

Abstract
Objectives:
To test the reliability and validity of an Arabic version of the modified dental anxiety scale (MDAS), and to correlate it with other demographic data.
Methods:
The original English version of the MDAS was translated into Arabic, and then translated back into English by experienced bilingual professionals. Four hundred and seventy-four patients referred to dental clinics for treatment at the Faculty of Dentistry Hospital, Jeddah, Kingdom of Saudi Arabia from November 2012 to June 2013 participated in the study. The assessment tool included questions regarding demographic characteristics, frequency of dental visits, the Arabic version of the MDAS, and the patient's rating of their current level of anxiety using a visual analogue scale (VAS).
Results:
The Arabic version of the MDAS had excellent internal consistency and reliability (Alpha coefficients >0.90). The scale was unidimensional, and the percentage of patients with dental anxiety was 48.3% (using a cutoff total score of >15) and with dental phobia was 2.5% (using a cutoff total score of >16). Younger patients, females, and infrequent visitors to the dentist were more anxious than those who were older, male, and frequent visitors. Visual analogue scale scores correlated significantly with individual items on the MDAS questionnaire and total anxiety score, supporting the criterion validity.
Conclusion:
The Arabic version of the MDAS presented adequate internal consistency reliability, allowing its safe use to assess levels of dental anxiety in Arabic-speaking populations.
Anxiety related to dental treatment is a well-known phenomenon that has been reported to cause 6% of the general population to avoid dental treatments.1 This emotional state can also affect the dentist who may become anxious dealing with patients who are known to be difficult to manage and who delay or even cancel their dental appointments.2 Dental anxiety is defined as a patient's response to stress that is specific to dental situations.3 It is therefore, very important to rate patient anxiety for proper control and management. There is a wide range of psychometric self-assessment scales to assess anxiety in general that are commonly used for research and clinical purposes to assess the dental anxiety and fear. The Corah Dental Anxiety Scale (CDAS) is probably the most widely used scale.4
Three shortcomings of the CDAS have been noted: the item responses vary, the responses are not necessarily ordered from lowest to highest anxiety, and the scale does not include an item referring to dental injections.2 A Modified Dental Anxiety Scale (MDAS) was proposed to overcome the psychometric and content validity issues of the original CDAS.5 The MDAS is a 5-item multiple-choice questionnaire, which includes an item that rates respondent anxiety upon receiving local anesthetic injections; thereby, differing from the CDAS. Other small, but important changes were also made to the English version response scheme, creating a simple, quick, and easy-to-complete instrument that will not increase patients’ fear and anxiety.6,7
The original English-language version of the MDAS5 has been translated into different languages (which include, but are not limited to, Spanish, Greek, Chinese, Turkish, Romanian, and Tamil) and tested for readability and validity in adult populations in a variety of cross-cultural studies.8-13 It is desirable to establish a linguistic and cultural psychometric equivalent of the MDAS and other psychological scales translated from American or British scales. An Arabic version of the scale was used with Jordanian adolescents;14 the authors recommended that future researchers consider older age groups and differing countries where Arabic is spoken.
Spoken Arabic varies considerably across different cultures and countries, especially with regards to colloquial or slang usage. Therefore, it is important to develop an Arabic version of the MDAS, which is suitable for all Arabic-speaking individuals, using simple Arabic, which would be understood by individuals from different cultures or countries. Different cultures, which share Arabic, as a common language would still benefit from different Arabic versions of this scale, which will add further evidence for the reliability, and validity of the MDAS. Therefore, the aim of this study was to test the reliability and validity of an Arabic version of the MDAS. In addition, we evaluated whether the Arabic MDAS can be utilized as an effective tool to assess dental anxiety among Arabic-speaking Saudi adult dental patients, by correlating scale scores with other demographic data.
Methods
Research design and study sample
The present study was based on a cross-sectional design. It includes a convenience sample of adult patients who were referred to dental clinics for treatment at the Faculty of Dentistry Hospital, Jeddah, Saudi Arabia. Most patients attending this hospital are Saudis, with varying socio-economic backgrounds. Consent was obtained prior to participation in the study. Following a brief explanation by one of the authors, patients completed the questionnaire in the waiting area prior to their dental appointment. Five hundred patients participated in the study. Inclusion criteria were participants whose age was 18-70 years. Patients outside the selected age group were not included in the study (n=14). Out of the 500 questionnaires that were distributed to patients, 486 were returned and eligible to be included in the study. Twelve questionnaires were found to have one or more incomplete MDAS questions. All questionnaires with missing data were excluded. Thus, only 474 completed questionnaires were included in the study. Gender, age, and frequency of dental visits of the study respondents were also noted. Ethical approval and a waiver for informed consent were obtained from the Ethical Committee of the Faculty of Dentistry Hospital, King Abdulaziz University, Jeddah, Saudi Arabia. The study was conducted from November 2012 to June 2013, and was carried out according to the principles of the Helsinki Declaration.
