

Abstract
Objectives
To determine whether the theory of planned behavior (TPB) predicted intent of child restraint system (CRS) use among pregnant women in the Kingdom of Saudi Arabia (KSA).
Methods
In this cross-sectional study conducted in Dallah Hospital, Riyadh, KSA during June-July 2013, 196 pregnant women completed surveys assessing their beliefs regarding CRS. Simultaneous observations were conducted among a different sample of 150 women to determine CRS usage at hospital discharge following maternity stay.
Results
Logistic regression model with TPB constructs and covariates as predictors of CRS usage intent was significant (χ2=64.986, p<0.0001) and predicted 38% of intent. There was an increase in odds of intent for attitudes (31.5%, p<0.05), subjective norm (55.3%, p<0.001), and perceived behavioral control (76.9%, p<0.001). The 3 logistic regression models testing the association of the relevant set of composite belief scores were also significant for attitudes (χ2=16.803, p<0.05), subjective norm (χ2=29.681, p<0.0001), and perceived behavioral control (χ2=20.516, p<0.05). The behavioral observation showed that none of the 150 women observed used CRS for their newborn at discharge.
Conclusion:
The TPB constructs were significantly and independently associated with higher intent for CRS usage. While TPB appears to be a useful tool to identify beliefs related to CRS usage intentions in KSA, the results of the separate behavioral observation indicate that intentions may not be related to the actual usage of CRS in the Kingdom. Further studies are recommended to examine this association.
According to the Ministry of Interior of the Kingdom of Saudi Arabia (KSA), mortality from road traffic accidents has continued to climb, and in 2011 has reached 7,153 fatalities compared with 4,848 in 2000, contributing to an overall rate increase of 27% over a 10-year period.1,2 While the Saudi traffic laws are in line with the rest of the developed countries, and require use of seatbelts and child restraint systems (CRS),3 limited studies show that few passengers use seatbelts in moving vehicles,4,5 and even fewer use CRS for their children.6 Based on the World Health Organization (WHO) Global Status Report on Road Safety,7 out of 6 traffic laws (CRS, motorcycle helmet, seat belt, speed limits, drunk driving, use of mobile phones), only 2 (seat belt and drunk driving) received a score of 8 for the enforcement (on a scale of 0-10, based on the professional opinion of respondents, in which 0 is not effective, and 10 is highly effective). While most scores improved compared with the 2007 report,8 it is of concern that the CRS enforcement score decreased from ‘2’ in 2007 to ‘one’ in a 2013 report. As there is no strict enforcement of this law in KSA presently, it is possible that CRS law is viewed by Saudi women as merely a suggestion, rather than a safety requirement. Another potential contributor to the low usage of infant restraints is revealed in a Riyadh Traffic Department survey results,1 which show that 63% of drivers reported no respect for traffic laws. This observation, paired with poor enforcement, suggests that there is a need to develop an awareness campaign to promote the use of infant restraints in KSA. Such a campaign would be more effective, if it targeted the specific beliefs held regarding the use of infant restraints. In order to develop an appropriate intervention for this population, one needs to identify the prevalent beliefs regarding the use of infant restraints, as they may differ from that in the rest of the world, and how well those beliefs will predict the intent and behavior in KSA. A number of prior studies have demonstrated the theory of planned behavior (TPB) is effective in predicting intentions and behavior including several traffic safety studies.9-11 The meta-analysis conducted by Armitage and Conner12 demonstrated that TPB explained 27% of the behavior variance, and 39% of the intention variance across 185 research studies. We explored whether the TPB constructs had sufficient predictive power on the intent to use infant restraints in KSA as it has for health behaviors in other areas of the world. The purpose of this study was to test whether attitude, subjective norm (SN), and perceived behavior control (PBC) significantly, and independently predicted intent to use infant restraints in Saudi pregnant women. The composite variables of beliefs and their valuations, which underlie these constructs were also examined to determine, which of them independently predicted attitude, SN, and PBC.
