolute weight loss, percent weight loss and change in BMI between men and women were calculated. Any study where mean change and standard deviation were reported separately for men and women was included in this calculation. For results presented with standard errors or confidence intervals, standard deviations were calculated from these values (22). For each intervention, the data and effect size were reported separately. The primary interventions investigated were diet alone, exercise alone and diet plus exercise. Effect sizes were calculated for these interventions using Hedges' g equation to assess the difference in mean weight loss between men and women using a weighted standard deviation (by group sample size) (23) to account for the differences in the proportion of men and women in each study. Results were interpreted using effect size definitions described by Cohen et al., with an effect size of 0.2 defined as small, 0.5 medium and 0.8 large (24). Additionally, if studies were sufficiently similar and change scores were reported and presented as means with standard deviations, data were pooled in a meta-analysis using Review Manager 5.1 Analyses (25). To determine the most appropriate meta-analysis model, statistical heterogeneity was assessed using chi square with a significant heterogeneity assigned at P < 0.05. If significant heterogeneity existed, the random effects model was used for statistical analysis; if homogeneous, the fixed effect model was used.
Results
The initial search identified 7,739 potential studies. A total of 68 papers representing 58 studies met all the inclusion criteria (Fig. 1). There were 50 studies excluded for not reporting data to support statements made regarding sex-specific intervention effectiveness or differences between men and women. Of these 50 excluded studies, 44 reported that sex was not a predictor of weight change.
Figure 1.
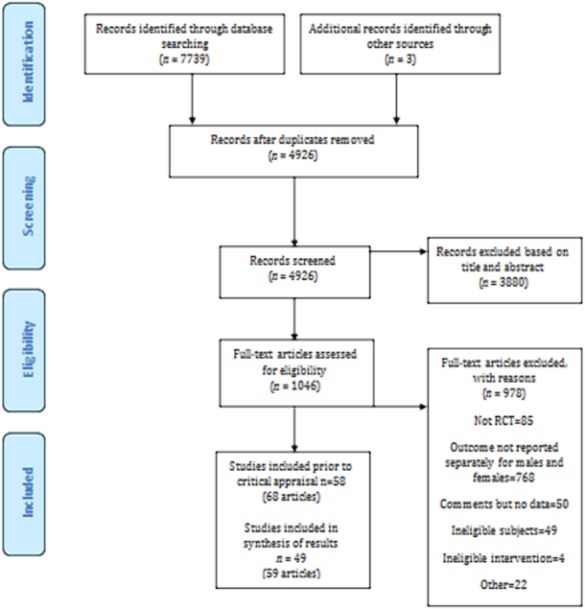
Flow chart of study selection.
Study characteristics
Table S1 summarizes the characteristics of each included study (n = 58) (irrespective of critical appraisal). Characteristics include sample size and proportion of men vs. women, age, weight status, the duration of the study, description of the intervention and retention rate.
Eighteen studies (31%) were published before 1999 (26–43) with the remaining (69%) published from 2000 onwards (44–84). Of the 58 studies, 32 (55%) were conducted in the USA (26,27,29,30,32–37,39,41,43–45,49–52,54,57,60,62,65,72,75,76,78–80,83,84); 7 in Australia (47,53,58,59,61,63,73); 3 in Canada (28,42,67); 2 in each of China (74,77) and Denmark (82,85); and 1 each in Italy (69), Norway (64), Iceland (70), Israel (68), Sweden (38), the Netherlands (71), Finland (31), Japan (81), Germany (40), Spain (46) and Turkey (48), with one study conducted as a multi-country study (Iceland, Ireland and Spain) (66).
There were 15,341 participants across the 58 included studies. Individual study sample sizes varied markedly ranging from 8 (26) to 2,921 (84) participants, with 48% (n = 28) of the studies having 100 or less participants. The percentage of women within study samples ranged from 14% (68) to 91% (28), and of those reporting sex distribution, 71% (n = 41) had >50% female distribution, with 21% (n = 13) having ≥70% female distribution. Only five studies had more men than women (26,46,49,68,73), and only one of these had >70% male. Of the studies that reported the age of men and women separately, the mean age of male participants ranged from 22 (52) to 63 years (62) and female participants from 21 (52) to 65 (62) years. BMI (kg m−2) for male participants ranged from 27 kg m−2 (51) to 43 kg m−2 (31) and female participants from 26 kg m−2 (51) to 44 kg m−2 (31). The duration of active weight loss interventions ranged from 6 weeks (78) to 24 months (31,38,68,86,87), with six studies conducting further follow-up (31,40,59,65,81,84).
Critical appraisal
Studies were assessed for quality (Table S2) using a critical appraisal tool developed by the Academy of Nutrition and Dietetics (21). The average quality score was positive with nine studies classed as negative. Any study found to be of negative quality was excluded from the remainder of the review, leaving a total of 49 studies included. Of the 49 studies still included following critical appraisal, the criteria not met by more than 50% were those pertaining to blinding of allocators and appropriate statistical analysis. Other quality criteria that were poorly met were the description of biases and limitations and also whether bias was due to funding (<65% of studies met these criteria).
Outcomes and interventions
Of the final 49 studies, 33 reported multiple weight outcomes and 16 reported a single weight outcome (Table S3). Weight change (kg) or weight (kg) as baseline and final values were the primary weight outcomes reported by the majority of studies (n = 45/49). Weight change as a percentage of baseline weight was reported by only 10 studies. Nineteen of the 49 studies reported change in fat mass (kg/lb/%) and 14 studies reported change in fat-free mass (kg/lb/%) or volume (L). Seventeen of the 49 studies reported changes in waist or hip circumference or waist to hip ratio, and 15 reported either change in BMI (kg m−2) or BMI as baseline and final values. Change in site-specific fat distribution (visceral/subcutaneous) was reported in 6 of the 49 studies. Three studies reported reaching goal weight as an additional outcome.
Of the 49 studies, 34 made a single comparison (two groups), while 15 made multiple comparisons. Of the 34 making a single comparison, 19 compared similar interventions (i.e. diet vs. diet). Of these, 10 compared dietary interventions (27,35,46,53,58,61,72,78,82,83), 2 compared PA (48,49) and 7 compared combinations of diet and PA interventions (31,45,50,62,63,65,79). Two studies compared different interventions (i.e. diet vs. diet plus meal replacements) (38,40). The remaining studies (n = 13) compared intervention to control (26,30,34,36,37,44,47,52,54,59,64,67,71,76,77,81,84). The intervention groups in these studies consisted of PA (n = 1) (52), combined diet and PA (n = 7) (34,36,37,59,71,81,84), and supplements (n = 5) (26,47,64,67,77). Three of the supplement groups received the supplement plus dietary intervention. The control groups were either minimal interventions (n = 5), true controls (n = 3) or placebo (n = 5; 3 of these received dietary intervention as well as placebo). Of the 15 studies comparing multiple interventions, there were 14 dietary interventions, 2 exercise interventions, 27 diet plus exercise interventions, 1 supplement group and 7 controls (2 minimal intervention, 4 true controls and 1 placebo).
Overall, diet plus exercise and diet alone were the main interventions investigated (diet and exercise groups [n = 48]; diet groups [n = 36], exercise groups [n = 7], supplement groups [n = 6] and control groups [total n = 19: minimal intervention n = 7; true control n = 6; placebo n = 6]).
Effectiveness of interventions
The effectiveness of interventions for men and women was reported in two ways. Twenty-one studies directly compared the weight loss responses of men and women. Of these studies, 11 reported significant differences between men and women for change in weight (34,36,46,50,53,61,65,68,73,79). The remaining studies reported that there were no significant differences in weight change between men and women. The second approach reported the effects of the interventions on men and women separately (i.e. within sex group effects) but there was no statistical comparison of the magnitude of these responses. Twenty-nine studies reported within sex effects and 28 studies reported significant intervention effects within men and/or women (29,31,35,37–40,42,45,47,48,52,54,58,59,61,62,64,66,67,71,76,77,79,81,83,84,86). The one remaining study reported that there were no significant intervention effects for either sex (49). Six studies did not report whether the differences were significant (26,27,30,75,80,82).
Direct comparison of differences between men and women
Overview
Overall, of the 11 studies reporting significant male vs. female sex differences in weight (kg or %) change (34,36,46,50,53,61,65,68,73,79,84), 10 reported that men lost significantly more weight (kg) than women (34,36,46,50,53,61,65,73,79,84); one study reported that men lost significantly more weight than women with one intervention but women lost significantly more weight than men in another intervention group (68). Of these 11 studies, 4 investigated the effectiveness of dietary interventions (46,53,61,68), 6 investigated the effects of combined diet and exercise prescription (29,31,50,65,79,84) and 1 reported between sex differences for a combination of interventions but not for each intervention (73).
