

Abstract
Objectives:
To observe the frequency of breast cancer among Saudi patients and to highlight the age variations and features of advanced cancer.
Methods:
A retrospective study of breast cancer biopsies from all Saudi patients performed between January 2006 and December 2013 in King Fahad Hospital, Al-Madinah, Kingdom of Saudi Arabia. All the available demographic and tumor related data was analyzed.
Results:
Of 1005 breast tissues reviewed, 982 specimens were from female, and 23 from male patients. In females, 398 specimens (40.5%) were diagnosed as malignant. Invasive ductal carcinoma (IDC) (85.2%) was most common, followed by ductal carcinoma in situ (8%), and invasive lobular carcinoma (2.7%). The mean age of Saudi females with IDC was 46.9 years. Approximately 48.7% IDC were Grade III tumors. A tumor size >2.5 cm was found in 61.1% patients, whereas axillary nodal metastasis was present in 57.1% and lymphovascular invasion in 64.1% who underwent axillary nodal dissection. In males, 4 specimens (17.4%) were malignant (all IDC).
Conclusion:
Our finding are consistent with previous reports of breast cancer being diagnosed in younger age group, in advanced stages, and with features of aggressive behavior; which signals the urgency for implementation of breast screening programs.
Breast cancer (BC) is the second most common cancer in the world, and most frequent cancer among women with an estimated 1.67 million new cancer cases diagnosed in 2012 (25% of all cancers).1 As reported by GLOBOCAN,1 in both, the less developed (883,000 cases) and the more developed regions (794,000 cases), it is the most common cancer in women. The American Cancer Society estimated 232,340 new cases of invasive BC in women, and approximately 2,240 new cases among men in the US during 2013.2 In the United Kingdom (UK), BC mortality is however, the second to lung cancer, accounting for 11,684 deaths in 2011.3 In the Kingdom of Saudi Arabia (KSA), BC is most prevalent cancer in Saudi females as reported in Saudi Tumour Registry Report 2012.4 In 2008, previous study3 from Jeddah, KSA compared the cancer statistics for the KSA and USA; with the aim to study the future cancer burden in Saudi Arabia. They concluded that the cancer rates demonstrate a considerable increase and enormous demands on healthcare resources, in the future.5 Al Diab et al,6 reported 80 articles on BC from KSA. They concluded that it is most common in the Central region of KSA, and least common in the Northern region, with Eastern, Western, and Southern regions falling in the middle.6 In our present, hospital based, retrospective study, we cited and compared similar recent studies from around the world; such as from India,7,8 Nigeria,9 Pakistan,10 and Yemen.11 The KSA medical literature also has a number of similar relevant hospital based studies available for comparison.12-15 There is however, only one article in the local literature for hospital-based cancer data for Al-Madinah, which was carried out almost 20 years back.16 Although there has been some very recent hospital-based research publications from Al-Madinah; these articles have reported general disease patterns and cancers in many different organs such as large bowel,17,18 prostate,19 lymph nodes,20 and thyroid,21 but no data is available for this common and important disease, namely BC. We will be investigating this important problem of BC in the rapidly growing and advancing region of Al-Madinah; based on the histopathology diagnosis of biopsies and mastectomies/axillary dissections performed in the local population; and compare our data with previous international and national studies.
Methods
The study was mainly performed in the Histopathology Laboratory of King Fahad Hospital, Al-Madinah, Saudi Arabia, which is a tertiary care hospital of more than 500 beds, catering services to large population of Al-Madinah and surrounding region of Western Saudi Arabia. The catchment population includes the local Saudi population, expatriates, and pilgrims from around the world visiting the Holy city of Al-Madinah throughout the year. The present study was a retrospective study that analyzed the breast biopsy reports from the Histopathology Department of the King Fahad Hospital. All the breast biopsies records, reported between January 2006 and December 2013, were retrieved from the laboratory computer database. The basic demographic information was collected including age, gender, nationality, and final diagnosis of the biopsy. The inclusion criteria were the diagnosis of breast carcinomas (both invasive as well as in-situ) in Saudi patients of both gender and all age groups. The exclusion criteria were all non-Saudi patients (whether resident expatiates, visitors or pilgrims) as well as any cutaneous carcinoma of skin overlying the breast. Tumor related parameters were then collected such as laterality, multiplicity, size of lesion, diagnosis, and associated conditions. In case of surgical specimens, additional information included in the study were lymph node status (in cases of any associated axillary procedure), multicentricity, skin/nipple involvement, and any available history of recurrence. Patients with more than one specimen for the same lesion were counted once. Patients with multiple or bilateral similar lesions, even if excised at different times, were counted once. All these neoplastic lesions were classified on the basis of 2003 World Health Organization Classification of tumors of the breast.22
All the available data was entered into Microsoft Office 2007 Excel program. The calculations were performed utilizing the inbuilt functions of Microsoft 2007 Excel program. As the study was addressing basic demographic and pathological information, and no comparison was indicated between the parameters, no statistical analysis or any p-value calculation was performed. Moreover, as all the records were obtained from the histopathology laboratory, written permission was obtained from the head of department of the laboratory. Literature search was performed by utilizing the google search engine and PUBMED (National Library of Medicine, Bethesda, MO, USA).