Methods
The Loma Linda University Institutional Review Board (IRB), Loma Linda, California, United States of America and Dallah Hospital, Riyadh, KSA approved this study in accordance with the Belmont Report (http://www.hhs.gov/ohrp/humansubjects/guidance/belmont.html). This was a cross-sectional study surveying Saudi pregnant women on their beliefs regarding infant restraints. Participants were recruited from Dallah Hospital, a private tertiary care teaching hospital in Riyadh, and participated in the study during the month of June 2013. Hospital representatives approached individuals in the waiting rooms at the time of regularly scheduled appointments with an invitation to participate in the study, and explained the requirements. All Saudi pregnant women at any stage of pregnancy were eligible to enter the study. There was no exclusion criteria. Consenting participants were invited to complete a 20-minute anonymous written survey before leaving the hospital. A 20 Saudi riyal (equivalent to US$5.33) gift coupon was provided to each participant. Of the 220 consenting women who agreed to complete the surveys, 196 (89%) responded to all of the questions. Twenty-four surveys, which had missing data were not used in the study.
Survey
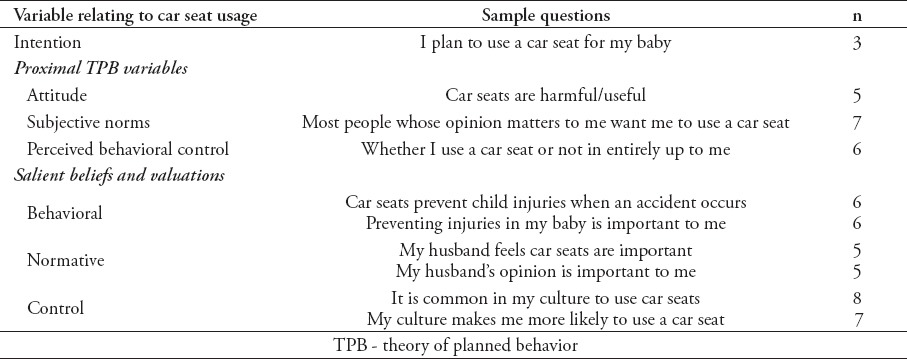
The survey had a total of 66 questions, and included 8 socio-demographic and traffic safety practices questions. The remaining questions assessed intentions, attitudes, SN, and PBC, as well as the underlying salient beliefs and corresponding valuations regarding the use of car seats. Table 1 lists the number and sample of questions for each of the 7 key study variables. The complete survey is available upon request.
Table 1.
Number of survey items and sample wording for each research variable used in a study on child restraint system (N=58).
Calculation of TPB constructs and intent variables
Following Ajzen’s guidelines for questionnaire development,13 we developed several statements to measure the intent variable, as well as each of the TPB constructs. All items used a 7-point Likert-type scale responses, except those for attitude, which relied on a 7-point semantic differential scale. Based on the internal reliability analysis, we kept 3 statements for the intent variable (Cronbach’s alpha [α]=0.830), 5 for attitude (α=0.942), 7 for SN (α=0.930), and 6 for PBC (α=0.791). We then used the average of the responses to the respective questions in the survey to calculate the mean variables of intentions, attitudes, SN, and PBC.
Calculation of composite belief scores
The behavioral, normative, and control beliefs were delineated in focus groups during the initial qualitative portion of this study.14 Based on the guidelines of Ajzen,13 the belief statements were paired with a scale from one to 7, from strongly disagree to strongly agree as scale anchors. The outcome evaluation statements for each belief were created based on the belief statement, and used a 7-point response scale from -3 to +3, with strongly disagree to strongly agree as scale anchors. For example, to measure the power of the behavioral belief “Car seats prevent child injuries in case of an accident”, we formulated the following evaluation statement: “Preventing injuries for my baby in an accident is important to me”. The scores for each of the belief statements were multiplied by the score for the corresponding outcome evaluation to form a composite variable for each belief. The bipolar scaling of the outcome evaluation variables made it easier to interpret the final results, with positive scores indicating a positive attitude towards car seat usage, and negative scores indicating a negative attitude towards the use of car seats.
Survey translation
As most participants did not read English, the survey was translated into Arabic using the method proposed by Jones et al.15 A team of independent interpreters translated the survey back and forth between English and Arabic until a consensus was reached among the team of interpreters and the researchers. The Arabic questionnaire was piloted among 8 Saudi women to establish that the questions were easy to understand and respond to. Minor corrections and modifications were made based on the results of the pilot test.
