

Abstract
We report the case of a 66-year-old woman with no significant past medical history who presented to the Emergency Department at Houston Methodist Hospital with 24 hours of chest pain. An electrocardiogram was done, an electrocardiogram confirmed a posterolateral ST elevation myocardial infarction. An immediate and successful percutaneous coronary intervention of a totally occluded ramus intermedius was performed. Six hours later she developed pulmonary edema, cardiogenic shock, severe acidosis, and anuria. Echocardiography showed severe mitral regurgitation due to a ruptured anterolateral papillary muscle, and emergency surgery revealed necrosis of this muscle. A bioprosthetic mitral valve was placed, and extracorporeal membrane oxygenation was needed for 3 days. This is a rare mechanical complication of myocardial infarction, which usually affects the posteromedial papillary muscle. The patient subsequently made a good recovery. One month later, just prior to discharge home, the patient developed pneumonia and sepsis, and she expired from multiorgan failure.
Keywords: cardiac anatomy/pathologic anatomy, cardiac function, physiology, heart valve prosthesis, mitral regurgitation, myocardial infarction

W. K. Abu Saleh, M.D.
Introduction
There are three catastrophic mechanical complications of acute myocardial infarction. These include left ventricular free wall rupture, rupture of the interventricular septum, and papillary muscle rupture. All involve loss of structural integrity of the infarcted tissue and are associated with extraordinarily high mortality rates if not promptly recognized and treated. Fortunately, with an increasing emphasis on early revascularization coupled with improved techniques, these catastrophic complications are relatively rare, representing 2.3% of acute myocardial infarction.1
Papillary muscle rupture (PMR) frequently presents with symptoms ranging from acutely decompensated heart failure to cardiogenic shock. The most frequent scenario involves infarction upstream from the posterior descending artery (i.e., the right coronary artery in right-dominant systems or the left circumflex artery in left-dominant systems). Valvular competence during ventricular systole is maintained by the actions of two papillary muscles—anterolateral and posteromedial. The anterolateral muscle typically has a dual blood supply while the posteromedial muscle is supplied from only the posterior descending artery, making it more susceptible to infarction and rupture. Treatment often necessitates emergent surgical intervention with mitral valve repair (if muscle necrosis is limited) or valve replacement.2 Both immediate and long-term outcomes are improved with concomitant coronary revascularization.3
We illustrate a case that demonstrates the typical presentation of acute papillary muscle rupture and remind clinicians that prompt recognition and management are critical in this uncommon but lethal complication.
Case Report
We present the case of a 66-year-old female patient with no significant past medical history presenting with chest pain that was treated with antacids by her primary care physician. The next day she presented to the emergency room, where an electrocardiogram revealed posterolateral ST elevation myocardial infarction. The patient was immediately taken to the catheterization lab. A successful percutaneous intervention was performed on an acutely occluded large ramus intermedius vessel that was supplying a large portion of the lateral wall (Figure 1).
Figure 1.
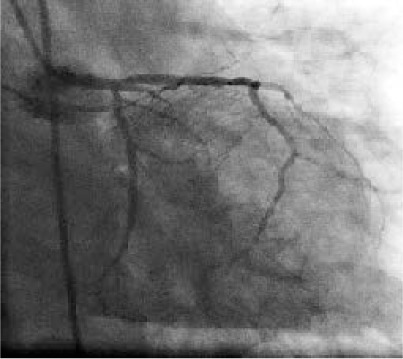
Angiogram showing a totally occluded ramus intermedius.
The patient did well initially, but several hours later she suddenly went into cardiogenic shock. An intra-aortic balloon pump was placed, and an echocardiogram demonstrated that she had severe mitral regurgitation from a ruptured papillary muscle (Figure 2).
Figure 2.
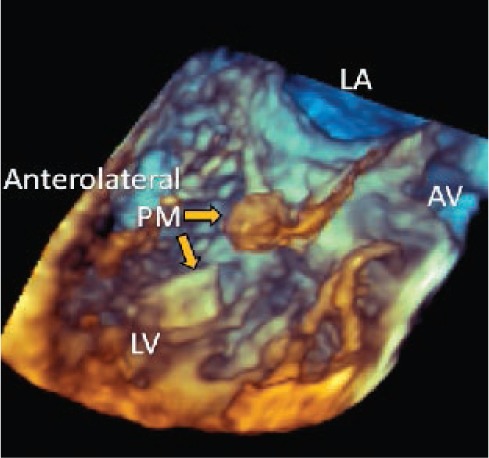
Echocardiogram showing a ruptured anterolateral papillary muscle with mitral regurgitation. LA: left atrium; LV: left ventricle; AV: aortic valve.
The patient, on maximal support, deteriorated rapidly with progressive acidosis, oliguria, and florid pulmonary edema. In spite of the very high risk, we decided to intervene surgically. Once in the operating room, transesophageal echocardiography confirmed severe mitral regurgitation with a ruptured anterolateral papillary muscle and a small left atrium. Shortly after the patient was put on cardiopulmonary bypass, the acidosis resolved and she began to make urine. Excellent visualization of the mitral valve was obtained using a vertical transseptal approach through the right atrium. The valve was carefully inspected and the necrotic ruptured anterolateral papillary muscle was seen (Figure 3). There was a large chunk of muscle attached to the A1 chordal apparatus. The anterior leaflet of the mitral valve was excised while keeping the posterior leaflet intact. A 27-mm St Jude Epic bioprosthesis was inserted (Figure 4).
Figure 3.
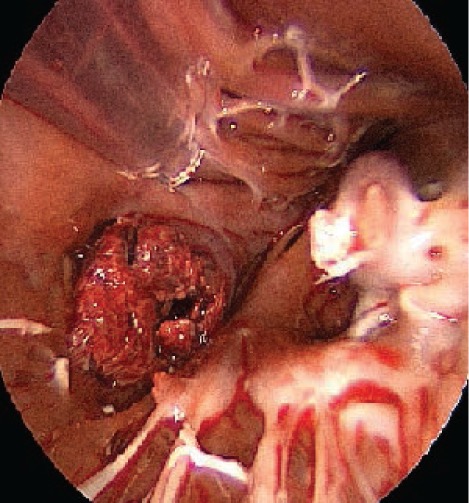
Image showing the ruptured anterolateral papillary muscle and muscle attached to the cord.
Figure 4.