Questionnaire
The MDAS is a 5-item multiple-choice questionnaire designed to measure the level of anxiety of respondents in reaction to 5 situations: (i) when planning to visit the dentist the following day, (ii) while in the waiting area for the appointment, (iii) having a tooth drilled, (iv) having scaling of the teeth, and (v) having a local anesthetic injection. Each item has 5 responses that range from one (not anxious) to 5 (extremely anxious). The total score is the sum of responses for the 5 items, and ranges from 5-25.
The original English version of the MDAS questionnaire was translated following the recommendations of Sartorius and Kuyken.15 An experienced bilingual professional who was fluent in English (and for whom Arabic was her native language) translated the questionnaire from English to Arabic. The resulting version was then translated back to English by another bilingual professional who was blind to the original English questionnaire, to reduce bias in translation.
The translated version was then corrected and culturally adapted with the help of the translators, to eliminate any difference in meaning between the original and back-translated version. The final version of the questionnaire was piloted/pretested with the target Arabic-speaking Saudi population. A convenience sample of 50 patients attending the dental outpatient clinic was selected to fill out the questionnaire. The patients were interviewed while they were completing the questionnaire, to evaluate the clarity of the contents. Final corrections were made to the translated Arabic version before testing of psychometric properties. To test concurrent criterion validity, patients were asked to rate their current level of anxiety or nervousness on a 100 mm Visual Analogue Scale (VAS), where zero referred to “not at all anxious” and 100 referred to “extreme dental anxiety.”
Statistical analysis
Data were analyzed using IBM Statistical Package for Social Sciences Version 20, (IBM, Armonk, NY, USA). A p-value <0.05 was used as the cutoff for statistical significance and all tests were 2-sided. The Shapiro-Wilk test was used to assess normality of anxiety scale scores. A known groups validity was tested by comparison of MDAS scores among groups using the Mann-Whitney test (for 2 groups) or the Kruskal-Wallis test (for 3 or more groups). In the case of a significant Kruskal-Wallis test, multiple comparisons among groups were performed using Dunn-Bonferroni tests. The receiver-operating characteristic (ROC) curve was used to select the best cutoff point for diagnosing dental anxiety and phobia versus the corresponding cutoff points for dental anxiety and phobia (>51% for a dental anxiety and >70% for high level of dental anxiety or phobia) that were used by Facco et al.16 Reliability was calculated using ordinal alpha reliability and an inter-item correlation matrix with Spearman's rho correlation coefficients.
Results
The present study included 474 dental patients; 46% were males with a mean age of 39.50±9.48 years. Less than 4% visited dentists regularly and 24.5% visited the dentist only when needed (Table 1). The current sample was similar in age and gender to the patients attending the Faculty of Dentistry Hospital, King Abdulaziz University (p>0.05). Moreover, our sample and the Saudi population were similar in terms of gender distribution (p>0.05), but not age distribution (p<0.05). In our sample, females were significantly younger than males (mean ages 37.08±7.41 and 42.34±10.78). Average scores for the 5 items of the MDAS (Table 2) indicated that the fifth item was the most influential on anxiety levels (3.25±0.87) and the second item was the least influential (2.32±0.79). Ratings on the VAS showed moderate anxiety (55.74±17.46). Testing the validity of the MDAS versus the VAS by ROC curve (Figures 1 & 2) revealed a considerable and significant area under the curve (AUC) both for dental anxiety (AUC=0.871, 95% confidence interval [CI]: 0.837-0.904) and dental phobia (AUC=0.852, 95% CI: 0.820-0.885). The best cutoff for dental anxiety on the MDAS scale as indicated by the ROC curve was >15, with sensitivity and specificity of 0.796. In contrast, the best cutoff for dental phobia was >16 (with sensitivity of 0.953 and specificity of 0.691).
Table 1.
Description of the study sample among the studied patients.
