

Abstract
Objectives:
To estimate the frequency of urinary problems among preschool children.
Methods:
In this cross-sectional study, 1000 preschool asymptomatic children attending the outpatient clinics of the Children’s Hospital, Taif, Kingdom of Saudi Arabia between August 2013 and December 2013 were subjected to dipstick urine analysis. Microscopic examination was performed for the abnormal dipstick samples, and children with hematuria were investigated for kidney function.
Results:
Dipstick urine analysis revealed abnormal findings in 25.1% of the screened children. The most common dipstick abnormalities were positive nitrite test in 18.1%, hematuria in 16.9%, and positive leukocyte esterase test in 14.3% of the cases. The most common abnormality in microscopic urine examination was crystals in 13% of the cases. Pyuria were evident in 5% of cases and hematuria in 2.5%. The most common bacteria in positive urine culture samples was Escherichia coli in 62.6%.
Conclusion:
In view of these important findings, dipstick screening should be implemented in preschool children.
Chronic kidney disease (CKD) is a global public health problem, its incidence is steadily increasing among children.1 The Kingdom of Saudi Arabia (KSA) is a large country (26.9 million) populated with a high percentage of children; children aged 0-14 years represent 28.2% of the population.2 The Kingdom of Saudi Arabia is similar to other developing countries in that there is no current national epidemiologic data on pediatric chronic renal failure (CRF) and its risks.3 Detection and management of renal problems in children are of major importance for CKD prevention; this in turn will decrease the burden of CKD in the pediatric population.4 Urinalysis is recognized as the simplest and least expensive method for screening healthy children and dipstick method is the most commonly implemented procedure.5 Moreover, dipstick has proven effective in prediction of rapidly declining kidney function.6 It must be recognized that not all abnormal results are clinically significant, and that false positive and false negative results can exist.7 Moreover, there is uncertainty as to whether early detection of renal disorders in children will lead to prevention of development of end-stage renal disease (ESRD). However, there is a clear consensus among Japanese, Taiwanese, and Korean investigators that the screening programs currently in place in these counties have led to early detection and effective intervention.8 Proteinuria and hematuria are among the early manifestations of renal disease.9 The presence of a dipstick test 1+ or ≥2+ for proteinuria was strongly associated with renal risk.10 Hematuria can be caused by several conditions, including infections, stone disease of the urinary tract, glomerular, and tubular disorders.11 Nitrite in urine has also been used to diagnose urinary tract infection; a common condition in childhood with serious complications.12 The treatment of persistent proteinuria should be directed toward the underlying cause. Steroid therapy may be used. Other therapies may be required in patients with renal dysfunction (namely, cyclophosphamide, chlorambucil, cyclosporine). Additionally, angiotensin-converting enzyme inhibitor and/or angiotensin-II receptor blocker can be used to the slow progression of renal disease and decreasing proteinuria. Referral to a pediatric nephrologist may be needed for further management.13 The aim of the current study was to screen for hematuria and other urine abnormalities among children in Taif city, as early detection could aid in preventing the progression of renal diseases.
Methods
Study design and settings
This cross-sectional study was conducted at the Children Hospital, Taif, Kingdom of Saudi Arabia. This hospital is government-funded, and serves approximately 400 children daily.
This study was approved and funded by the Review Board Committee of Taif University. We included all preschool children (aged 3-6 years) with no history of renal disease. These subjects were accompanying sick children who attended the outpatient clinics during the period from August 2013 to December 2013. Exclusion criteria were children with fever, abdominal pain, vomiting, diarrhea, acute voiding symptoms, facial or leg swelling, and children with severe malnutrition or other chronic debilitating diseases. A written consent was obtained from parents prior to the start of the study.