Image showing the ruptured papillary muscle with the mitral valve after excision.
She was placed on extracorporeal membrane oxygenation that was successfully weaned 3 days later. Following this, she made a remarkable early recovery. One month later, just prior to discharge, she expired after developing pneumonia that progressed to sepsis with multiorgan failure.
Discussion
Papillary muscle rupture occurs most frequently within 2 to 7 days after a myocardial infarction.4 This patient presented at least 24 hours after the onset of chest pain. Rupture of the posteromedial papillary muscle occurs much more frequently than rupture of the anterolateral muscle. This is due to differences in blood supply, with the posteromedial muscle receiving blood only from the posterior descending artery while the anterolateral muscle receives a dual blood supply from both the left anterior descending and left circumflex arteries. Given the singular blood supply to the posteromedial muscle, about half the cases of rupture occur with relatively small infarcts.5
Transthoracic echocardiography (TTE) is often the first imaging modality used in diagnosing PMR, with a sensitivity of 65% to 85%.6 Since the mitral apparatus is a posterior structure, TTE can offer superior visibility with a diagnostic yield between 95% and 100%.7 Once PMR is identified, urgent surgery is warranted. Without surgical repair, approximately 90% of patients with PMR will die within 1 week.8 The valve may be repaired in selected cases. However, the tissue is often weak and friable, making repair difficult or impossible. Most cases are best served with mitral valve replacement.
Fortunately, with the increasing use of early and effective revascularization therapies, PMR has become a fairly rare complication. Clinicians should, however, remain aware and be able to diagnose this serious and potentially lethal complication, especially where thrombolytics are still used as a primary treatment for acute coronary syndromes or, as in this case, when the patient presents with prolonged symptoms.
Conclusion
Cardiogenic shock developing days after the onset of angina, an angina-equivalent, or diagnosed infarction may indicate a catastrophic mechanical complication of AMI, such as papillary muscle rupture. Although the incidence appears to be on the decline, clinicians must keep potentially lethal complications in mind when evaluating these unstable patients.
Acknowledgments
Conflict of Interest Disclosure: The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Funding/Support: The authors have nothing to disclose.
References
- 1.Yuan S, Jing H, Lavee J. The mechanical complications of acute myocardial infarction: echocardiographic visualizations. Turkish J Thorac Cardiovasc Surg. 2011 Oct;19(1):36–42. [Google Scholar]
- 2.David TE. Techniques and results of mitral valve repair for ischemic mitral regurgitation. J Card Surg. 1994 Mar;9(2 Suppl):274–7. doi: 10.1111/j.1540-8191.1994.tb00940.x. [DOI] [PubMed] [Google Scholar]
- 3.Kishon Y, Oh JK, Schaff HV, Mullany CJ, Tajik AJ, Gersh BJ. Mitral valve operation in postinfarction rupture of a papillary muscle: immediate results and long-term follow-up of 22 patients. Mayo Clin Proc. 1992 Nov;67(11):1023–30. doi: 10.1016/s0025-6196(12)61116-1. [DOI] [PubMed] [Google Scholar]
- 4.Lavie CJ, Gersh BJ. Mechanical and electrical complications of acute myocardial infarction. Mayo Clin Proc. 1990 May;65(5):709–30. doi: 10.1016/s0025-6196(12)65133-7. [DOI] [PubMed] [Google Scholar]
- 5.Antman EM, Morrow DA. ST-segment elevation myocardial infarction: management. In: Bonow RO, Man DL, Zipes DP, Libby P, editors. Braunwald's heart disease: a textbook of cardiovascular medicine. 9th ed. Philadelphia: Saunders Elsevier; 2011. Chapter 55. [Google Scholar]
- 6.Czarnecki A, Thakrar A, Fang T et al. Acute severe mitral regurgitation: consideration of papillary muscle architecture. Cardiovasc Ultrasound. 2008 Jan 18;6:5. doi: 10.1186/1476-7120-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sochowski RA, Chan KL, Ascah KJ, Bedard P. Comparison of accuracy of transesophageal versus transthoracic echocardiography for the detection of mitral valve prolapse with ruptured chordae tendineae (flail mitral leaflet) Am J Cardiol. 1991 Jun 1;67(15):1251–5. doi: 10.1016/0002-9149(91)90936-f. [DOI] [PubMed] [Google Scholar]
- 8.Nishimura RA, Gersh BJ, Schaff HV. The case for an aggressive surgical approach to papillary muscle rupture following myocardial infarction: “From paradise lost to paradise regained.”. Heart. 2000 Jun;83(6):611–13. doi: 10.1136/heart.83.6.611. [DOI] [PMC free article] [PubMed] [Google Scholar]