Behavior observation
An observation of a separate sample of women was conducted to document the current trend of infant restraint usage by women who had just delivered their baby. Two nurses conducted observations at the exit of the obstetrics/gynecology wing of Dallah Hospital over a period of 2 weeks during the month of July 2013. Observations were conducted between 12:00 noon and 8:00 pm. The nurses discretely monitored mothers leaving the hospital for the presence and usage of car seats in the vehicles, which were used to pick up patients. These observations were anonymous not only because the observers did not know the patients’ names, but also because the patients’ faces were veiled, as is common in Saudi culture.
Data analysis
The completed surveys were entered and processed using the Statistical Package for Social Sciences version 20 (IBM Corp, Armonk, NY, USA).16 Due to non-normal distribution of the residuals, we used logistic regression analysis instead of multiple linear regression. The value of the mean score for the intention variable was 7 on the 7-point scale for 58.2% of the participants. The variable was categorized to a binomial variable of high and lower intent. Given the distribution, all responses below 7 were categorized as lower intent, and responses of 7 were categorized as high intent. To determine the goodness-of-fit, Nagelkerke pseudo R2 results were used to state the percentage of outcomes explained.
Results
The socio-demographic characteristics and traffic safety practices of the sample are presented in Table 2.
Table 2.
Socio-demographic characteristics and traffic safety practices among Saudi pregnant women (n = 196, except where noted).

Table 3.
Multiple logistic regression of association of the theory of planned behavior (TPB) constructs and the intent to use restraints among pregnant women in the Kingdom of Saudi Arabia (n = 196).
Actual behavior observation
In order to preserve the anonymity of the study and ensure that testing was not one of the influencing factors on the outcome, we chose not to measure the car seat usage among the survey participants at the end of pregnancy. Instead, we conducted a separate observation of 150 women at the time of their discharge from their maternity stay at Dallah hospital. All women left the hospital in private cars with drivers. Of the 150 women, none used a car seat for their infants, and each left the hospital holding the infant in their arms. Two of the cars did have car seats installed, but the mothers were holding their infants as the cars drove away. This noncompliance is distinct from that reported by survey participants who already had children; 58.2% of them indicated they used a car seat for the child.
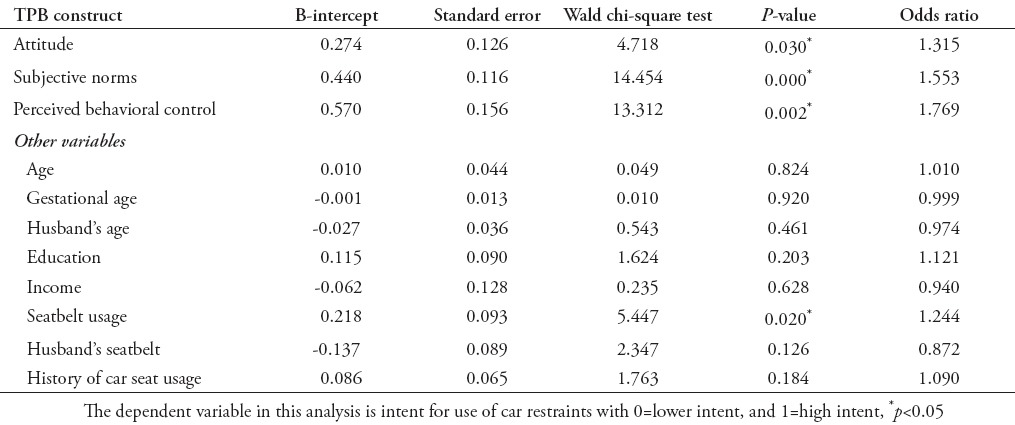
Association of TPB proximal values with intention to use car seats
According to the survey’s data analysis, there was a significant difference between the high and lower intent groups on the items relating to the TPB proximal values with the high intent group having higher scores on the constructs of attitude, SN, and PBC (p<0.001). Logistic regression analysis was performed with the binomial variable of intent as the outcome variable, and the mean scores for each proximal TPB construct as the predictor variables. Additional covariates included the participants’ age, gestational age, husband’s age, participant’s education, income, personal, and husband’s use of seatbelts, and past history of car seat usage. Table 4 presents the results. A test of the full model against a constant only model was statistically significant, indicating that the set of 3 proximal TPB constructs reliably distinguished between high and lower intent groups with higher scores for TPB constructs being related to high intent (χ2=64.986. p<0.0001 with df=11). Overall, the full model predicted 38% of intent to use car seats based on Nagelkerke R2. Prediction success of the overall model was 72.4%, and was higher for the high intent group, based on proximal TPB scores. Over half of the respondents with children (58.2%) stated that they had used car seats in the past. Given the results of no car seat usage among observations of a separate sample of 150 women conducted at approximately the same time, this outcome suggests that some participants may have responded in a socially desirable manner to this question. A similar trend was observed for the question of seatbelt usage by the women: 26% of participants marked the highest score of “7” for use of seatbelt. Based on the discrepancy regarding car seat usage, there is a concern that this may be overly optimistic, and may not reflect the true rate of seatbelt usage. As there may be some doubt regarding the veracity of reporting of these 2 variables, we tested the model excluding the 2 covariates of seatbelt usage, and history of car seat usage. The results were similar to the previous model. A test of this model was also statistically significant (χ2=56.515, p<0.0001 with df=9). Overall, the model that excluded the 2 covariates predicted 33.7% of intent to use car seats based on Nagelkerke R2. Prediction success was 73%. All 3 of the constructs remained significant in this model with odds changing only slightly compared with the original model. The results show that each unit increase in attitude score increased the odds of intent to use car seats by 30.4% (p<0.05). Each unit increase in SN score increased the odds of intent by 59.7% (p<0.0001), which was slightly better than the other model. Each unit increase in PBC score was associated with the 75.1% increase in the odds of intent (p<0.0001).