Results
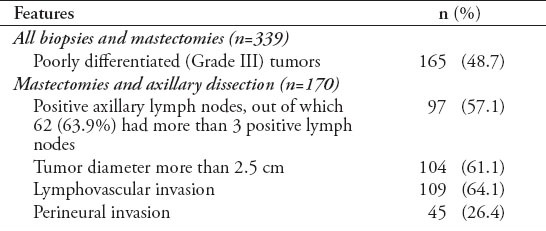
A total of 1005 breast cases were reported during the study period, out of which 982 were Saudi females and 23 were Saudi males, with a female to male ratio of 42.6:1. Of 982 breast tissues received from female patients, malignant lesions comprised 398 cases (40.5%). Most commonly reported was invasive ductal carcinoma accounting for 85.2% of malignant lesions, followed by ductal carcinoma in situ (8%). There were 11 cases of infiltrating lobular carcinoma (2.7%), and 3 cases of lobular carcinoma in situ (0.7%). All the malignant lesions in 398 females are summarized in Table 1. Out of 32 Saudi males, 4 cases were reported to have infiltrating ductal carcinoma. Table 2 provides the age distribution of most common types of BCs in both genders. The ages of patients with infiltrating ductal carcinoma (IDC) were distributed between 25-88 years. The peak age occurrence was in the fifth decade followed by the sixth decade. Seventy-four (21.8%) cases were seen below the age of 40 years and 79 (23.3%) cases were above the age of 60 years. Both breasts were equally affected in frequency by carcinoma; namely, involvement of the right breast in 163 (48%) cases, left breast in 166 (49%), and both breasts in 3 cases. In 7 cases, the side was not recorded. Sixty patients (17.7%) had tumor with grade I differentiation; 114 cases (33.6%) with grade II, and 165 cases (48.7%) with grade III differentiation. The ages of patients with ductal carcinoma in situ ranged from 26-112 years. The peak occurrence was in the sixth decade. Both the breasts were equally involved: the right breast in 15 cases (46.8%) and the left breast in 17 cases (53.2%). Infiltrating lobular carcinoma ranked third in this series. The ages of patients ranged from 40-70 years. The peak age occurrence was in the sixth decade. The right breast was involved in 5 cases (45.4%) and the left breast in 6 cases (54.6%). One hundred and seventy patients underwent mastectomy with axillary lymphadenectomy. The size of the tumor was less than 2.5 cm in only 66 cases (38.9%). Ten patients (5.9%) had more than one focus or nodule of tumor in the same breast. In 5 cases (1.5%), the tumor attained quite a large size and was associated with ulceration of the skin with formation of a fungating mass. Six patients showed clinical and histological evidence of nipple involvement (Paget disease), one associated with infiltrating lobular carcinoma, 2 associated with intraductal carcinoma and the rest involved with infiltrating ductal carcinoma. More than half of the patients who underwent axillary surgery had axillary lymph node metastasis; 62% of patients with metastasis had more than 3 positive lymph nodes. Similarly, almost two third of the patients who underwent mastectomy and axillary surgery had lymphovascular invasion. In contrast, perineural invasion was not seen in as high proportion of cases as the lymphovascular invasion. Table 3 summarizes all the features of advanced disease and aggressive behavior of our patients. It was clear from these findings that our patients with infiltrating carcinoma of the breast presented with a more advanced disease and that their tumor was biologically more aggressive as evidenced by the high frequency of poorly differentiated tumors.
Table 1.
Distribution of breast cancer in 398 Saudi females with mean age from Western Saudi Arabia (N=398).