Screening protocol
Urine containers were collected from the children after instructing their parents on how to obtain a clean midstream urine specimen. Parents were also given a questionnaire on family history of renal problems, residence, mothers’ education, mothers’ work, family income, and crowding index. Urine specimens were tested for physical characters including abnormal color or aspect and examined immediately by dipstick method. In this study, the dipstick was adopted from the Medi-Test combi 10® (SGL, Düren, Germany), consisting of 10 reagents, including: pH, specific gravity, protein, blood, glucose, leucocytes, nitrite, urobilinogen, bilirubin, and ketones. Children with positive dipstick results were subsequently subjected to microscopic urine examination and urine culture. For cases with hematuria, blood samples were collected and sent for urea, creatinine, and uric acid measurements.
The following case definitions were applicable: 1) hematuria: more than 5 red blood cells per high power field (RBC/HPF) 2) Pyuria: more than 10 white blood cells per high power field (WBC/HPF). 3) >1 proteinuria. 4) >1 glycosuria. 5) positive nitrite.
Statistical analysis
Data was analyzed using the Statistical package for Social Sciences Version 20.0 (Armonk, NY: IBM Corp.). The frequency tables (number, percentage) were calculated for all measurements. Chi-square test was used for comparison of categorical variables. Significance was detected at p<0.05.
Results
Table 1 shows that 1000 apparently healthy children were included in this study. Six percent (n=60) had a family history of renal problems, and 7.8% (n=78) were overweight. Most of the studied children were aged 60-72 months. Approximately 51% were females and nearly 62% were rural residents. Most of their mothers were educated housewives and most parents were unsatisfied with their income. Table 2 reveals that from the 25 hematuria cases, 3 had elevated blood urea, 8 had elevated serum creatinine and 7 had hyperuricemia. Figure 1 shows that dipstick examination of urine samples revealed abnormal results in screened children, positive nitrite, hematuria, positive leukocyte esterase, glucose, and protein. Figure 2 shows that microscopic examination of abnormal dipstick urine samples showed crystals and epithelial cells. Pyuria was evident in 50 cases while hematuria was present in 25 cases. Figure 3 shows that the most common bacteria encountered in the positive urine cultures, were Escherichia coli (E. coli) in 62.6% (15 cases), followed by Enterococci in 20.8% (5 cases). The only microscopic urine findings that differed significantly between male and female children were crystals and epithelial cells; they were significantly higher in females. The variables were examined using Chi-square test. Statistical significance was defined as p-values of less than 0.05.
Table 1.
Children characteristic among 1000 apparently healthy children.
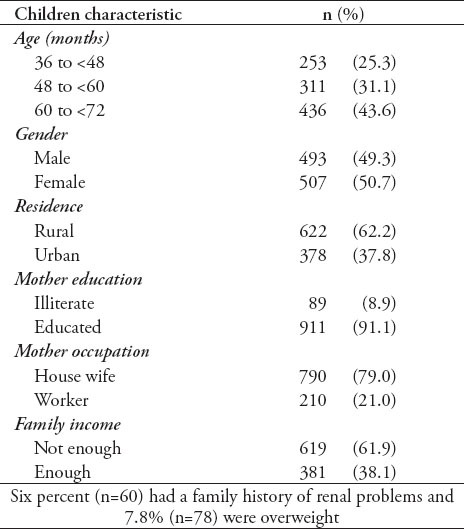
Table 2.
Investigations carried out for the 25 cases with microscopic hematuria.
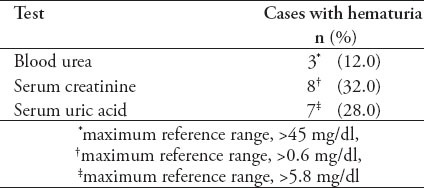
Figure 1.
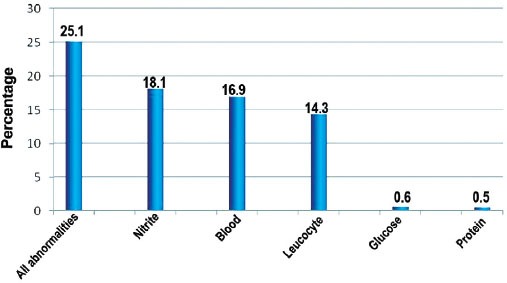
Frequency of dipstick examination of urine samples among screened children (N=1000).