Table 4.
Logistic regression analysis of the effect of salient behavioral belief composite scores on attitude toward car seat usage among pregnant women in the Kingdom of Saudi Arabia (n = 196)

Association of salient behavioral beliefs with attitude
As the mean attitude variable created by averaging all responses to the 5 attitudinal items did not have a normal distribution, it was categorized as a binomial variable based on a median split. All scores of 6.8 and below were categorized as lower attitude, and scores above 6.8 were categorized as high (positive) attitude towards car seat use. The composite scores for each of the behavioral belief items were computed by multiplying the score of the belief by its valuation. Logistic regression analysis was performed to determine whether there was an independent association between each of the 6 behavioral belief composite scores, and attitude (Table 4). Of the 6 beliefs that were tested, only one (that is, ‘Car seats can protect my baby from injury in case of an accident’) was independently associated with the attitude towards car seats. A test of the full model against a constant only model was statistically significant, indicating that all behavioral beliefs as a set reliably distinguished between high and lower intent groups (χ2=16.803, p<0.05 with df=6). The full model predicted 11% of intent to use car seats based on Nagelkerke R2. The overall prediction success was 64.3% (65.7 for lower and 62.8 for higher intent groups). This low result may be explained by the low variability in the attitude scores.
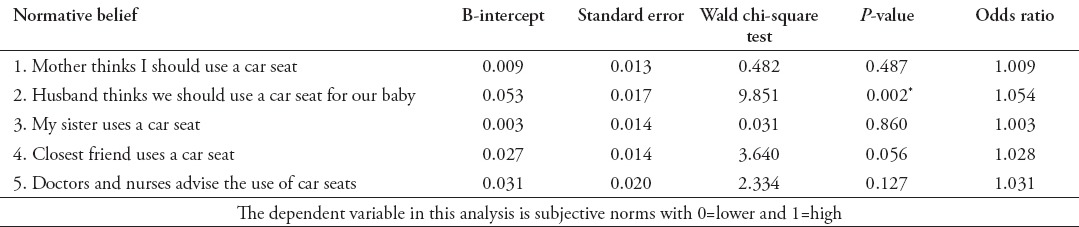
Association of salient normative beliefs with SN
As the SN mean scores were not normally distributed, this variable was divided by a median split into 2 categories: the values above 5.6 were categorized as high SN, and the remaining scores were categorized as lower SN. The individual normative belief composite scores were computed by multiplying the score of each belief to the corresponding valuation (motivation to comply). The association was then tested using logistic regression with the categorical variable of SN as the outcome variable, and the composite scores for normative beliefs as predictors (Table 5). A test of the full model against a constant only model was statistically significant, indicating that the 5 normative beliefs as a set reliably distinguished between high and lower SN groups (χ2=29.681, p<0.0001 with df=5). The model predicted 18.7% of the SN based on Nagelkerke R2. Prediction success overall was 63.8% (61.4 for lower SN, and 66.3 for high SN groups).
Table 5.
Logistic regression analysis of the effect of salient normative beliefs on the subjective norms among pregnant women in the Kingdom of Saudi Arabia (n = 196).