Effectiveness of diet only interventions
Four studies investigated between sex differences for the effects of dietary interventions on weight loss (46,53,61,68). The mean difference in weight loss between men and women ranged from 1.2 kg (68) to 3.5 kg (53); the mean weight losses for men ranged from 4.1 to 10.8 kg and for women from 2.9 to 7.8 kg. The duration of the active weight loss interventions ranged from 5 weeks (46) to 24 months (68).
The first study (53,56) compared a standard protein (SP; 15% protein, 55% carbohydrate, 30% fat) diet to a high protein (HP; 30% protein, 40% carbohydrate, 30% fat) diet over 16 weeks (12-week weight loss, 4-week weight loss maintenance). Men in both groups lost significantly more weight than women (P = 0.003); however, when expressed as a percentage of baseline weight, this difference was no longer significant. Additionally, men lost significantly more fat mass (P < 0.03) and fat-free mass (P < 0.02) than women.
The second study (61,88) also compared an SP diet to HP diet over 16 weeks but with different macronutrient distributions to the previous study (SP: 40% protein, 30% carbohydrate, 30% fat; HP: 20% protein, 30% carbohydrate, 50% fat). Again, both men and women lost weight, but overall, men lost significantly more weight (kg and %) than women ([11 kg vs. 8 kg; P = 0.028]; [2% greater wight lost in men; P = 0.03]). Men also lost significantly more abdominal fat mass than women (P = 0.039).
Another study that investigated the effects of macronutrients on weight compared three diet arms over 24 months (68). The three arms were low-fat calorie-restricted diet (30% fat, 1,500–1,800 kcal), a calorie-restricted Mediterranean diet (35% fat, 1,500–1,800 kcal) and a low carbohydrate diet with no calorie restriction (20 g carbohydrate). Men lost significantly more weight (kg) than women in interventions 1 (3.3-kg difference; P < 0.001) and 3 (2.5-kg difference; P < 0.001); however, women lost more weight in intervention 2 (2.2-kg difference; P < 0.001). When baseline weight was adjusted for in the analysis, these treatment differences by sex were no longer significant.
The final study compared two intervention arms over 8 weeks (46); one group was prescribed a diet composed of seven meals per day with a macronutrient distribution of 40% total energy from carbohydrates, 30% from proteins and 30% from fats, and the second group was instructed to consume three to five meals per day with a macronutrient distribution of 50–55% total energy from carbohydrates, 15% from proteins and 30% from fats (46). Both groups were requested to improve healthy fatty acid profiles, increase intake of fiber to 20–25 g d−1 and reduce cholesterol <300 mg d−1. Men lost significantly more weight (kg) than women in both intervention groups (group 1: 1.2 kg difference; group 2: 2.0 kg difference; P < 0.007).
Effectiveness of combined diet and exercise interventions
Six studies investigated sex differences in the effectiveness of diet and exercise interventions (34,36,50,65,79,84). Of those reporting weight loss (kg), the mean difference between men and women ranged from 1.4 kg (50) to 3.9 kg (65), with the mean weight losses for men ranging from 4.2 to 7.3 kg and for women from 0.3 to 5.9 kg. The duration of the active weight loss interventions ranged from 12 weeks to 18 months (36,65).
The first study compared two intervention groups, one high protein (HP) and one low protein (LP) (79). Participants were recommended 30-min walking, 5 d week−1 and attended weekly educational sessions for the duration (79). With results from both interventions pooled, men lost significantly more weight than women (M 2.7 kg > F; P = 0.04) after 4 months; however, when expressed as a percentage of baseline weight, this was no longer significant.
Andersen et al. (50) compared two exercise programmes with both groups following the same calorie-restricted diet. One group performed moderate-vigorous aerobic activity for 45 min, 3–4 d week−1 with the other group performing moderate PA (mostly walking) for 30 min 5 d week−1. Men lost significantly more weight (kg) than women (−7.3 ± 3.3 vs. −5.9 ± 2.9; P = 0.027) over the 12 weeks (50).
The next study (61) of 30-month duration consisted of an 18-month weight loss phase with 12-month passive follow-up. The two intervention groups were prescribed the same type of exercise; however, group 1 had an exercise energy expenditure goal of 1,000 kcal week−1 and group 2 of 2,500 kcal week−1. Both groups were instructed to consume an energy-restricted diet of 1,000–1,500 kcal d−1. There was no difference between the interventions so data were pooled to examine sex differences. Men had significantly greater weight loss (kg) than women (−4.2 ± 7.1 vs. −0.29 ± 9.5; P-value not reported) at 30 months (61).
Stevens et al. (34) compared a diet and exercise intervention group to a no-intervention control group over a 6-month weight loss phase and 12-month weight loss maintenance. The intervention group was asked to reduce calorie intake to no less than 1,200 kcal d−1, prescribed an exercise goal of 30–45 min of moderate intensity PA on 4–5 d week−1, and attended behaviour change sessions (goal setting, self-monitoring, relapse prevention). The control group maintained their normal diet and exercise patterns. Men in the intervention group lost significantly more weight (kg) than women in the intervention group from baseline to post-weight loss phase (M −6.5 vs. F −3.7; P < 0.01), post-weight loss to mid-weight maintenance phase (M −5.6 vs. F −2.7; P < 0.01) and post-weight maintenance phase (M −4.7 vs. F −1.6; P < 0.01). When expressed as a percentage of baseline weight, these differences remained significant at each time point (P < 0.05) (34).
Wing et al. (36) compared a diet and exercise intervention of calorie restriction (1,000–1,500 kcal d−1), with an emphasis on increasing complex carbohydrates and decreasing fat, and an exercise goal of 1,000 kcal week−1 and educational sessions to a minimal intervention group that received diet and exercise information (no prescription) but did not attend any sessions (36). Men in the intervention group lost a significantly greater amount of weight (kg) at 6, 12 and 18 months (6 months −11.3 vs. −8.4; 12 months −8.5 vs. −6.3; 18 months −7.3 vs. −4.6; P < 0.05) and body fat (%) at 6 and 18 months (6 months −7.2 vs. −5.2; 18 months −4.7 vs. −3.1; P < 0.05) than women in the intervention group.
The final study (84) of 30-month duration compared an intensive lifestyle intervention of diet and PA with individual fortnightly visits for the first 6 months, then monthly to bi-monthly for the remaining duration, to a minimal intervention group who had annual visits only. The lifestyle intervention included goals of 7% reduction in weight, at least 150 min of moderate PA per week, and a reduction of dietary fat to 25% of total energy intake. Overall, women in the lifestyle group had a significantly lower weight loss than men. When results were reported for the six sex-race groups (Caucasian men, Caucasian women, African-American men, African-American women and Hispanic men and Hispanic women), African-American women had a significantly lower percent weight loss than all other sex-race groups (−2.0 ± 6.2; P < 0.01), except for African-American men (P = 0.356); however, the weight loss of African-American men was not significantly different from any other sex-race group.
Multiple interventions
The final study compared three groups over 12 weeks: diet alone, diet and exercise, or no-intervention control. Both intervention groups were prescribed a modified Dietary Approach to Stop Hypertension (DASH) diet plan with a 600 kcal d−1 energy restriction. The exercise consisted of 40 min of cycling on an ergometer on alternate days at 65% maximum heart rate. The control group was advised not to change their diet or PA for the 12 weeks but visited the research clinic for assessment sessions. Pooled data from the two interventions and one control showed that men had a significantly greater weight loss (kg) (−8.8 ± 0.8 vs. −6.2 ± 0.8; P < 0.05) than women (73).
Effect sizes comparing changes in weight outcomes between men and women
Effect sizes to compare the differences in absolute weight loss achieved by men and women for diet alone, exercise alone or diet plus exercise are shown in Table 1a. Additional effect sizes were calculated for percent weight change and change in BMI to determine if effect sizes remained the same after adjusting for baseline weight and body composition (Table 1b). For absolute weight loss, the mean effect sizes for diet (Hedges' g: −0.489) were moderate and diet-plus-exercise interventions (Hedges' g: −0.240) were small, although the difference in weight loss between men and women ranged from trivial to large. There was no difference in weight loss between men and women using exercise alone (Hedges' g: −0.105). Effect sizes for percent weight change were small for dietary interventions (Hedges' g: −0.254) and diet plus exercise interventions (Hedges' g: −0.225). However, an increase from no difference to a small difference favouring women was found for exercise only interventions (Hedges' g: −0.339). For change in BMI, all intervention categories showed no difference between men and women (Hedges' g: diet −0.183; diet plus exercise −0.072; exercise 0.153). For those studies that reported mean change (irrespective of significance) in absolute weight, percent weight and change in BMI, an illustration can been seen in Fig. 2.