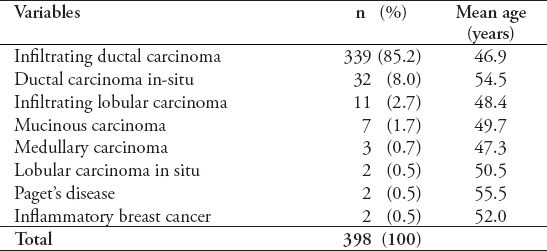
Table 2.
Age distribution of the most common types of breast cancer in both genders among 339 patients from Western Saudi Arabia.

Table 3.
Features of advanced disease and aggressive behavior in infiltrating ductal carcinoma among mastectomies and axillary dissection specimens (n=170).
Discussion
Our study from the region of Al-Madinah highlights the frequency, demographic data, and pathological features of BC based on biopsy experience at King Fahad Hospital, Al-Madinah. This study encompasses all malignant breast lesions reported by histopathologists, involving both genders, and all age groups of Saudi patients. Being a retrospective study, this present study has its limitation that important statistical analysis was not possible and we had to depend on the data collecting efficacy and performance of others; however, it serve the purpose of collecting basic data that can be compiled and compared with similar historical studies.
There are several similar relevant publications from KSA and abroad with which to compare our results. From the Al-Madinah region, there was only one previous study from 2 decades back, which analyzed patterns of all cancers diagnosed in the region, and did not specifically address BC.16 Thus, our study provides important baseline data for BC, and allows us to compare with results of other studies from within and outside KSA.
In our present study, there was a total of 982 female patients out of which, 398 (40.5%) were diagnosed to have malignant lesions. Infiltrating ductal carcinoma and ductal carcinoma in situ accounted for most malignancies. In a recent review of BC in KSA, Al Diab et al,6 concluded that the frequency percentage of BC varied from a lowest percentage of 8.6% in the Northern region, to a highest percentage of 34.2% in the Central region. Comparing our data with other recent studies, we found that there were much lower BC percentages reported; for example 11.8% from Pakistan;10 21.4% from Hofuf, Al Hassa, KSA,14 22.4% from South Yemen,11 and 22.3% from India.7 In the previous study of cancers in Al-Madinah 20 years earlier, the percentage of BC reported in 2237 cases was only 8.5%.16 Two studies from KSA12,15 reported a higher percentage of BC, which is close to our findings. Jamal et al15 from Jeddah, KSA reported 32.5% BC in >1000 breast lesions, whereas Al-Rikabi and Husain12 quoted the figures of 34.2% for BC in the whole study group (both genders), and 35.8% within the female group. The frequency percentage of BC in our study is even higher (398 [40.5%] malignant diagnosis in 982 females) than the previous report from the Central region (34.2%) of KSA as analyzed by Al Diab et al.6 Al Diab et al6 commented that data from all regions of KSA were not available for comparison with their study and Al-Madinah was one of the regions, which not previously been studied for BC frequency percentages.
In our study, the mean age of patients with BC is 46.9 years, and most were younger than 50 years. The peak age incidence for malignant breast disease was 31-40 years in the study from Lagos, Nigeria.9 Bafakeer et al,11 reported that BC was common in the 40-49 age group in South Yemen. Al-Rikabi and Husain,12 from Central KSA reported the mean age of onset for BC was 48.6 years. Similar observations were reported by Rudat et al,13 from Eastern KSA that BC patients were diagnosed at a markedly younger age (<50 years); they reported 57.5% young BC patients from Eastern KSA compared with 12.5% from the USA. In 2010, Najjar and Easson23 carried out a comprehensive literature review from Arab countries; and concluded that BC is being diagnosed a decade earlier at an average age of 48 years, and one third of patients were younger than 50 years. All these findings are endorsed by an epidemiological study by Alghamdi et al,24 who concluded that in KSA, BC is diagnosed in a significantly younger age group (38.6% in age group of 30-44, and 31.2% in 45-59 years). Our study results are in line with the regional and national reports that BC is being diagnosed at an earlier age than the western population.