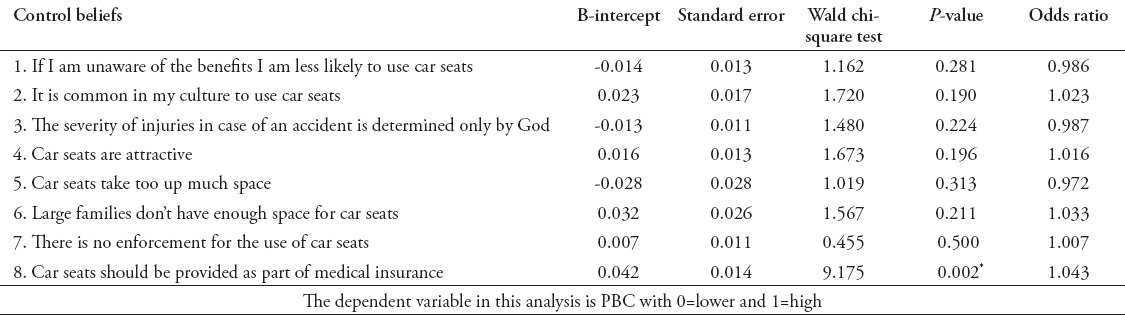
Association of control beliefs and perceived behavioral control
The variables used to test the association of control beliefs with PBC were determined in a similar way as in the above tests. Due to non-normal distribution, PBC was divided into high and lower categories at the median split. The values above 5.75 were categorized as high PBC, and the rest as lower PBC. The individual control belief composite scores were calculated by multiplying belief values by their respective valuations. The association was then tested using logistic regression test with the categorical variable of PBC as the outcome variable, and the individual control belief composites as predictors (Table 6). A test of the full model against a constant only model was statistically significant, indicating that the 8 control beliefs as a set reliably distinguished between high and lower PBC groups (χ2=20.516, p<0.05 with df=8). The model explained 13.3% of intent to use car seats based on Nagelkerke R2. Prediction success overall was 64.3% (65 for lower and 63.5 for high intent groups). The low result may be due to the low variability in responses.
Table 6.
Logistic regression analysis of the effect of salient control beliefs on perceived behavioral control (PBC) (n = 196).
Discussion
In our study, the key TPB constructs of attitude, SN, and perceived behavioral control predicted 38% of the intentions to use car seats among Saudi pregnant women. This agrees with other TPB studies conducted in the Middle East, such as an Iranian study,10 which showed that TPB predicted 38% of intentions for seat belt use. The TPB studies relating directly to CRS have shown similar results. In a Canadian study,11 TPB predicted 30% of the use of booster seats. Further studies needs to be conducted in KSA to examine the relationship between intention and behavior in the same sample.
Only 3 of all beliefs tested were significant independent contributors to attitudes, SN, and PBC. It is possible that the low variability of responses for both the beliefs and proximal TPB variables contributed to such results. Low variability suggests that the respondents did not use the full scale when responding to the survey, which limited the analysis we could perform, and thus, may have prevented us from uncovering potential associations. Two of the beliefs ‘Car seats can protect my baby from injury in case of an accident,’ and ‘Husband thinks we should use a car seat for our baby’ - have been mentioned previously in the literature as significant beliefs in determining intentions for CRS.17 As husbands were demonstrated to have a significant effect on women’s decision regarding the use of car seats, car dealerships, and gas stations could be approached to develop educational campaigns geared specifically to men, especially since women do not currently drive in KSA. Further studies would be useful to explore Saudi men’s opinions regarding the use of car seats.
The belief that ‘car seats should be provided as part of medical insurance’ has not been identified in prior literature, although car seat loan programs have been researched and found successful.18 It is possible that if car seats were provided as part of medical insurance, it would carry a message to the public that the medical community and the government strongly endorse the use of CRS. The observation of the actual behavior of car seat usage on a separate sample showed that none of the 150 observed women used a car seat upon discharge from the hospital. It is possible that in our study, women and their families did not feel comfortable to use CRS for their newborns as they left the hospital. One could argue that they may choose to do so at a later time. While to our knowledge, the actual CRS usage has not been measured in Saudi Arabia, our findings of car seat usage observations correspond to the self-report-based study by Jan et al,6 in which only 8% of parents reported use of car seats, and only 3.7% parents of children under 5. Further studies need to be conducted to determine the prevalence of car seats usage as infants grow. These observations can be carried out in a variety of settings, such as during mandatory immunizations visits at the hospital, at kindergartens, schools, and daycare centers. Meanwhile, additional enforcement could encourage compliance, such as a hospital policy requiring all infants to be restrained in CRS prior to discharge.