Table 1a.
Mean weight changes in men and women plus effect size for the difference between men and women within intervention groups
| Intervention | Study | Men |
Women |
Hedge's g | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Diet alone | Bowen et al. (a), 2005 (58) | −9.4 | 4.1 | −9.4 | 3.9 | 0.000 |
| Bowen et al. (b), 2005 (58) | −12 | 4.7 | −7.8 | 2.3 | −1.220 | |
| Ditschuneit et al. (a), 1999 (40) | −8.4 | 3.9 | −6.8 | 3.3 | −0.464 | |
| Ditschuneit et al. (b), 1999 (40) | −1.1 | 2.6 | −1.2 | 2.1 | 0.046 | |
| Dow et al. 2012 (78) | −0.3 | 2.1 | −0.6 | 1.8 | 0.189 | |
| Farnsworth et al. (a), 2003 (53) | −9.6 | 1.7 | −7.4 | 0.5 | −2.373 | |
| Farnsworth et al. (b), 2003 (53) | −11.4 | 2.1 | −6.6 | 0.5 | −4.364 | |
| Thorsdottir et al. (a), 2008 (66) | −6.5 | 2.8 | −4.4 | 2.3 | −0.830 | |
| Thorsdottir et al. (b), 2008 (66) | −7 | 3.5 | −3.9 | 2.3 | −1.047 | |
| Janssen and Ross 1999 (42) | −11.7 | 3.5 | −10.7 | 3.8 | −0.270 | |
| Lopez-Legarrea et al. (a), 2013 (46) | −7.7 | 2.6 | −6.5 | 3.1 | −0.419 | |
| Lopez-Legarrea et al. (b), 2013 (46) | −7.6 | 3.3 | −5.6 | 2.5 | −0.671 | |
| Luscombe-Marsh et al. (a), 2005 (61) | −11.2 | 6.1 | −7.9 | 5.4 | −0.577 | |
| Luscombe-Marsh et al. (b), 2005 (61) | −10.5 | 5.9 | −7.8 | 3.2 | −0.592 | |
| Shea et al. 2011 (76) | −5.3 | 4.8 | −4.6 | 4.2 | −0.156 | |
| Stocks et al. 2012 (82) | −7.9 | 3.8 | −6.5 | 3.2 | −0.412 | |
| St-Onge et al. (a), 2012 (83) | −5.6 | 1.5 | −3.4 | 2 | −1.180 | |
| St-Onge et al. (b), 2012 (83) | −2.9 | 1.5 | −3.3 | 2.2 | 0.203 | |
| Torgerson et al. (a), 1997 (38) | −15.5 | 17.2 | −5.6 | 11 | −0.728 | |
| Torgerson et al. (b), 1997 (38) | −5.3 | 9.8 | −6.8 | 9.3 | 0.158 | |
| Wood et al. (a), 1991 (29) | −5.1 | 5.8 | −4.1 | 5.5 | −0.175 | |
| Mean weight loss | −7.7 | – | −5.8 | – | – | |
| Pooled*effect size | – | – | – | – | −0.489 | |
| Exercise alone | Donnelly et al. (a), 2013 (44) | −3.8 | 5.7 | −4.1 | 4.3 | 0.060 |
| Donnelly et al. (b), 2013 (44) | −5.9 | 6.6 | −4.4 | 4.2 | −0.270 | |
| Mean weight loss | −4.9 | – | −4.3 | – | – | |
| Pooled*effect size | – | – | – | – | −0.105 | |
| Diet + exercise | Andersen et al. 2002 (50) | −7.3 | 3.3 | −5.9 | 2.9 | −0.467 |
| Byrne et al. 2006 (63) | −7.3 | 2.2 | −5.7 | 3.9 | −0.516 | |
| Dansinger et al. 2005 (60) | −3.3 | 6.4 | −2.4 | 5.1 | −0.155 | |
| De Jonge et al. 2012 (86) | −7.6 | 5.1 | −5.9 | 6.1 | −0.293 | |
| Gabriele et al. (a), 2011 (75) | −6.7 | 5.3 | −2.4 | 3 | −1.274 | |
| Gabriele et al. (b), 2011 (75) | −6.6 | 6.6 | −2.5 | 3.4 | −0.983 | |
| Gabriele et al. (c), 2011 (75) | −3.4 | 5.9 | −4.5 | 3.7 | 0.273 | |
| Gorin et al. (a), 2013 (45) | −10 | 10.5 | −4.2 | 9.7 | −0.588 | |
| Gorin et al. (b), 2013 (45) | −4.6 | 10.6 | −8.1 | 9.8 | 0.351 | |
| Hakala et al. (a), 1993 (31) | −1.8 | 7.4 | −5.4 | 10.9 | 0.363 | |
| Hakala et al. (b), 1993 (31) | −15.6 | 12 | −10.4 | 13.4 | −0.402 | |
| Janssen and Ross (a), 1999 (42) | −12.7 | 3.8 | −10 | 2.8 | −0.809 | |
| Janssen and Ross (b), 1999 (42) | −11.4 | 3.8 | −11.5 | 3.2 | 0.028 | |
| Jeffery et al. (a), 2003 (54) | −2.6 | 5.7 | −1.7 | 4.1 | −0.193 | |
| Jeffery et al. (b), 2003 (54) | −3.8 | 5.7 | −1.9 | 18.7 | −0.116 | |
| Stewart et al. 2005 (62) | −2.2 | 2.7 | −2.3 | 3.4 | 0.032 | |
| Tate et al. 2007 (65) | −4.2 | 7.1 | −0.3 | 9.5 | −0.453 | |
| ter Bogt et al. 2009 (71) | −2.1 | 4.8 | −1.5 | 4.1 | −0.133 | |
| West et al. (a), 2008 (84) | −5.7 | 7.6 | −4.2 | 7.5 | −0.199 | |
| West et al. (b), 2008 (84) | −4.8 | 3.5 | −2.1 | 6.3 | −0.465 | |
| West et al. (c), 2008 (84) | −6.3 | 6.6 | −5.1 | 8.3 | −0.154 | |
| Williams et al. (a), 1998 (39) | −1.5 | 6.9 | −7.8 | 3.7 | 1.283 | |
| Williams et al. (b), 1998 (39) | −11.6 | 5 | −7 | 5.7 | −0.866 | |
| Williams et al. (c), 1998 (39) | −14.7 | 5.5 | −8.2 | 4.1 | −1.420 | |
| Wood et al. (b), 2001 (29) | −8.7 | 5.7 | −5.1 | 5.3 | −0.655 | |
| Mean weight loss | −6.7 | – | −5.1 | – | – | |
| Pooled*effect size | – | – | – | – | −0.240 | |
| Overall pooled†effect size | – | – | – | – | −0.315 | |
Pooled effect sizes for intervention type.
Overall pooled diet; exercise and diet + exercise effect size; effect size of 0.2 defined as small, 0.5 medium and 0.8 large.
The effect sizes are weighted based upon the sample sizes of men and women.
Table 1b.