Figure 2.
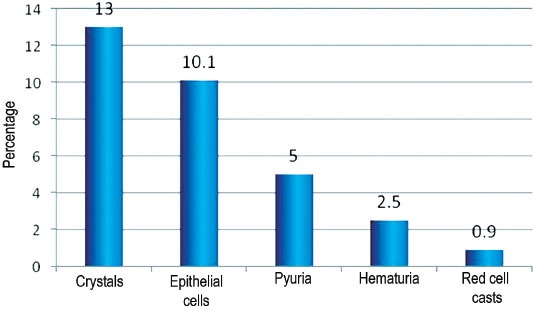
Microscopic examination of abnormal dipstick urine samples among the 251 cases positive by dipstick.
Figure 3.
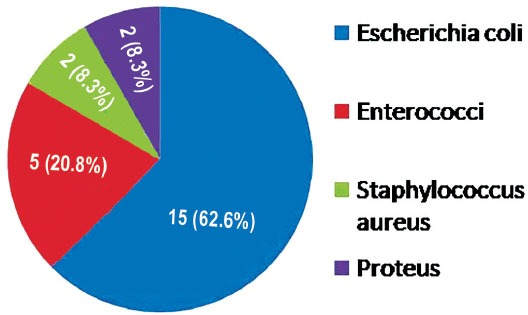
Distribution of bacteria in positive urine culture among 24 cases.
Discussion
In developing countries, the national epidemiologic data on chronic kidney disease in the pediatric population is currently limited.14 A cornerstone in evaluation of kidney function is the urine analysis, which is a simple and inexpensive test. Dipstick method is the most rapid screening procedure used in early detection of urinary tract diseases; thus, helping prevention and retarding progression to chronic renal failure.15
In our study, the dipstick urine analysis revealed that 25% of the screened children had urinary abnormality. Similarly, a high prevalence of urinary abnormality (up to 30%) among children has been reported by different authors in different regions all over the world.16,17 Proteinuria and hematuria are the most important laboratory signs of renal disease in children.13 Proteinuria is considered a strong independent risk factor of end stage renal disease. Thus, asymptomatic proteinuria warrants attention for early detection and management.18 The most important causes of hematuria in young age are renal stones, structural abnormalities of the urinary tract, or parenchymal renal diseases.19 In our study, dipstick-detected hematuria was encountered in 17% and proteinuria in 0.5% of the cases. Inversely, in a study conducted among Indian schoolchildren, the prevalence was 16% for proteinuria and 5% for hematuria.20 In agreement with our results, a survey conducted in Makkah among schoolchildren, revealed 14.75% of the screened children had hematuria.21 In concordance with these results, there is also a study on schoolchildren in Shanghai which reported a prevalence of 0.5% of children having proteinuria.22
Glucosuria and positive nitrite were another abnormality in our study; glucosuria was detected in 0.6% of children (no ketones detected in urine), and positive nitrate in 18.1%, which is similar to the studies carried out in Shiraz, Iran (glucosuria was 0.2% and positive nitrite was 18%).5 Detectable nitrite in urine has been used to diagnose urinary tract infection; a very common disorder in children.23
The presence of hematuria must be confirmed by microscopic examination of urine because other substances besides blood can produce red or brown urine or give a false positive dipstick test for blood.24 The development of asymptomatic microscopic hematuria is relatively common in children. Its prevalence in pre-school aged children is 0.5-2.0% depending on the population screened.15 This is comparable with our results that showed a prevalence of 2.5% (in the abstract section was 9.9%?. The most prevalent microscopic finding in our study was crystalluria, which was evident in 13% of children (in the Abstract was 51.8%?, please check). Crystalluria is a global reflection of the risk of stone formation and therefore, the physician should be alerted by this finding in urine analysis. Our results are in concordance with Arustamov and Nurullaev25 study who found that crystalluria among children aged between one and 5 years, was encountered in 17.3% of the cases. Escherichia coli is the most frequent organism isolated from subjects with asymptomatic bacteriuria.26 This fact is consistent with our findings where E. coli was the most common pathogen identified in culture, accounting for 62.6% of isolated organisms. Our study showed that gender had a significant impact on some results as for crystals and epithelial cells, which were more prevalent in females. However, this was not in concordance with the study carried out in Basra city in Iraq, regarding crystalluria, which found no significant difference between males and females.27
In conclusion, urinary abnormalities are common among apparently healthy children. We strongly recommend the implementation of a national screening program for urinary problems in childhood as an early way of detection that could mandate early intervention before a permanent or chronic renal or urinary tract damage takes place.