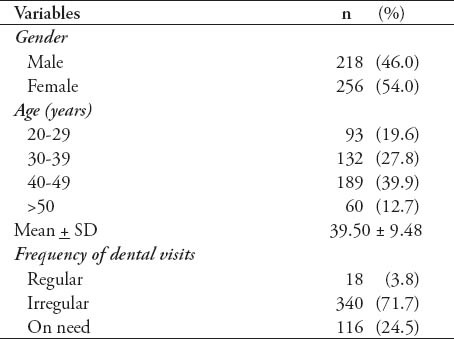
Table 2.
Descriptive statistics and inter-item correlation of the MDAS and VAS.
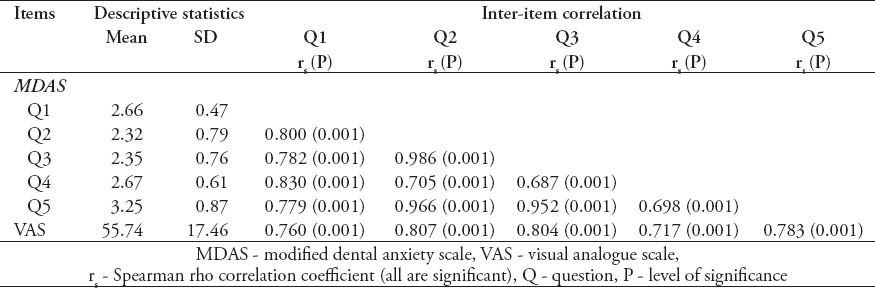
Figure 1.
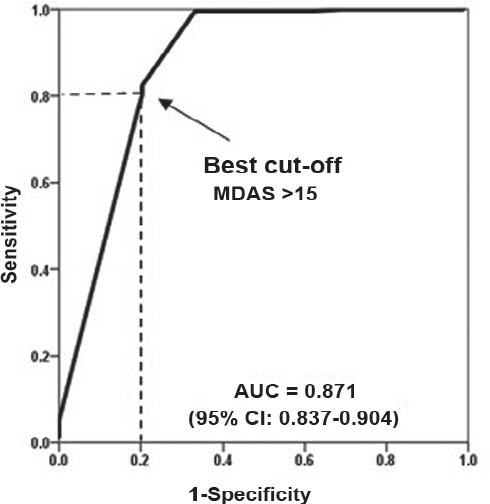
Receiver operating characteristic curve for modified dental anxiety scale (MDAS) versus visual analogue scale (VAS), where a VAS <51% was selected as an indicator of dental anxiety. AUC - area under the curve
Figure 2.
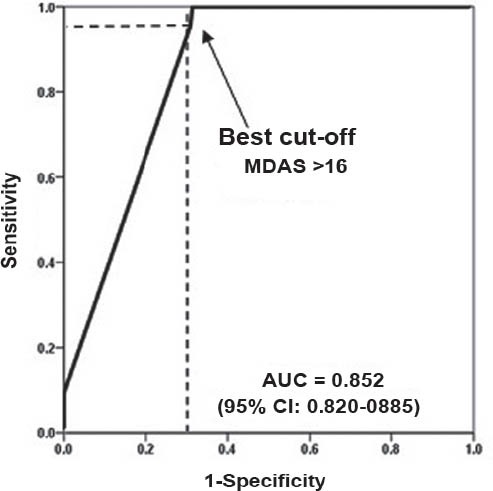
Receiver operating characteristic curve for modified dental anxiety scale (MDAS) versus visual analogue scale (VAS), where a VAS >70% was selected as an indicator of dental phobia. AUC - area under the curve
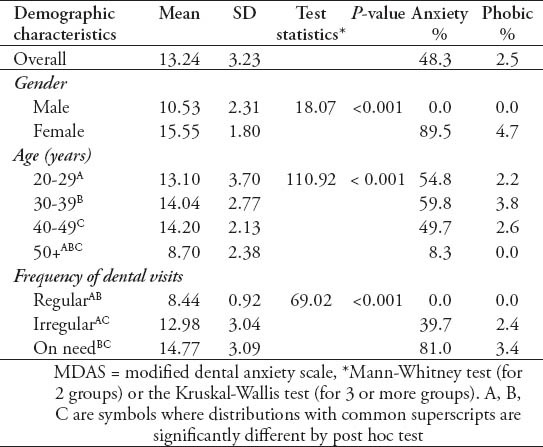
Comparison of the MDAS by gender, age, and frequency of dental visits (Table 3), verified known group validity. Females had significantly higher mean anxiety levels compared with males (15.55±1.80 versus 10.53±2.31). The level of anxiety was lowest for those aged 50 years or older (8.70±2.38) compared with all younger age groups. Furthermore, those who visited the dentist regularly had the lowest anxiety level (8.44±0.92) compared with irregular visitors (12.98±3.04), or those who visited the dentist only when needed (14.77±3.09). Subgroup comparisons with gender and frequency of dental visit combinations revealed the same results.