Mean percent weight changes and changes in body mass index (BMI) in men and women plus effect size for the difference between men and women within intervention groups
| Percent weight change | ||||||
|---|---|---|---|---|---|---|
| Intervention | Study | Men |
Women |
Hedge's g | ||
| Mean | SD | Mean | SD | |||
| Diet alone | Evans et al. (a), 2012 (79) | −9 | 3.4 | −8.3 | 3.2 | −0.213 |
| Evans et al. (b), 2012 (79) | −8.5 | 4 | −7.3 | 3.8 | −0.309 | |
| Mean percent weight loss | −8.8 | – | −7.8 | – | – | |
| Pooled*effect size | – | – | – | – | −0.254 | |
| Exercise alone | Sanal et al. (a), 2013 (48) | −4.6 | 2.5 | −4 | 2.4 | −0.245 |
| Sanal et al. (b), 2013 (48) | −3 | 2.8 | −5.3 | 3 | 0.906 | |
| Mean percent weight loss | −3.8 | – | −4.7 | – | – | |
| Pooled*effect size | – | – | – | – | 0.339 | |
| Diet + exercise | Gabriele et al. (a), 2011 (75) | −6.8 | 5.2 | −3 | 3.8 | −0.950 |
| Gabriele et al. (b), 2011 (75) | −6.7 | 7.1 | −2.9 | 4 | −0.805 | |
| Gabriele et al. (c), 2011 (75) | −3.4 | 5.8 | −5.3 | 4 | 0.349 | |
| ter Bogt et al. 2009 (71) | −2.1 | 4.8 | −1.7 | 4.9 | −0.082 | |
| West et al. (a), 2008 (84) | −5.8 | 7.1 | −4.5 | 7.6 | −0.175 | |
| West et al. (b), 2008 (84) | −5.1 | 3.7 | −2 | 6.2 | −0.539 | |
| West et al. (c), 2008 (84) | −6.5 | 6.3 | −5.9 | 9.2 | −0.072 | |
| Mean percent weight loss | −5.2 | – | −3.6 | – | – | |
| Pooled* effect size | – | – | – | – | −0.225 | |
| Overall pooled†effect size | – | – | – | – | −0.193 | |
| Change in BMI | ||||||
|---|---|---|---|---|---|---|
| Intervention | Study | Men |
Women |
Hedge's g | ||
| Mean | SD | Mean | SD | |||
| Diet alone | Thorsdottir et al. (a), 2008 (66) | −2.1 | 0.9 | −1.6 | 0.8 | −0.591 |
| Thorsdottir et al. (b), 2008 (66) | −2.2 | 1.1 | −1.4 | 0.9 | −0.796 | |
| Janssen and Ross 1999 (42) | −3.8 | 0.9 | −4 | 1.3 | 0.179 | |
| Lopez-Legarrea et al. (a), 2013 (46) | −2.5 | 1.1 | −2.6 | 0.1 | 0.128 | |
| Lopez-Legarrea et al. (b), 2013 (46) | −2.6 | 1.1 | −2.3 | 1 | −0.284 | |
| Luscombe-March et al. (a), 2005 (61) | −3.6 | 2.2 | −3.1 | 1.2 | −0.292 | |
| Luscombe-March et al. (b), 2005 (61) | −3.6 | 2.1 | −2.9 | 1.9 | −0.352 | |
| Stocks et al. 2012 (82) | −2.5 | 1.2 | −2.4 | 1.2 | −0.083 | |
| Mean BMI change | −2.9 | – | −2.5 | – | – | |
| Pooled* effect size | – | – | – | – | −0.183 | |
| Exercise alone | Donnelly et al. (a), 2013 (44) | −1.2 | 1.8 | −1.5 | 3.1 | 0.118 |
| Donnelly et al. (b), 2013 (44) | −1.9 | 3.9 | −1.6 | 3.1 | −0.085 | |
| Sanal et al. (a), 2013 (48) | −4.8 | 2.7 | −4.1 | 2.5 | −0.269 | |
| Sanal et al. (b), 2013 (48) | −3.1 | 2.8 | −5.3 | 3 | 0.867 | |
| Mean BMI change | −2.8 | – | −3.1 | – | – | |
| Pooled* effect size | – | – | – | – | 0.153 | |
| Diet + exercise | De Jonge et al. 2012 (86) | −3 | 1.8 | −2.6 | 1.8 | −0.222 |
| Janssen and Ross (a), 1999 (42) | −3.7 | 1.3 | −4.2 | 1.3 | 0.385 | |
| Janssen and Ross (b), 1999 (42) | −4 | 1.3 | −3.7 | 0.9 | −0.268 | |
| Stewart et al. 2005 (62) | −0.8 | 0.9 | −0.9 | 1.3 | 0.089 | |
| Mean BMI change | −3.9 | – | −3.5 | – | – | |
| Pooled* effect size | – | – | – | – | −0.072 | |
| Overall pooled†effect size | – | – | – | – | −0.131 | |
Pooled effect sizes for intervention type.
Overall pooled diet; exercise and diet + exercise effect size; effect size of 0.2 defined as small, 0.5 medium and 0.8 large.
The effect sizes are weighted based upon the sample sizes of men and women.
Figure 2.

Mean changes in absolute weight loss, percent weight loss and body mass index (BMI) in men and women in those studies reporting mean data.*Significant difference between men and women. #No significant difference between men and women.
Meta-analyses comparing changes in weight outcomes between men and women
In addition to the above effect sizes, meta-analyses were also conducted to investigate the differences in change in weight outcomes between men and women (Supporting information Fig. S1a–c). Meta-analysis showed that when comparing the difference in absolute weight loss in men and women for diet-only, exercise-only and combined diet and exercise interventions, weight loss was significantly greater for men in the diet-only and diet plus exercise interventions. When meta-analysis was conducted for percent weight change, greater percent weight loss was still significant in men for the diet plus exercise interventions but not diet-only; however, this is possibly due to the small number of diet-only studies. Meta-analysis of change in BMI for each of the intervention categories showed that men had a significantly greater reduction in BMI in the diet-only interventions; however, change in BMI for exercise-only and diet plus exercise interventions were not different between men and women.
Characteristics of studies with insignificant between sex differences
Of the 10 studies (42,44,47,48,60,63,70,72,78,86) that reported no sex differences in weight loss, men tended to have slightly greater improvement in weight outcomes than women but not sufficient to reach statistical significance. The duration of these studies ranged from 6 weeks to 24 months. Within these 10 studies, sex differences in weight loss were compared in 25 interventions (diet plus exercise, n = 12; diet-only, n = 8; exercise-only, n = 4; supplement, n = 1).
Effectiveness of interventions for men and women reported separately
Significant within sex differences were reported in 28 studies (29,31,35,37–40,42,45,47,48,52,54,58,59,61,62,64,66,67,71,76,77,79,81,83,84,86), and of these, 17 compared differences in weight loss between intervention groups (29,31,35,38–40,45,47,52,54,59,66,71,76,81,83,84) and four reported differences for each intervention but did not compare interventions (48,58,62,66,67). Within the first 17 studies, the following comparisons were made (24 interventions within 17 studies): diet plus exercise vs. minimal intervention (n = 6); diet plus exercise vs. control (n = 2); diet plus exercise vs. diet plus exercise (n = 3); diet plus exercise vs. diet (n = 1); diet vs. control (n = 1); diet vs. minimal intervention (n = 1), diet vs. diet (n = 3); diet plus meal replacements vs. diet (n = 2); exercise vs. control (n = 1), diet vs. placebo (n = 2) and supplement vs. placebo (n = 2). The four reporting results for each intervention but not directly comparing interventions reported both men and women lost significant amounts of weight in diet-only, exercise-only, diet plus exercise and supplement interventions. Supporting information Table S4 shows the comparisons of interventions that were effective for men and/or women. The remaining seven studies reported significance for pooled intervention data; therefore, information on the effectiveness of individual interventions could not be extracted. However, of these studies, four reported that both men and women lost a significant amount of weight and the other three reported only women lost a significant amount of weight.
As within sex differences do not directly answer our research question, these results are not discussed further.
Discussion
This is the first systematic review investigating whether particular weight loss interventions are more effective for men than women or vice versa. In total, the results of 49 studies were consolidated in order to address this question. The interest in sex differences in weight loss resulting from lifestyle interventions has grown in recent years, with 65% (n = 32) of the final 49 included studies conducted since the year 2000 and over 40% of these conducted in the last 4 years.
After methodological evaluation of study quality, nine studies assessed as having very poor methodological quality were excluded. With the release of the Consolidated Standards of Reporting Trials (CONSORT) statement in 1996 (89) and updates released in both 2001 and 2010, it is surprising to see studies still not meeting the criteria during quality assessment. Of these nine excluded studies, five were conducted after 1996 with two as late as 2009/2010. However, the overall quality of the studies included in this review was generally positive (n = 27/49). The main areas for improvement were description of the method of handling withdrawals, blinding of assessors, conducting appropriate statistical analysis, description of study limitations and whether bias occurred due to funding.
The average sample size of studies in this review was 265 participants; however, 43% had fewer than 100 and a number of studies had as few as 30. When investigating sex differences, larger numbers are required as sample sizes are essentially halved during statistical analysis. A small sample size leads to lower power, which reduces ability to conclude that results are valid, reliable and generalizable (90). Although all studies in this review included men and women, there were a number of studies that had low proportions of either men or women in comparison to the other sex; therefore, results from these unmatched studies need to be treated with caution. One study in particular reported that men lost significantly more weight than women; however, the proportion of women in this sample was only 14% (68). On the contrary, over 70% of the studies in this review had less than 50% of men in their sample and more than 20% of studies had less than 30% men. Similar results have been reported previously. A review of weight loss trials in men found that study samples were predominantly women, with, on average, only 23% of men (91). This variation in sample size of men and women within studies contributes to the difficulty in determining whether sex differences in weight loss exist.