Acknowledgment
We gratefully acknowledge the support provided by Taif University, Taif, Saudi Arabia and the administration at the Children’s Hospital where the study was carried out.
Footnotes
Disclosure.
Related Articles.
Abdullah LS. The value of urine cytology in the diagnosis of bladder cancer. Cytopathological correlation. Saudi Med J 2013; 34: 937-941.
Per H, Canpolat M, Sahin U, Gumus H, Konuskan B, Kumandas S. Serum and urine boron and selenium levels in children with resistant epilepsy. Saudi Med J 2012; 33: 942-947.
Hussein HG, Ali HH. Value of the silver-stained nucleolar organizer regions technique in the differentiation between benign and malignant lesions in urine cytology. Saudi Med J 2009; 30: 719-721.
References
- 1.Gulati S, Gulati S, Finberg L, Windle ML, Kaskel FJ, Langman GB. Chronic Kidney Disease in Children. [Accessed: 2014 February]. Updated: 2012 September 28. Available from URL: http://emedicine.medscape.com/article/984358-overview .
- 2.Index Mundi. Saudi Arabia Demographics Profile. [Accessed: 2014 March]. Updated 2013. Available from URL: http://www.indexmundi.com/saudi_arabia/demographics_profile.html .
- 3.Kari JA. Pediatric renal diseases in the Kingdom of Saudi Arabia. World J Pediatr. 2012;8:217–221. doi: 10.1007/s12519-012-0360-6. [DOI] [PubMed] [Google Scholar]
- 4.Parakh P, Bhatta NK, Mishra OP, Shrestha P, Budhathoki S, Majhi S, et al. Urinary screening for detection of renal abnormalities in asymptomatic school children. Nephrourol Mon. 2012;4:551–555. doi: 10.5812/numonthly.3528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shajari A, Zadeh FMH, Shajari H. screening of renal diseases in the first primary school children in Shiraz. Acta Medica Iranica. 2007;45:215–218. [Google Scholar]
- 6.Clark WF, Macnab JJ, Sontrop JM, Jain AK, Moist L, Salvadori M, et al. Dipstick proteinuria as a screening strategy to identify rapid renal decline. J Am Soc Nephrol. 2011;22:1729–1736. doi: 10.1681/ASN.2010111217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Patel HP. The abnormal urinalysis. Pediatr Clin North Am. 2006;53:325–337. doi: 10.1016/j.pcl.2006.02.004. [DOI] [PubMed] [Google Scholar]
- 8.Hogg RJ. Screening for CKD in children: a global controversy. Clin J Am Soc Nephrol. 2009;4:509–515. doi: 10.2215/CJN.01210308. [DOI] [PubMed] [Google Scholar]
- 9.Akor F, Okolo S, Agaba E, Okolo A. Urine examination findings in apparently healthy new school entrants in Jos, Nigeria. South African Journal of Child Health. 2009;3:60–63. [Google Scholar]
- 10.Gansevoort RT, Bakker SJL, de Jong PE. Early detection of progressive chronic kidney disease: is it feasible? [comment] J Am Soc Nephrol. 2006;17:1218–1220. doi: 10.1681/ASN.2006030247. [DOI] [PubMed] [Google Scholar]
- 11.Tjale MC. Sovenga: South Africa: Polokwane Mankweng Hospital; 2009. The prevalence of abnormal urine components as detected by routine dipstick urinalysis: a survey at a primary health care clinic in Mankweng hospital [dissertation] [Google Scholar]