A number of participants marked responses at the top, or bottom of the 7-point scale for the items relating to their personal seatbelt usage, or past history of CRS, as well as some of the key TPB variables. As they did not tend to use the entire 7-point scale, this implies that a scale with fewer categories than typically used might be sufficient for this population. According to a review of literature by Choi and Pak,19 long surveys may contribute to a survey respondent fatigue bias, which may result in participants marking just the extreme positive or negative responses of the scale. It is possible that the responses did not always reflect reality, but that the participants wished to mark the socially desirable responses despite the fact that the surveys were anonymous. While studies, including those studying social desirability responses, suggest that the self-administrated questionnaire method may yield the most accurate results,20 there have been suggestions that certain studies may need to rely on other methods of data collection.21 It is of interest that during focus group interviews conducted in preparation for this research, participants expressed responses, which appeared to match the actual behavior observations of no car seat usage as reported in the independent sample in this study. This finding may have significant implications for future research among this particular population; participants may be more open in their responses if they complete a survey in a confidential face-to-face interview compared with an anonymous self-administered survey.
In summary, the current trends of CRS usage demonstrate a need for stronger enforcement (that is, hospital policy, traffic police enforcement) of CRS regulation in KSA. The key constructs of TPB were significantly associated with intention to use CRS among Saudi pregnant women. The TPB constructs and specific beliefs found as significant independent predictors of the proximal TPB constructs of attitude, SN, and perceived behavioral control in this study should be utilized in developing national health interventions, to educate parents of the importance of CRS.
The study objective was to examine the effect of the 3 constructs of TPB and their underlying beliefs on the intent to use car seats in pregnant women in KSA. This study also aims to document observed usage of infant restraints in Saudi Arabia. The study brings to light an important issue of child car safety in Saudi Arabia largely neglected by most of the population.
One of the study limitations is that this research relied on data restricted to a single hospital, which would make it difficult to generalize to all of Riyadh and Saudi Arabia. It should be noted, however, that Dallah Hospital is a private tertiary care, community hospital in the center of the capital of KSA, and may only be representative of the Riyadh population. While the salient beliefs contributing to attitudes, SN, and PBC may be representative of Riyadh population of women, they may not reflect the beliefs of women living in other cities of Saudi Arabia. Furthermore, the results may not be generalizable to the wider population of Saudi Arabia residing outside of urban centers, although it would be unlikely to see greater car seat usage in such areas. Another limitation is the fact that some of participants may have misrepresented their behavior, or perceptions by selecting socially desirable responses for some of the questions. Specifically, 58.2% of women reported they have used car seats for their children in the past. None of the women in the observed sample however, used a car seat for their infants at the time of discharge from hospital. Just as there may be some bias in the history of car seat usage variable, there is a possibility that a similar bias may be present in the intent, and personal use of seat belts. One way to avoid such bias in the future would to administer surveys by conducting individual confidential interviews.
Future prospective studies of the actual behavior performance in the same sample of women who respond to the questionnaire could suggest whether intention and PBC predict behavior, as the theory suggests.
Acknowledgment
The authors gratefully acknowledge the Administration and the Obstetrics and Gynecology Department of Dallah Hospital, Riyadh, KSA, and specifically Dr. Mohammed Alfagih and Dr. Lamia Khaleel for their kind support and active assistance in this study.
Footnotes
Disclosure.