Table 3.
The MDAS by demographic characteristics among the studied patients.
Discussion
The main goal of the present study was to develop an Arabic translation and cultural adaptation of the MDAS, which is a valuable scale for identifying and managing levels of patient dental anxiety in Saudi Arabia. Highly anxious dental patients require greater attention during treatment, as special behavioral management strategies or additional pharmacological treatment.17 Simple and understandable modern standard Arabic language was used in the translation of the MDAS, instead of colloquial local language, so it would be acceptable and understandable to patients from all areas of Saudi Arabia and even all Arab countries.
The results of this study demonstrated that the MDAS had an excellent internal consistency and reliability for male, female, and total sample models (>0.90). The original, and a number of translated versions of the MDAS, have shown some variability in internal consistency results depending on content and the linguistic variation.10,18 Internal consistency values from these studies were lower (<0.80) for the Indian version of the MDAS (0.78)19 and the Anticipatory Dental Anxiety (ADA) factor (0.74) of the Chinese version of the MDAS.13 Higher values (>0.80) were found for the Spanish version (0.88),10 Romanian version (0.90),20 Turkish version (0.91),12 Greek version (0.90),21 United Kingdom version (0.957),22 and the Chinese MDAS (0.86).13 In the present study, the alpha reliability results indicated unidimensionality of the MDAS. In contrast, the 2-dimensional model provided a better fit in the validation study of the Chinese version of the MDAS.13
It is evident from the present study that the Arabic version of the MDAS is a valid scale. The VAS correlated significantly with individual items of the MDAS and the total anxiety score. Convergent validity was established by the strong positive correlations between the items of the scale, and the total score, as well as the VAS score; the latter also confirms the criterion validity. Construct validity was evident through the unidimensionality indicated by the alpha results.
There are different ways to choose a cutoff point on the MDAS. In our study, we selected the best cutoff based on the ROC curve results. As indicated by the ROC curve, the best cutoff value for dental anxiety in our study was >15, and the best cutoff for dental phobia was >16, such that 2.5% of patients were classified as highly anxious or dental phobic. Our results were similar to the findings of Acharya (2.2%) in the Indian population,12 and consistent with the MDAS in Turkish patients12 however, that scale uses a higher cutoff for diagnosing dental phobia (>19).
Our findings indicated that dental anesthetic injection was the procedure with the most influence on anxiety level, with a mean score of 3.25±0.87 in all samples, and that waiting in the dental office had the least influence on anxiety (2.32 ± 0.79). These findings are consistent with the results of Humphris et al,18 who found that dental anesthetic injection was the most anxiety-provoking item, with a mean score of 2.45±1.23 in all samples. However, they reported that scaling and polishing (1.90±1.35) was the least anxiety-provoking procedure, which is inconsistent with our findings.