- 12.Whiting P, Westwood M, Watt I, Cooper J, Kleijnen J. Rapid tests and urine sampling techniques for the diagnosis of urinary tract infection (UTI) in children under five years: a systematic review. BMC Pediatrics. 2005;5:4. doi: 10.1186/1471-2431-5-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Leung AK, Wong AH. Proteinuria in children. Am Fam Physician. 2010;82:645–6451. [PubMed] [Google Scholar]
- 14.Gheissari A, Hemmatzadeh S, Merrikhi A, Fadaei Tehrani S, Madihi Y. Chronic kidney disease in children: A report from a tertiary care center over 11 years. J Nephropathology. 2012;1:177–182. doi: 10.5812/nephropathol.8119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hajar F, Taleb M, Aoun B, Shatila A. Dipstick urine analysis screening among asymptomatic school children. North Am J Med Sci. 2011;3:179–184. doi: 10.4297/najms.2011.3179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dang le NN, Doan Tle B, Doan NH, Pham TK, Smets F, Thi MH, et al. Epidemiological urinalysis of children from kindergartens of Can Gio, Ho Chi Minh City - Vietnam. BMC Pediatr. 2013;13:183. doi: 10.1186/1471-2431-13-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Akor F, Okolo SN, Agaba EI, Okolo A. Urine examination findings in apparently healthy new school entrants in Jos, Nigeria. South African J Child Health. 2010;3:60–63. [Google Scholar]
- 18.El-Tayeb M, El Setouhy M, El Sayed H, Elshahawy Y. Screening of proteinuria in young adults: Is it worthwhile? Dialysis & Transplantation. 2010;39:522–526. [Google Scholar]
- 19.Ashraf M, Parray NA, Malla RA, Rasool S, Ahmed K. Hematuria in children. Int J Clin Pediatr. 2013;2:51–60. [Google Scholar]
- 20.Patil PM, Hipparagi SB, Sinha KS, Sorangavi VM. Asymptomatic Proteinuria and Hematuria in School Going Children. Journal of Krishna Institute of Medical Sciences University. 2013;2:105–108. [Google Scholar]
- 21.Edrees B, Tayeb M, Shandeedi M. Prevalence of Hematuria among School Children in Makkah and Baha in Saudi Arabia. J Med J. 2013;47:20–25. [Google Scholar]
- 22.Rao J, Zhou L, Shen Q, Sun L, Fang XY, Liu HM, et al. School urinalysis screening in Shanghai. World J Pediatr. 2006;2:195–198. [Google Scholar]
- 23.White B. Diagnosis and treatment of urinary tract infection in children. Am Fam Physician. 2011;83:409–415. [PubMed] [Google Scholar]
- 24.Meyers KEC. Evaluation of hematuria in children. Urologic Clinics of North America. 2004;31:559–573. doi: 10.1016/j.ucl.2004.04.015. [DOI] [PubMed] [Google Scholar]
- 25.Arustamov D, Nurullaev R. Prevalence of the most significant urological diseases among the rural population of Uzbekistan. Urology [Urologiya], Russian. 2004;6:3–6. [PubMed] [Google Scholar]
- 26.Chukwu BF, Okafor HU, Ikefuna AN. Asymptomatic bacteriuria in children with sickle cell anemia at The University of Nigeria teaching hospital, Enugu, South East, Nigeria. Ital J Pediatr. 2011;37:45. doi: 10.1186/1824-7288-37-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hassan JK. Crystalluria types and incidence in Basra City;southern of Iraq. Journal of Basrah Researches (Sciences) 2011;37:5A. [Google Scholar]