The length of studies ranged from 6 weeks to 30 months of active weight loss with 47% (n = 23) less than 6 months in duration. It has been suggested that weight loss plateaus at approximately 6 months (12), suggesting that lifestyle interventions should be conducted over a 6-month period to ensure maximum weight loss is achieved; however, any longer than this may not be necessary. One study included in this review reported data at 6 monthly time points up to 30 months and some sex-race sub-groups continued to lose weight up to 18 months, suggesting longer interventions may be of benefit for some populations. Weight loss did plateau around 6–12 months in other sex-race sub-groups, but these groups also started to regain weight, highlighting the importance of weight maintenance programmes (84). It remains unclear whether men lose weight at a faster rate than women (after adjusting for initial body weight); therefore, 6 months may be sufficient for maximal weight loss in men but not women. Research does suggest that women are better at maintaining weight loss (12), possibly due to a more gradual initial weight decrease than men. It has been reported that differences in weight loss between men and women early on in an intervention do not exist at completion of the study (92). These patterns of weight loss in men and women may be of importance for determining the most suitable weight loss interventions and also for maintenance of lost weight.
Although 80% of the studies directly comparing weight loss (kg) between men and women found that men lost significantly more weight than women, it should be noted that women also lost weight during these interventions. Also, two of the studies (53,79) reported significant differences in weight loss (kg) between men and women, but when adjusted for baseline weight, this was no longer significant. Of the studies reporting weight loss as a percentage of baseline weight, only two reported a significant sex difference with men losing more percent weight over 16 weeks (61) and 30 months (84). Both analysis of effect sizes and meta-analyses of the differences in change in weight outcomes between men and women showed greater differences for men when using absolute weight change. However, when percent weight change or change in BMI was used, results indicating greater weight loss in men were less convincing, but not absent. This is likely because percentage weight change accounts for the baseline differences that exist in weight and height, which absolute weight change does not. Therefore, reporting only absolute weight loss rather than weight change as a percentage of baseline weight or BMI may lead to an incorrect conclusion regarding whether a meaningful sex difference exists. The capacity to directly compare results between absolute weight change, percent weight change and BMI change was also limited because all outcomes were not reported in all studies, thus different studies were included in the analysis of effect sizes and meta-analyses of each weight outcome. Additionally, the number of studies reporting these outcomes, particularly percent weight change and BMI, was relatively small. Therefore, whether differences in weight loss between men and women are due to differences in absolute size remains unclear; future reporting of percent weight loss or change in BMI will allow this to be explored more thoroughly.
There were many more diet or diet plus exercise interventions than exercise alone or dietary supplement interventions. It has previously been reported that the effectiveness of interventions producing a clinically significant weight loss were improved by the inclusion of both diet and PA (93). Over 85% of the interventions in this review consisted of diet alone or diet plus exercise interventions. Energy restriction through diet is often more effective for weight loss than exercise alone (94) and this was observed in the differences in mean weight loss between diet vs. exercise interventions in both sexes. However, with energy restriction difficult to maintain, the inclusion of exercise for increased energy expenditure means less energy restriction from foods and possibly greater adherence. This might explain why those who include both diet and exercise are more likely to maintain weight loss after 1 year (94). Hence, we could recommend that both men and women adopt a lifestyle of moderate energy restriction with the inclusion of exercise for weight loss.
Within those studies prescribing diet or diet plus exercise interventions, there were some common features that likely contributed to weight loss success in both sexes. Energy intake was tailored by sex, in that women were prescribed 1,200 kcal d−1 and men 1,500–1,800 kcal d−1. This is important due to the baseline differences in energy expenditure between men and women (6,7). Exercise recommendations were not extreme with protocols generally ranging from 30 to 60 min of exercise on 3–5 d week−1 with a number of studies increasing frequency and intensity over time. This is in line with exercise recommendations for overweight individuals with initial durations of 20–30 min d−1 working up to 60 min d−1 recommended and initial intensities of 50–60% working up to 60–80% of heart rate reserve recommended (95). This ensures that participants are able to complete exercise prescriptions safely but also ensures protocols change enough to ensure the benefits of exercise continue with increasing fitness. A large RCT investigating the effectiveness of an intensive lifestyle intervention in over 5,000 participants with type 2 diabetes examined weight losses over a 4-year period (92). This study was not included in the review because a considerable number of participants were currently using insulin, which is known to impact on weight. Nonetheless, it is interesting to note that participants with better dietary and PA practices were more likely to maintain their 1-year weight losses at 4 years further highlighting the importance of diet and PA, not only for weight loss but also weight maintenance.
A number of limitations were identified in this review, with the main ones being the availability of so few studies reporting weight loss as a percentage of baseline weight and the lack of direct comparison of men and women in the statistical analysis. There was also a high rate of heterogeneity between study interventions, making conclusions difficult. Additionally, although a large number of studies were retrieved and included, the search strategy did not include grey literature or unpublished work. However, this review did have a number of strengths including this being the first known systematic review on sex differences in weight loss. This review included a substantive number of studies and also adhered to PRISMA guidelines when conducting and reporting this review. There are a number of factors that need to be addressed in future research. Studies need to be powered to assess differences in weight loss between men and women, and outcomes need to be reported as a percentage of baseline weight or change in BMI rather than absolute weight loss only.
Men do appear to lose more weight than women during weight loss attempts, although it is possible that this is due to the greater baseline weight of men rather than the specific lifestyle interventions. Despite men showing greater weight loss than women in the majority of studies, women have still had significant weight losses meaning lifestyle interventions which include dietary and exercise prescription appear effective for both men and women. There is little evidence that men and women should adopt different weight loss strategies and the differences in weight loss seen in the short term may have little significance long term. To facilitate weight loss in overweight and obese men and women, health professionals need to focus on the inclusion of both diet and exercise in weight loss attempts and need to provide support for individuals to assist with implementation of programmes which has the potential to increase long-term success.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Authors' contributions
RLW has made substantial contributions to conception and design, data collection and analysis, interpretation of data and has been involved in drafting the manuscript. RC has made substantial contributions to conception and design, interpretation of data and revising it critically for important intellectual content. CEC has made substantial contributions to interpretation of data and revising it critically for important intellectual content. LW has made substantial contributions to interpretation of data and revising it critically for important intellectual content. RLW, RC, CEC and LW have given final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors would like to acknowledge Debbie Booth for her assistance with undertaking the literature search.
APPENDIX
Appendix 1
Supporting Information
Additioal Supporting Information may be found in the online version of this article, http://dx.doi.org/10.1111/obr.12241
(a) Meta-analysis comparing absolute weight change in men and women. (b) Meta-analysis comparing percent weight change in men and women. (c) Meta-analysis comparing change in body mass index (BMI) in men and women.
Table S1.Study characteristics.
Table S2.Critical appraisal of RCTs included in review.
Table S3.Weight outcomes and results.
Description of effective* interventions for weight loss in men and/or women.