In the present study, the most commonly reported subtype of BC was IDC, followed by ductal carcinoma in situ (DCIS) with more than 93% of cases. The remaining subtypes of BC comprised only a minority of cases. Within this small group, invasive lobular carcinoma was the most common malignant lesion. Comparing these findings with other studies, we found that all cases from a Pakistan study were IDC.10 Whereas from within KSA, Al-Rikabi and Husain,12 from Central KSA reported 96.1% IDC, followed by a small group containing malignant phylloides, medullary, mucinous/colloid, and inflammatory carcinomata. Amin et al,14 from the Eastern town of Al Hassa, KSA reported 78.7% IDC, and 1.9% DCIS, followed by infiltrating lobular carcinoma in 7.7%. There were also some cases of combined lobular and ductal carcinoma in their observations. Jamal15 from Jeddah (Western region) reported 88% IDC and 4.5% lobular carcinoma. Our results regarding the subtypes of BC are in conformity with that of national studies.
Summarizing the available tumor parameters in our study, almost half were a high grade (Grade III), greater than 2.5 cm and/or had positive lymph nodes. Most had lymphovascular invasion. The findings of advanced BC at the time of diagnosis has also been reported from within the country. There were 2 recent studies on advanced BC, both from the Eastern region of KSA. Firstly, Rudat et al,13 from Al-Khobar analyzed and compared 262 female patients diagnosed with BC to the published American data and concluded that localized disease was found in only 28.6% of their cases as compared with 61.2% localized disease in American patients derived from SEER database.13 Secondly, Amin et al14 from Al Hassa reported 969 cases, out of which 69.1% were of a higher grade with lymph nodes metastasis. Our results are in keeping with the above studies; and we conclude that BC presents in aggressive and advanced stages in the local population.
During the study period, 23 male specimens were reported out of which, 4 (17.4%) were IDC. Similarly, a study from Jeddah, Western KSA, reported 13% malignant lesions (75% IDC and 25% metastasis).15 Our findings from the male patients were consistent with the results of the available studies carried out in KSA, that the predominant diagnosis of BC in males is IDC.
In conclusion, we report the highest frequency of BC diagnosis in our region comparing with other regions from KSA, even higher than previously highest figure from the Central KSA. The present study results are in line with the cancer diagnosis being made in younger age group, in advanced stages, with features of aggressive behavior. The results of this present study are highly important, as these results provide baseline data of BC in the Al-Madinah region; thus, contributing to future epidemiological and hospital-based researches. We recommend further epidemiological studies along with educational campaigns and screening programs to address the increasing BC problem in the region.
Footnotes
Disclosure.
References
- 1.Geneva (CH): World Health Organization; 2012. World Health Organization. GLOBOCAN 2012. Estimated incidence, mortality and prevalence worldwide in 2012. [Google Scholar]
- 2.Atlanta (GA): American Cancer Society; 2013. American Cancer Society. Cancer Facts & Figures 2013; pp. 1–64. [Google Scholar]
- 3.Cancer Research. Cancer Statistics Report. Cancer Mortality in the UK in 2011. [Accessed 2013 December 14]. Updated 2013 November. Available from URL: http://www.cancerresearchuk.org/cancer-info/cancerstats .
- 4.Tumour Registry Annual Report 2012. King Faisal Specialist Hospital and Research Centre. [Accessed 2014 January 8]. Updated 2013 November. Available from URL: http://www.kfshrc.edu.sa/oncology/2012_Tumor_Registry_Annual_Report.pdf .