References
- 1.Ministry of Interior. General Department of Traffic Statistics. [cited 2012 May 12];2012 [Google Scholar]
- 2.Cairo (Egt): Regional Office for Eastern Mediterranean; 2007. World Health Organization. Country cooperation strategy for WHO and Saudi Arabia 2006-2011. Available from: www.who.int/countryfocus/cooperation_strategy/ccs_sau_en.pdf . [Google Scholar]
- 3.Bendak S. Compliance with seat belt enforcement law in Saudi Arabia. Int J Inj Contr Saf Promot. 2007;14:45–48. doi: 10.1080/17457300600841726. [DOI] [PubMed] [Google Scholar]
- 4.Crankson S. Motor vehicle injuries in childhood: a hospital-based study in Saudi Arabia. Pediatr Surg Int. 2006;22:641–645. doi: 10.1007/s00383-006-1715-7. [DOI] [PubMed] [Google Scholar]
- 5.Naeem Z. Road traffic injuries - changing trend? Int J Health Sci (Qassim) 2010;4:v–viii. [PMC free article] [PubMed] [Google Scholar]
- 6.Jan MM, Hasanain FH, Al-Dabbagh AA. Infant and child safety practices of parents. Saudi Med J. 2000;21:1142–1146. [PubMed] [Google Scholar]
- 7.Geneva (CH): World Health Organization; 2013. World Health Organization, WHO global status report on road safety. 2013: supporting a decade of action. Available from: www.who.int/iris/bitstream/10665/78256/1/9789241564564_eng.pdf . [Google Scholar]
- 8.Geneva (CH): World Health Organization; 2007. World Health Organization. Road Safety Country Profile. [Google Scholar]
- 9.Elliott MA, Armitage CJ. Promoting drivers’ compliance with speed limits: Testing an intervention based on the theory of planned behaviour. Br J Psychol. 2009;100:111–1132. doi: 10.1348/000712608X318626. [DOI] [PubMed] [Google Scholar]
- 10.Tavafian SS, Aghamolaei T, Gregory D, Madani A. Prediction of seat belt use among Iranian automobile drivers: application of the theory of planned behavior and the health belief model. Traffic Inj Prev. 2011;12:48–53. doi: 10.1080/15389588.2010.532523. [DOI] [PubMed] [Google Scholar]
- 11.Bruce BS, Snowdon AW, Cunningham C, Cramm CL, Whittle K, Correale H, et al. Predicting parents’ use of booster seats. Inj Prev. 2011;17:313–318. doi: 10.1136/ip.2010.029181. [DOI] [PubMed] [Google Scholar]
- 12.Armitage CJ, Conner M. Efficacy of the Theory of Planned Behaviour: a meta-analytic review. Br J Soc Psycho. 2001;40:471–499. doi: 10.1348/014466601164939. [DOI] [PubMed] [Google Scholar]
- 13.Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health. 2011;26:1113–1127. doi: 10.1080/08870446.2011.613995. [DOI] [PubMed] [Google Scholar]
- 14.Nelson A, Modeste N, Hopp Marshak H, Hopp JW. Saudi Women's Beliefs on the Use of Car Infant Restraints: a Qualitative Study. Traffic Inj Prev. 2014 doi: 10.1080/15389588.2014.931578. [DOI] [PubMed] [Google Scholar]
- 15.Jones PS, Lee JW, Phillips LR, Zhang XE, Jaceldo KB. An adaptation of Brislin's translation model for cross-cultural research. Nurs Res. 2001;50:300–304. doi: 10.1097/00006199-200109000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Armonk (NY): IBM Corp; 2011. IBM Corp. Released 2011. IBM SPSS Statistics for Windows Version 20.0. [Google Scholar]
- 17.Radius SM, McDonald EM, Bernstein L. Influencing car safety seat use: prenatal and postnatal predictors. Health Values. 1991;15:29–38. [Google Scholar]
- 18.Kedikoglou S, Belechri M, Dedoukou X, Spyridopoulos T, Alexe DM, Pappa E, et al. A maternity hospital-based infant car-restraint loan scheme: public health and economic evaluation of an intervention for the reduction of road traffic injuries. Scand J Public Health. 2005;33:42–49. doi: 10.1080/14034940410028334. [DOI] [PubMed] [Google Scholar]
- 19.Choi BC, Pak AW. A Catalog of biases in questionnaires. Prev Chronic Dis. 2005;2:13. [PMC free article] [PubMed] [Google Scholar]
- 20.Ramo DE, Hall SM, Prochaska JJ. Reliability and validity of self-reported smoking in an anonymous online survey with young adults. Health Psychol. 2011;30:693–701. doi: 10.1037/a0023443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bergmann M, Jacobs E, Hoffmann K, Boeing H. Agreement of self-reported medical history: comparison of an in-person interview with a self-administered questionnaire. Eur J Epidemiol. 2004;19:411–416. doi: 10.1023/b:ejep.0000027350.85974.47. [DOI] [PubMed] [Google Scholar]