References
- 1.World Health Organization. Obesity and Overweight. Geneva: WHO; 2013. URL: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed August 2014) [Google Scholar]
- 2.Organisation for Economic Co-operation and Development. OECD Obesity Update 2012. France: OECD; 2012. [Google Scholar]
- 3.Australian Bureau of Statistics. Overweight and Obesity in Adults in Australia: A Snapshot. Canberra: Australian Bureau of Statistics; 2011. [Google Scholar]
- 4.National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults. Melbourne: NHMRC; 2013. pp. 1–202. [Google Scholar]
- 5.Boutcher S, Dunn S. Factors that may impede the weight loss response to exercise-based interventions. Obes Rev. 2009;10:671–680. doi: 10.1111/j.1467-789X.2009.00621.x. [DOI] [PubMed] [Google Scholar]
- 6.Wu B, O'Sullivan A. Sex differences in energy metabolism need to be considered with lifestyle modifications in humans. J Nutr Metab. 2011;2011 doi: 10.1155/2011/391809. doi: 10.1155/2011/391809; [Epub 2011 Jun 6] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cunningham JJ. Body composition as a determinant of energy expenditure: a synthetic review and a proposed general prediction equation. Am J Clin Nutr. 1991;54:963–969. doi: 10.1093/ajcn/54.6.963. [DOI] [PubMed] [Google Scholar]
- 8.Donnelly JE, Hill JO, Jacobsen DJ, et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Arch Intern Med. 2003;163:1343–1350. doi: 10.1001/archinte.163.11.1343. [DOI] [PubMed] [Google Scholar]
- 9.Couillard C, Mauriege P, Prud'Homme D, et al. Plasma leptin concentrations: gender differences and associations with metabolic risk factors for cardiovascular disease. Diabetologia. 1997;40:1178–1184. doi: 10.1007/s001250050804. [DOI] [PubMed] [Google Scholar]
- 10.Curioni C, Lourenco P. Long-term weight loss after diet and exercise: a systematic review. Int J Obes (Lond) 2005;29:1168–1174. doi: 10.1038/sj.ijo.0803015. [DOI] [PubMed] [Google Scholar]
- 11.Douketis J, Macie C, Thabane L, Williamson D. Systematic review of long-term weight loss studies in obese adults: clinical significance and applicability to clinical practice. Int J Obes (Lond) 2005;29:1153–1167. doi: 10.1038/sj.ijo.0802982. [DOI] [PubMed] [Google Scholar]
- 12.Franz MJ, VanWormer JJ, Crain AL, et al. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc. 2007;107:1755–1767. doi: 10.1016/j.jada.2007.07.017. [DOI] [PubMed] [Google Scholar]
- 13.Hutchesson MJ, Hulst J, Collins CE. Weight management interventions targeting young women: a systematic review. J Acad Nutr Diet. 2013;113:795–802. doi: 10.1016/j.jand.2013.01.015. [DOI] [PubMed] [Google Scholar]
- 14.Young M, Morgan P, Plotnikoff R, Callister R, Collins C. Effectiveness of male-only weight loss and weight loss maintenance interventions: a systematic review with meta-analysis. Obes Rev. 2012;13:393–408. doi: 10.1111/j.1467-789X.2011.00967.x. [DOI] [PubMed] [Google Scholar]
- 15.de Castro JJ, Dias T, Chambel P, et al. A randomized double-blind study comparing the efficacy and safety of orlistat versus placebo in obese patients with mild to moderate hypercholesterolemia. Rev Port Cardiol. 2009;28:1361–1374. [PubMed] [Google Scholar]
- 16.Derosa G, Mugellini A, Ciccarelli L, Rinaldi A, Fogari R. Effects of orlistat, simvastatin, and orlistat + simvastatin in obese patients with hypercholesterolemia: a randomized, open-label trial. Curr Ther Res Clin Exp. 2002;63:621–633. [Google Scholar]
- 17.Adams TD, Davidson LE, Litwin SE, et al. Health benefits of gastric bypass surgery after 6 years. JAMA. 2012;308:1122–1131. doi: 10.1001/2012.jama.11164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Korenkov M, Kneist W, Heintz A, Junginger T. Laparoscopic gastric banding as a universal method for the treatment of patients with morbid obesity. Obes Surg. 2004;14:1123–1127. doi: 10.1381/0960892041975479. [DOI] [PubMed] [Google Scholar]
- 19.Padwal RS, Majumdar SR. Drug treatments for obesity: orlistat, sibutramine, and rimonabant. Lancet. 2007;369:71–77. doi: 10.1016/S0140-6736(07)60033-6. [DOI] [PubMed] [Google Scholar]
- 20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.American Dietetic Association. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. American Dietetic Association; 2012. URL: http://www.adaevidencelibrary.com/files/Docs/2012_Jan_EA_Manual.pdf (accessed April 2013) [Google Scholar]
- 22.Cochrane Collaboration. Obtaining standard deviations from standard errors and confidence intervals for group means. In: Higgins J, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011] 2011. In: (eds).. URL: http://www.cochrane-handbook.org (accessed April 2014) [Google Scholar]
- 23.Ellis P. The Essential Guide to Effect Sizes – Statistical Power, Meta-Analysis, and the Interpretation of Research Results. New York: Cambridge University Press; 2010. [Google Scholar]
- 24.Cohen J. Statistical Power Analysis for the Behavioral Sciences. Oxford: Routledge Academic; 2013. [Google Scholar]
- 25.Review Manager (RevMan) [Computer program] 2011. Version 5.1. The Nordic Cochrane Centre. The Cochrane Collaboration: Copenhagen,
- 26.Strain GW, Strain JJ, Zumoff B. L-tryptophan does not increase weight loss in carbohydrate-craving obese subjects. Int J Obes (Lond) 1985;9:375–380. [PubMed] [Google Scholar]
- 27.Kanders BS, Lavin PT, Kowalchuk MB, Greenberg I, Blackburn GL. An evaluation of the effect of aspartame on weight loss. Appetite. 1988;11(Suppl. 1):73–84. [PubMed] [Google Scholar]
- 28.Cameron R, MacDonald MA, Schlegel RP, et al. Toward the development of self-help health behaviour change programs: weight loss by correspondence. Can J Public Health. 1990;81:275–279. [PubMed] [Google Scholar]
- 29.Wood PD, Stefanick ML, Williams PT, Haskell WL. The effects on plasma lipoproteins of a prudent weight-reducing diet, with or without exercise, in overweight men and women. N Engl J Med. 1991;325:461–466. doi: 10.1056/NEJM199108153250703. [DOI] [PubMed] [Google Scholar]
- 30.Folsom AR, Qamhieh HT, Wing RR, et al. Impact of weight loss on plasminogen activator inhibitor (PAI-1), factor VII, and other hemostatic factors in moderately overweight adults. Arterioscler Thromb. 1993;13:162–169. doi: 10.1161/01.atv.13.2.162. [DOI] [PubMed] [Google Scholar]
- 31.Hakala P, Karvetti RL, Ronnemaa T. Group vs. individual weight reduction programmes in the treatment of severe obesity – a five year follow-up study. Int J Obes Relat Metab Disord. 1993;17:97–102. [PubMed] [Google Scholar]
- 32.Morris DH, Cuneo P, Stuart MJ, et al. High-intensity sweetener, energy and nutrient intakes of overweight women and men participating in a weight-loss program. Nutr Res. 1993;13:123–132. [Google Scholar]
- 33.Schlundt DG, Hill JO, Popecordle J, Arnold D, Virts KL, Katahn M. Randomized evaluation of a low-fat ad libitum carbohydrate-diet for weight-reduction. Int J Obes (Lond) 1993;17:623–629. [PubMed] [Google Scholar]
- 34.Stevens VJ, Corrigan SA, Obarzanek E, et al. Weight loss intervention in phase 1 of the trials of hypertension prevention. The TOHP Collaborative Research Group. Arch Intern Med. 1993;153:849–858. [PubMed] [Google Scholar]
- 35.Wing RR, Blair E, Marcus M, Epstein LH, Harvey J. Year-long weight loss treatment for obese patients with type II diabetes: does including an intermittent very-low-calorie diet improve outcome? Am J Med. 1994;97:354–362. doi: 10.1016/0002-9343(94)90302-6. [DOI] [PubMed] [Google Scholar]
- 36.Wing RR, Jeffery RW. Effect of modest weight loss on changes in cardiovascular risk factors: are there differences between men and women or between weight loss and maintenance? Int J Obes Relat Metab Disord. 1995;19:67–73. [PubMed] [Google Scholar]
- 37.Agurs-Collins TD, Kumanyika SK, Ten Have TR, Adams-Campbell LL. A randomized controlled trial of weight reduction and exercise for diabetes management in older African-American subjects. Diabetes Care. 1997;20:1503–1511. doi: 10.2337/diacare.20.10.1503. [DOI] [PubMed] [Google Scholar]