The percentage of people with dental anxiety in this study was 48.3%, which is high in comparison with the results from Western countries such as the United Kingdom (11%),22 Northern Ireland (19.5%),18 Turkey (23.5%),12 and Finland (3%).18 The percentage of people with dental phobia was 2.5%. A relatively high percentage of anxious patients were expected, given that we approached our participants in the dental clinic waiting areas, and most were irregular visitors who visited the dentist only as needed. Motivating patients to visit the dentist more frequently may diminish this high level of anxiety. The high level of dental anxiety may have also resulted because the size of the older age group was relatively small. Our study showed that anxiety levels and phobias decrease with increases in age. We found that the lowest anxiety scores were recorded for those aged 50 years or older. This reduction in anxiety with increased age is in accordance with several other studies,13,19,23,24 which noted that the decline of anxiety with aging might be attributed to physiological changes in anxiety with age and the experience of diseases in the elderly that change their responses. These results are contrary to those of other studies that demonstrated positive correlations of anxiety level and age.12,25
Female patients in the present study experienced more anxiety than did male patients. This result is similar to findings of other studies that suggest differences in pain thresholds between genders as a possible explanation, given that female patients are more susceptible to anxiety disorders than male patients.19,21,26,27 We found that participants who visited the dentist on a regular basis were less dentally anxious than other participants. This could be because frequent dental visits enable a person to cope better with stress. In contrast, irregular visitors had more psychological problems and hence, could have had more fear toward dental treatment. Our results were similar to the findings of some previous studies;21,28 however, other studies showed no significant differences in dental anxiety scores between participants based on their frequency of dental visits and duration since the last dental visit.19
This study has some limitations. First, we tested only a few predictors of dental anxiety; future studies might include socio-economic status, education level, or other demographic variables which may be related to dental anxiety. Second, we used a convenience sample. A more heterogeneous sample would have improved generalization of the results. A third limitation is that criterion validity could not be established using standard scales, due to non-availability of translated and validated dental anxiety questionnaires in Saudi Arabia. Instead, we used the VAS scale as the criterion. A fourth limitation was that dentally phobic patients may have been underrepresented, because we sampled patients at general dental clinics rather than a clinic specializing in dentally fearful patients. A further point to be considered is related to generalizability. Our patients are similar in age and gender to those attending the Faculty of Dentistry Hospital, King Abdulaziz University, and are also similar in gender to the adult Saudi population, they were different in terms of age.29
Despite these limitations, our data indicated that the Arabic version of the MDAS has an adequate internal consistency and convergent and criterion validity in this sample, allowing its safe use to assess levels of dental anxiety in Arabic speaking populations. Areas of future research would include testing this scale in other areas of Saudi Arabia and in different Arab countries, to strengthen and ensure generalizability of the findings of this study. It is hoped that this version of the MDAS will be useful addition for both research and clinical settings involving Arabic-speaking adults.
Footnotes
Disclosure.
References
- 1.Kleinknecht R, Bernstein D. The assessment of dental fear. Behav Ther. 1978;9:626–634. [Google Scholar]
- 2.Corah NL. Dental anxiety. Assessment, reduction and increasing patient satisfaction. Dent Clin North Am. 1988;32:779–790. [PubMed] [Google Scholar]
- 3.Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc. 1978;97:816–819. doi: 10.14219/jada.archive.1978.0394. [DOI] [PubMed] [Google Scholar]
- 4.Corah NL. Development of a dental anxiety scale. J Dent Res. 1969;48:596. doi: 10.1177/00220345690480041801. [DOI] [PubMed] [Google Scholar]
- 5.Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health. 1995;12:143–150. [PubMed] [Google Scholar]
- 6.Humphris GM, Clarke HM, Freeman R. Does completing a dental anxiety questionnaire increase anxiety? A randomised controlled trial with adults in general dental practice. Br Dent J. 2006;201:33–35. doi: 10.1038/sj.bdj.4813772. [DOI] [PubMed] [Google Scholar]
- 7.Humphris GM, Hull P. Do dental anxiety questionnaires raise anxiety in dentally anxious adult patients? A two-wave panel study. Prim Dent Care. 2007;14:7–11. doi: 10.1308/135576107779398165. [DOI] [PubMed] [Google Scholar]