- 5.Ibrahim EM, Zeeneldin AA, Sadiq BB, Ezzat AA. The present and the future of breast cancer burden in the Kingdom of Saudi Arabia. Med Oncol. 2008;25:387–393. doi: 10.1007/s12032-008-9051-5. [DOI] [PubMed] [Google Scholar]
- 6.Al Diab A, Qureshi S, Al Saleh KA, Al Qahtani AH, Aleem A, Algamdi MA, et al. Review on breast cancer in the Kingdom of Saudi Arabia. Middle-East J Sci Res. 2013;14:532–543. [Google Scholar]
- 7.Bag A, Rawat S, Pant NK, Jyala NS, Singh A, Pandey KC. Cancer patterns in Nainital and adjoining districts of Uttarakhand: A one year survey. J Nat Sci Biol Med. 2012;3:186–188. doi: 10.4103/0976-9668.101911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Maiti PK, Jana U, Ray A, Karmakar R, Mitra TN, Ganguly S. Patterns of cancer occurrence in different regions of West Bengal--a hospital based study. J Indian Med Assoc. 2012;110:445–448. [PubMed] [Google Scholar]
- 9.Jeje EA, Mofikoya BO, Oku YE. Pattern of breast masses in Lagos: a private health facility review of 189 consecutive patients. Nig Q J Hosp Med. 2010;20:38–41. doi: 10.4314/nqjhm.v20i1.58015. [DOI] [PubMed] [Google Scholar]
- 10.Aslam HM, Saleem S, Shaikh HA, Shahid N, Mughal A, Umah R. Clinico-pathological profile of patients with breast diseases. Diagn Pathol. 2013;8:77. doi: 10.1186/1746-1596-8-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bafakeer SS, Banafa NS, Aram FO. Breast diseases in Southern Yemen. Saudi Med J. 2010;31:1011–1014. [PubMed] [Google Scholar]
- 12.Al-Rikabi A, Husain S. Increasing prevalence of breast cancer among Saudi patients attending a tertiary referral hospital: a retrospective epidemiologic study. Croat Med J. 2012;53:239–243. doi: 10.3325/cmj.2012.53.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rudat V, Brune-Erbe I, Noureldin A, Bushnag Z, Almuraikhi N, Altuwaijri S. Epidemiology of breast cancer patients at a tertiary care center in the Eastern Province of Saudi Arabia. Gulf J Oncolog. 2012;11:45–49. [PubMed] [Google Scholar]
- 14.Amin TT, Al-Mulhim AR, Chopra R. Histopathological patterns of female breast lesions at secondary level care in Saudi Arabia. Asian Pac J Cancer Prev. 2009;10:1121–1126. [PubMed] [Google Scholar]
- 15.Jamal AA. Pattern of breast diseases in a teaching hospital in Jeddah, Saudi Arabia. Saudi Med J. 2001;22:110–113. [PubMed] [Google Scholar]
- 16.Al Saigh AA, Allam MM, Khan KA, Al Hawsawi ZM. Pattern of cancer in Madina Al-Munawara region. Ann Saudi Med. 1995;15:350–353. doi: 10.5144/0256-4947.1995.350. [DOI] [PubMed] [Google Scholar]
- 17.Albasri A, Yosef H, Hussainy A, Bukhari S, Alhujaily A. Profile of colorectal polyps: a retrospective study from King Fahad Hospital, Madinah, Saudi Arabia. Asian Pac J Cancer Prev. 2014;15:2669–2673. doi: 10.7314/apjcp.2014.15.6.2669. [DOI] [PubMed] [Google Scholar]
- 18.Albasri A, Yosef H, Hussainy AS, Sultan SA, Alhujaily A. Histopathological features of colorectal cancer in Al-Madinah region of Saudi Arabia: 8 years experience. Asian Pac J Cancer Prev. 2014;15:3133–3137. doi: 10.7314/apjcp.2014.15.7.3133. [DOI] [PubMed] [Google Scholar]
- 19.Albasri A, El-Siddig A, Hussainy A, Mahrous M, Alhosaini AA, Alhujaily A. Histopathologic characterization of prostate diseases in Madinah, Saudi Arabia. Asian Pac J Cancer Prev. 2014;15:4175–4179. doi: 10.7314/apjcp.2014.15.10.4175. [DOI] [PubMed] [Google Scholar]
- 20.Albasri AM, El-Siddig AA, Hussainy AS, Alhujaily AS. Pattern of lymph node pathology in western Saudi Arabia. Asian Pac J Cancer Prev. 2014;15:4677–4681. doi: 10.7314/apjcp.2014.15.11.4677. [DOI] [PubMed] [Google Scholar]
- 21.Albasri A, Sawaf Z, Hussainy AS, Alhujaily A. Histopathological patterns of thyroid disease in Al-Madinah region of Saudi Arabia. Asian Pac J Cancer Prev. 2014;15:5565–5570. doi: 10.7314/apjcp.2014.15.14.5565. [DOI] [PubMed] [Google Scholar]
- 22.Tavassoli FA, Devilee P. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. Lyon (FR): IARC Press; 2003. World Health Organization Classification of Tumours. [Google Scholar]
- 23.Najjar H, Easson A. Age at diagnosis of breast cancer in Arab nations. Int J Surg. 2010;8:448–452. doi: 10.1016/j.ijsu.2010.05.012. [DOI] [PubMed] [Google Scholar]
- 24.Alghamdi IG, Hussain II, Alghamdi MS, El-Sheemy MA. The incidence rate of female breast cancer in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001-2008. Breast Cancer (Dove Med Press) 2013;5:103–109. doi: 10.2147/BCTT.S50750. [DOI] [PMC free article] [PubMed] [Google Scholar]