- 38.Torgerson JS, Lissner L, Lindroos AK, Kruijer H, Sjostrom L. VLCD plus dietary and behavioural support versus support alone in the treatment of severe obesity. A randomised two-year clinical trial. Int J Obes Relat Metab Disord. 1997;21:987–994. doi: 10.1038/sj.ijo.0800507. [DOI] [PubMed] [Google Scholar]
- 39.Williams KV, Mullen ML, Kelley DE, Wing RR. The effect of short periods of caloric restriction on weight loss and glycemic control in type 2 diabetes. Diabetes Care. 1998;21:2–8. doi: 10.2337/diacare.21.1.2. [DOI] [PubMed] [Google Scholar]
- 40.Ditschuneit HH, Flechtner-Mors M, Johnson TD, Adler G. Metabolic and weight-loss effects of a long-term dietary intervention in obese patients. Am J Clin Nutr. 1999;69:198–204. doi: 10.1093/ajcn/69.2.198. [DOI] [PubMed] [Google Scholar]
- 41.Fontaine KR, Barofsky I, Andersen RE, et al. Impact of weight loss on health-related quality of life. Qual Life Res. 1999;8:275–277. doi: 10.1023/a:1008835602894. [DOI] [PubMed] [Google Scholar]
- 42.Janssen I, Ross R. Effects of sex on the change in visceral, subcutaneous adipose tissue and skeletal muscle in response to weight loss. Int J Obes Relat Metab Disord. 1999;23:1035–1046. doi: 10.1038/sj.ijo.0801038. [DOI] [PubMed] [Google Scholar]
- 43.Jeffery RW, Bjornson-Benson WM, Rosenthal BS, Kurth CL, Dunn MM. Effectiveness of monetary contracts with two repayment schedules on weight reduction in men and women from self-referred and population samples. Behav Ther. 1984;15:273–279. [Google Scholar]
- 44.Donnelly JE, Honas JJ, Smith BK, et al. Aerobic exercise alone results in clinically significant weight loss for men and women: Midwest exercise trial 2. Obesity (Silver Spring) 2013;21:E219–E228. doi: 10.1002/oby.20145. [Randomized Controlled Trial Research Support, N.I.H., Extramural] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gorin AA, Raynor HA, Fava J, et al. Randomized controlled trial of a comprehensive home environment-focused weight-loss program for adults. Health Psychol. 2013;32:128–137. doi: 10.1037/a0026959. [Randomized Controlled Trial Research Support, N.I.H., Extramural] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lopez-Legarrea P, De La Iglesia R, Abete I, et al. Short-term role of the dietary total antioxidant capacity in two hypocaloric regimes on obese with metabolic syndrome symptoms: the RESMENA randomized controlled trial. Nutr Metab (Lond) 2013;10:22. doi: 10.1186/1743-7075-10-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Munro IA, Garg ML. Prior supplementation with long chain omega-3 polyunsaturated fatty acids promotes weight loss in obese adults: a double-blinded randomised controlled trial. Food Funct. 2013;4:650–658. doi: 10.1039/c3fo60038f. [Randomized Controlled Trial] [DOI] [PubMed] [Google Scholar]
- 48.Sanal E, Ardic F, Kirac S. Effects of aerobic or combined aerobic resistance exercise on body composition in overweight and obese adults: gender differences. A randomized intervention study. Eur J Phys Rehabil Med. 2013;49:1–11. [Comparative Study Randomized Controlled Trial Research Support, Non-U.S. Gov't] [PubMed] [Google Scholar]
- 49.Shrestha M, Combest T, Fonda SJ, Alfonso A, Guerrero A. Effect of an accelerometer on body weight and fitness in overweight and obese active duty soldiers. Mil Med. 2013;178:82–87. doi: 10.7205/milmed-d-12-00275. [Randomized Controlled Trial Research Support, U.S. Gov't, Non-P.H.S.] [DOI] [PubMed] [Google Scholar]
- 50.Andersen RE, Franckowiak SC, Bartlett SJ, Fontaine KR. Physiologic changes after diet combined with structured aerobic exercise or lifestyle activity. Metabolism. 2002;51:1528–1533. doi: 10.1053/meta.2002.36304. [DOI] [PubMed] [Google Scholar]
- 51.Fraser GE, Bennett HW, Jaceldo KB, Sabate J. Effect on body weight of a free 76 kilojoule (320 calorie) daily supplement of almonds for six months. J Am Coll Nutr. 2002;21:275–283. doi: 10.1080/07315724.2002.10719221. [DOI] [PubMed] [Google Scholar]
- 52.Donnelly JE, Hill JO, Jacobsen DJ, et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Arch Intern Med. 2003;163:1343–1350. doi: 10.1001/archinte.163.11.1343. [DOI] [PubMed] [Google Scholar]
- 53.Farnsworth E, Luscombe ND, Noakes M, Wittert G, Argyiou E, Clifton PM. Effect of a high-protein, energy-restricted diet on body composition, glycemic control, and lipid concentrations in overweight and obese hyperinsulinemic men and women. Am J Clin Nutr. 2003;78:31–39. doi: 10.1093/ajcn/78.1.31. [DOI] [PubMed] [Google Scholar]
- 54.Jeffery RW, Sherwood NE, Brelje K, et al. Mail and phone interventions for weight loss in a managed-care setting: weigh-to-be one-year outcomes. Int J Obes Relat Metab Disord. 2003;27:1584–1592. doi: 10.1038/sj.ijo.0802473. [DOI] [PubMed] [Google Scholar]
- 55.Lafortuna CL, Resnik M, Galvani C, Sartorio A. Effects of non-specific vs. individualized exercise training protocols on aerobic, anaerobic and strength performance in severely obese subjects during a short-term body mass reduction program. J Endocrinol Invest. 2003;26:197–205. doi: 10.1007/BF03345157. [DOI] [PubMed] [Google Scholar]
- 56.Luscombe ND, Clifton PM, Noakes M, Farnsworth E, Wittert G. Effect of a high-protein, energy-restricted diet on weight loss and energy expenditure after weight stabilization in hyperinsulinemic subjects. Int J Obes (Lond) 2003;27:582–590. doi: 10.1038/sj.ijo.0802270. [DOI] [PubMed] [Google Scholar]
- 57.Volek JS, Sharman MJ, Gomez AL, et al. Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutr Metab (Lond) 2004;1:13. doi: 10.1186/1743-7075-1-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Bowen J, Noakes M, Clifton PM. Effect of calcium and dairy foods in high protein, energy-restricted diets on weight loss and metabolic parameters in overweight adults. Int J Obes (Lond) 2005;29:957–965. doi: 10.1038/sj.ijo.0802895. [DOI] [PubMed] [Google Scholar]
- 59.Burke V, Beilin LJ, Cutt HE, Mansour J, Wilson A, Mori TA. Effects of a lifestyle programme on ambulatory blood pressure and drug dosage in treated hypertensive patients: a randomized controlled trial. J Hypertens. 2005;23:1241–1249. doi: 10.1097/01.hjh.0000170388.61579.4f. [DOI] [PubMed] [Google Scholar]
- 60.Dansinger ML, Gleason JA, Griffith JL, Selker HP, Schaefer EJ. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: a randomized trial. JAMA. 2005;293:43–53. doi: 10.1001/jama.293.1.43. [DOI] [PubMed] [Google Scholar]
- 61.Luscombe-Marsh ND, Noakes M, Wittert GA, Keogh JB, Foster P, Clifton PM. Carbohydrate-restricted diets high in either monounsaturated fat or protein are equally effective at promoting fat loss and improving blood lipids. Am J Clin Nutr. 2005;81:762–772. doi: 10.1093/ajcn/81.4.762. [DOI] [PubMed] [Google Scholar]
- 62.Stewart KJ, Bacher AC, Hees PS, Tayback M, Ouyang P, De Beur SJ. Exercise effects on bone mineral density: relationships to changes in fitness and fatness. Am J Prev Med. 2005;28:453–460. doi: 10.1016/j.amepre.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 63.Byrne NM, Meerkin JD, Laukkanen R, Ross R, Fogelholm M, Hills AP. Weight loss strategies for obese adults: personalized weight management program vs. standard care. Obesity (Silver Spring) 2006;14:1777–1788. doi: 10.1038/oby.2006.205. [DOI] [PubMed] [Google Scholar]
- 64.Gaullier J-M, Halse J, Hoivik HO, et al. Six months supplementation with conjugated linoleic acid induces regional-specific fat mass decreases in overweight and obese. Br J Nutr. 2007;97:550–560. doi: 10.1017/S0007114507381324. [DOI] [PubMed] [Google Scholar]
- 65.Tate DF, Jeffery RW, Sherwood NE, Wing RR. Long-term weight losses associated with prescription of higher physical activity goals. Are higher levels of physical activity protective against weight regain? Am J Clin Nutr. 2007;85:954–959. doi: 10.1093/ajcn/85.4.954. [DOI] [PubMed] [Google Scholar]
- 66.Thorsdottir I, Tomasson H, Gunnarsdottir I, et al. Randomized trial of weight-loss-diets for young adults varying in fish and fish oil content. Int J Obes (Lond) 2007;31:1560–1566. doi: 10.1038/sj.ijo.0803643. [DOI] [PubMed] [Google Scholar]