- 8.Appukuttan D, Datchnamurthy M, Deborah SP, Hirudayaraj GJ, Tadepalli A, Victor DJ. Reliability and validity of the Tamil version of Modified Dental Anxiety Scale. J Oral Sci. 2012;54:313–320. doi: 10.2334/josnusd.54.313. [DOI] [PubMed] [Google Scholar]
- 9.Coolidge T, Arapostathis KN, Emmanouil D, Dabarakis N, Patrikiou A, Economides N, et al. Psychometric properties of Greek versions of the Modified Corah Dental Anxiety Scale (MDAS) and the Dental Fear Survey (DFS) BMC Oral Health. 2008;8:29. doi: 10.1186/1472-6831-8-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coolidge T, Hillstead MB, Farjo N, Weinstein P, Coldwell SE. Additional psychometric data for the Spanish Modified Dental Anxiety Scale, and psychometric data for a Spanish version of the Revised Dental Beliefs Survey. BMC Oral Health. 2010;10:12. doi: 10.1186/1472-6831-10-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marginean I, Filimon L. Modified Dental Anxiety Scale: a validation study on communities from the west part of Romania. Int J Edu Psychol Community. 2012;2:102–114. [Google Scholar]
- 12.Tunc EP, Firat D, Onur OD, Sar V. Reliability and validity of the Modified Dental Anxiety Scale (MDAS) in a Turkish population. Community Dent Oral Epidemiol. 2005;33:357–362. doi: 10.1111/j.1600-0528.2005.00229.x. [DOI] [PubMed] [Google Scholar]
- 13.Yuan S, Freeman R, Lahti S, Lloyd-Williams F, Humphris G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual Life Outcomes. 2008;6:22. doi: 10.1186/1477-7525-6-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abu-Ghazaleh SB, Rajab LD, Sonbol HN, Aljafari AK, Elkarmi RF, Humphris G. The Arabic version of the modified dental anxiety scale. Psychometrics and normative data for 15-16 year olds. Saudi Med J. 2011;32:725–729. [PubMed] [Google Scholar]
- 15.Sartorius N, Kuyken W. ‘Translation of health status Instruments’. In: Orley J, Kuyken W, editors. Quality of Life Assessment. International Perspectives. New York (NY): Springer-Verlag; 1994. [Google Scholar]
- 16.Facco E, Zanette G, Favero L, Bacci C, Sivolella S, Cavallin F, et al. Toward the validation of visual analogue scale for anxiety. Anesth Prog. 2011;58:8–13. doi: 10.2344/0003-3006-58.1.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Meniglia-Ferreira C, Gurgel-Filho E, Bonecker-Valverde G, Moura E, de Deus G, Coutinho-Filho T. [Dental anxiety: score, prevalence and behavior] Revista Brasileira em Promoção da Saúde. 2004;17:251–255. Portuguese. [Google Scholar]
- 18.Humphris GM, Freeman R, Campbell J, Tuutti H, D’Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50:367–370. doi: 10.1111/j.1875-595x.2000.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 19.Acharya S. Factors affecting dental anxiety and beliefs in an Indian population. J Oral Rehabil. 2008;35:259–267. doi: 10.1111/j.1365-2842.2007.01777.x. [DOI] [PubMed] [Google Scholar]
- 20.Marginean I, Filimon L. Modified Dental Anxiety Scale: a validation study on communities from the west part of Romania. Int J Edu Psychol Community. 2012;2:102–114. [Google Scholar]
- 21.Luyk NH, Beck FM, Weaver JM. A visual analogue scale in the assessment of dental anxiety. Anesth Prog. 1988;35:121–123. [PMC free article] [PubMed] [Google Scholar]
- 22.Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009;9:20. doi: 10.1186/1472-6831-9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liddell A, Locker D. Gender and age differences in attitudes to dental pain and dental control. Community Dent Oral Epidemiol. 1997;25:314–318. doi: 10.1111/j.1600-0528.1997.tb00945.x. [DOI] [PubMed] [Google Scholar]
- 24.Settineri S, Tati F, Fanara G. Gender differences in dental anxiety: is the chair position important? J Contemp Dent Pract. 2005;6:115–122. [PubMed] [Google Scholar]
- 25.Thomson WM, Locker D, Poulton R. Incidence of dental anxiety in young adults in relation to dental treatment experience. Community Dent Oral Epidemiol. 2000;28:289–294. doi: 10.1034/j.1600-0528.2000.280407.x. [DOI] [PubMed] [Google Scholar]
- 26.Desai VD, Gaurav I, Bailoor DN. Dental anxiety - an area of concern for the oral physician - a study. J Indian Dent Assoc. 2011;5:177–179. [Google Scholar]
- 27.Malvania EA, Ajithkrishnan CG. Prevalence and socio-demographic correlates of dental anxiety among a group of adult patients attending a dental institution in Vadodara city, Gujarat, India. Indian J Dent Res. 2011;22:179–180. doi: 10.4103/0970-9290.79989. [DOI] [PubMed] [Google Scholar]
- 28.Woolgrove J, Cumberbatch G. Dental anxiety and regularity of dental attendance. J Den t. 1986;14:209–213. doi: 10.1016/0300-5712(86)90003-5. [DOI] [PubMed] [Google Scholar]
- 29.Riyadh (KSA): Central Department of Statistics & Information; 2007. Ministry of Economy and Planning. Population & Housing Characteristics in the Kingdom of Saudi Arabia. Demographic survey 1428 RAH. Available from: http://www.cdsi.gov.sa/pdf/demograph.pdf . [Google Scholar]