- 67.Major GC, Doucet E, Jacqmain M, St-Onge M, Bouchard C, Tremblay A. Multivitamin and dietary supplements, body weight and appetite: results from a cross-sectional and a randomised double-blind placebo-controlled study. Br J Nutr. 2008;99:1157–1167. doi: 10.1017/S0007114507853335. [DOI] [PubMed] [Google Scholar]
- 68.Shai I, Schwarzfuchs D, Henkin Y, et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. [Erratum appears in N Engl J Med. 2009 Dec 31;361(27):2681] N Engl J Med. 2008;359:229–241. doi: 10.1056/NEJMoa0708681. [DOI] [PubMed] [Google Scholar]
- 69.Di Pierro F, Menghi AB, Barreca A, Lucarelli M, Calandrelli A. Greenselect phytosome as an adjunct to a low-calorie diet for treatment of obesity: a clinical trial. Altern Med Rev. 2009;14:154–160. [PubMed] [Google Scholar]
- 70.Ramel A, Jonsdottir MT, Thorsdottir I. Consumption of cod and weight loss in young overweight and obese adults on an energy reduced diet for 8-weeks. Nutr Metab Cardiovasc Dis. 2009;19:690–696. doi: 10.1016/j.numecd.2008.12.013. [DOI] [PubMed] [Google Scholar]
- 71.ter Bogt NCW, Bemelmans WJE, Beltman FW, Broer J, Smit AJ, van der Meer K. Preventing weight gain: one-year results of a randomized lifestyle intervention. Am J Prev Med. 2009;37:270–277. doi: 10.1016/j.amepre.2009.06.011. [DOI] [PubMed] [Google Scholar]
- 72.Dennis EA, Dengo AL, Comber DL, et al. Water consumption increases weight loss during a hypocaloric diet intervention in middle-aged and older adults. Obesity (Silver Spring) 2010;18:300–307. doi: 10.1038/oby.2009.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Straznicky NE, Lambert EA, Nestel PJ, et al. Sympathetic neural adaptation to hypocaloric diet with or without exercise training in obese metabolic syndrome subjects. Diabetes. 2010;59:71–79. doi: 10.2337/db09-0934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Wu X, Xu X, Shen J, Perricone NV, Preuss HG. Enhanced weight loss from a dietary supplement containing standardized Phaseolus vulgaris extract in overweight men and women. J Appl Res. 2010;10:73–79. [Google Scholar]
- 75.Gabriele JM, Carpenter BD, Tate DF, Fisher EB. Directive and nondirective e-coach support for weight loss in overweight adults. Ann Behav Med. 2011;41:252–263. doi: 10.1007/s12160-010-9240-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Shea MK, Nicklas BJ, Houston DK, et al. The effect of intentional weight loss on all-cause mortality in older adults: results of a randomized controlled weight-loss trial. Am J Clin Nutr. 2011;94:839–846. doi: 10.3945/ajcn.110.006379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Chen S-C, Lin Y-H, Huang H-P, Hsu W-L, Houng J-Y, Huang C-K. Effect of conjugated linoleic acid supplementation on weight loss and body fat composition in a Chinese population. Nutrition. 2012;28:559–565. doi: 10.1016/j.nut.2011.09.008. [DOI] [PubMed] [Google Scholar]
- 78.Dow CA, Going SB, Chow H-HS, Patil BS, Thomson CA. The effects of daily consumption of grapefruit on body weight, lipids, and blood pressure in healthy, overweight adults. Metabolism. 2012;61:1026–1035. doi: 10.1016/j.metabol.2011.12.004. [DOI] [PubMed] [Google Scholar]
- 79.Evans EM, Mojtahedi MC, Thorpe MP, Valentine RJ, Kris-Etherton PM, Layman DK. Effects of protein intake and gender on body composition changes: a randomized clinical weight loss trial. Nutr Metab. 2012;9:55. doi: 10.1186/1743-7075-9-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Hersey JC, Khavjou O, Strange LB, et al. The efficacy and cost-effectiveness of a community weight management intervention: a randomized controlled trial of the health weight management demonstration. Prev Med. 2012;54:42–49. doi: 10.1016/j.ypmed.2011.09.018. [DOI] [PubMed] [Google Scholar]
- 81.Nakade M, Aiba N, Suda N, et al. Behavioral change during weight loss program and one-year follow-up: Saku Control Obesity Program (SCOP) in Japan. Asia Pac J Clin Nutr. 2012;21:22–34. [PubMed] [Google Scholar]
- 82.Stocks T, Angquist L, Banasik K, et al. TFAP2B influences the effect of dietary fat on weight loss under energy restriction. PLoS ONE. 2012;7:e43212. doi: 10.1371/journal.pone.0043212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.St-Onge M-P, Salinardi T, Herron-Rubin K, Black RM. A weight-loss diet including coffee-derived mannooligosaccharides enhances adipose tissue loss in overweight men but not women. Obesity (Silver Spring) 2012;20:343–348. doi: 10.1038/oby.2011.289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.West DS, Elaine Prewitt T, Bursac Z, Felix HC. Weight loss of black, white, and Hispanic men and women in the Diabetes Prevention Program. (Erratum appears in Obesity [Silver Spring]. 2009 Nov;17(11):2119–2120) Obesity (Silver Spring) 2008;16:1413–1420. doi: 10.1038/oby.2008.224. [DOI] [PubMed] [Google Scholar]
- 85.Christiansen T, Paulsen SK, Bruun JM, et al. Comparable reduction of the visceral adipose tissue depot after a diet-induced weight loss with or without aerobic exercise in obese subjects: a 12-week randomized intervention study. Eur J Endocrinol. 2009;160:759–767. doi: 10.1530/EJE-08-1009. [DOI] [PubMed] [Google Scholar]
- 86.De Jonge L, Bray GA, Smith SR, et al. Effect of diet composition and weight loss on resting energy expenditure in the POUNDS LOST study. Obesity (Silver Spring) 2012;20:2384–2389. doi: 10.1038/oby.2012.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Linde JA, Jeffery RW, Levy RL, Pronk NP, Boyle RG. Weight loss goals and treatment outcomes among overweight men and women enrolled in a weight loss trial. Int J Obes (Lond) 2005;29:1002–1005. doi: 10.1038/sj.ijo.0802990. [DOI] [PubMed] [Google Scholar]
- 88.Moran LJ, Luscombe-Marsh ND, Noakes M, Wittert GA, Keogh JB, Clifton PM. The satiating effect of dietary protein is unrelated to postprandial ghrelin secretion. J Clin Endocrinol Metab. 2005;90:5205–5211. doi: 10.1210/jc.2005-0701. [DOI] [PubMed] [Google Scholar]
- 89.Altman DG. Better reporting of randomised controlled trials: the CONSORT statement. BMJ. 1996;313:570. doi: 10.1136/bmj.313.7057.570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Frost MH, Reeve BB, Liepa AM, Stauffer JW, Hays RD. What is sufficient evidence for the reliability and validity of patient-reported outcome measures? Value Health. 2007;10:S94–S105. doi: 10.1111/j.1524-4733.2007.00272.x. [DOI] [PubMed] [Google Scholar]
- 91.Pagoto SL, Schneider KL, Oleski JL, Luciani JM, Bodenlos JS, Whited MC. Male inclusion in randomized controlled trials of lifestyle weight loss interventions. Obesity (Silver Spring) 2012;20:1234–1239. doi: 10.1038/oby.2011.140. [DOI] [PubMed] [Google Scholar]
- 92.Wadden TA, Neiberg RH, Wing RR, et al. Four-year weight losses in the Look AHEAD study: factors associated with long-term success. Obesity (Silver Spring) 2011;19:1987–1998. doi: 10.1038/oby.2011.230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Greaves CJ, Sheppard KE, Abraham C, et al. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health. 2011;11:119. doi: 10.1186/1471-2458-11-119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Miller WC, Koceja DM, Hamilton EJ. A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Int J Obes Relat Metab Disord. 1997;21:941–947. doi: 10.1038/sj.ijo.0800499. [Comparative Study Journal Article Meta-Analysis Research Support, Non-U.S. Gov't] [DOI] [PubMed] [Google Scholar]
- 95.Ehrman J, Gordon P, Visich P, Keteyian S. Clinical Exercise Physiology. 3rd Edn. Champaign, IL: Human Kinetics; 2013. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(a) Meta-analysis comparing absolute weight change in men and women. (b) Meta-analysis comparing percent weight change in men and women. (c) Meta-analysis comparing change in body mass index (BMI) in men and women.
Table S1.Study characteristics.
Table S2.Critical appraisal of RCTs included in review.
Table S3.Weight outcomes and results.
Description of effective* interventions for weight loss in men and/or women.