

Abstract
The aim of study was to investigate the effect of postoperative gum chewing on the recovery of bowel function after cesarean section. Total 100 women delivered by lower uterine segment section cesarean under local anesthesia (spinal). Eligible patients were randomly allocated into two groups: a gum-chewing group (n=50) or a control group (n= 50). The gum-chewing group participants who received one stick of sugarless gum for one hours, three times daily immediately after recovery from anesthesia and the control group had the usual postoperative care until being discharged. All women were followed up regularly until discharge from hospital, and recorded the times to the first bowel sounds of normal intestinal sounds, the time to the first passage of flatus, the time to the first feeling of hunger, and the time to the first defecation. The operative data, postoperative tolerance of gum chewing, and postoperative complications were documented. There was no statistically significant difference between the two groups in terms of demographic characteristics such as age, body mass index, parity, duration of surgery, number of miscarriages and curettages, time to the first feeding, the amount of serum intake, and type of cesarean section. The mean average postoperative interval of the first bowel sounds (21.9 versus 26.1 hours, p= 0.016), the first feeling of hunger (11.8 versus 14.5 hours, p= 0.050), the first passage of flatus (24.8 versus 30.0 hours, P=0.002), the first defecation (30.6 versus 38.4 hours, P= 0.0001) was significantly shorter compared to the control group.
Keywords: gum chewing, ileus, cesarean section, postoperative, early oral feeding
INTRODUCTION
Cesarean section is the most common surgery among women which is associated with central nervous system (CNS) changes in postoperative, leading to decreased bowel movements and driven problems among women (1). Postoperative ileus is defined as transient cessation of coordinated bowel motility after surgical intervention (2), and is one of the major problems of post-abdominal surgery along with delays hospital discharge, abdominal pain, abdominal distension, inability to start oral feeding and, breastfeeding, and eventually increases the cost of hospital care (3). The pathogenesis of postoperative ileus is multifactorial, but it is more common in cases of preoperative narcotic and drug interaction and abdominal surgery procedures, especially intraoperative bowel manipulation, and temporarily contributes to stop peristaltic (bowel movement); the related mechanism is probably dysfunction in parasympathetic system activity (inhibitory neurons) (4). Historically, professionals of gynecology and obstetrics waited until gut function returns allowing oral or entered feeding, characterized by symptoms such as bowel sounds, first flatus or stool, and feeling of hunger (5). When the first passage flatus or stool is noted it is not an initial return of bowel function. Studies have demonstrated that early postoperative feeding can be safe prior to the return of flatus or stool (6). However, some investigators reported that early feeding was associated with a high rate of intolerance and such as delayed feeding might even lead to increased cell breakdown, delayed wound healing, elevated risk of infection and the need for more intravenous feeding, and eventually additional costs on healthcare system as well as the family (7, 8). Chewing gum can bring on a feel faint because it stimulate the stomach, enhances gastric secretion, increases peristaltic bowel movements and finally hastens recovery from ileus (9-12). It has also been recently considered by researchers as a strategy toward ileus reduction. In some studies, beneficial effect of chewing gum has been approved in the resumption of bowel function (13-15), but in some others such as Quah et al., (16) contradictory findings have been achieved for the effects of gum chewing on peristaltic movements and digestive system stimulation. It seems that a necessity is felt for more investigation on such a least-expensive physiological method in stimulating the return of bowel function. Therefore, the aim of the present study was to evaluate the effect of chewing gum on the recovery of bowel function after cesarean section in women.
MATERIALS AND METHODS
This study was approved by Babol University of Medical Sciences for ethics in medical research. A single blind randomized controlled clinical trial was conducted on 100 women candidates for cesarean section with local anesthesia (spinal) in gynecology ward of Hospital during June 2010 to March 2011. The nature of the study did not allow blinding after assignment of the intervention postoperatively. Written informed consent was obtained from 110 enrolled women. All enrolled women were allocated using a computer-generated random sequence from a statistics program. All cesarean section were carried out by a Gynecologic Surgeon (an author) in the morning. A transverse incision on the uterus and a Pfannenstiel incision on the abdomen were performed. Demographic information on all variables women included; patient’s age, body mass index, number of pregnancies, miscarriage and uterine curettages. Exclusion criteria were: women with history of drug consumption, especially opioids, water and electrolyte disturbances, pancreatitis or peritonitis, history of abdominal surgery except cesarean section, no willingness to cooperate, intra- and sever postoperative complications, inability to chew gum, withdrawal, diabetes, pre-eclampsia, prolonged rupture of membranes, hypothyroidism, and muscular and neurological disorders. The operative data were recorded, including the presence of severe adhesions, the occurrence of intraoperative complications, estimated blood loss and duration of surgery. Data-collection instruments included the interview form, questionnaires, and subjects’ examination. For each of the study participants, a questionnaire, designed based on characteristics and the research objective. The women in the chewing gum group chewed sugar-free gum for at least one hour, three times daily from six hours after surgery (after recovery from anesthesia) until being discharged. Commercially available sugar-free gum (Wrigley Company, Poland) was used in this study. The oral intake of clear fluids and soft foods was initiated on postoperative day. Only after documentation of bowel function, which they was determined with the presence of any two of the following three criteria: (1) bowel sounds; (2) flatus; and (3) felling of hunger. In order to reduce the effects of other variables, the postoperative feeding regime was standardized for the all women. Around 48 hours following operation, the women were discharged when they had stable vital signs with no febrile morbidity for at least 24 hours, ability to ambulate and urinate independently, defecation, ability to tolerate solid food and absence of sever other post surgery complications. For post-operative analgesia, 100 mg rectal sodium suppository diclofenac was routinely given three times daily. All women were followed up regularly until discharge from hospital, and recorded the times to the first bowel sounds of normal intestinal sounds, the time to the first passage of flatus, the time to the first feeling of hunger, and the time to the first defecation. Also, postoperative tolerance of gum chewing and postoperative complications was documented. However, any side effects, and unresolved postoperative complication presented by the women during the postoperative period were to be recorded. Before intervention, 10 enrolled women were excluded due to considered by surgeon to be inappropriate for this study. All analyses were performed with SPSS (version16.0). The data were analyzed by t test and chi square. A p value of 0.05 or less was considered statistically significant.
RESULTS
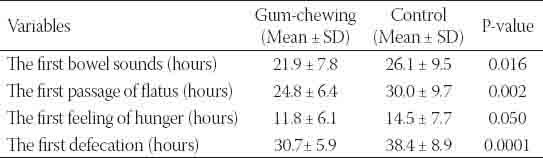
There was no statistically significant difference between the two groups in terms of demographic characteristics such as age, body mass index, parity, duration of surgery, number of miscarriages and curettages, time to the first feeding, the amount of serum intake, and type of cesarean section (Table 1). In gum-chewing group, the first bowel sounds was significantly shorter compared to the control group (p=0.016). The first defecation was 30.7 hours in the gum group and 38.4 hours in the control group (p=0.000). The first passage of flatus was seen on postoperative hours 24.8 in gum chewing group and on hours 30.0 in the control group respectively (p=0.002), and also the first feeling of hunger were felt on postoperative hours 11.8 in the gum-chewing group and 14.5 hours in the control group (p=0.050). None of the participants felt dissatisfied with chewing gum and none were excluded from the study (Table 2).
TABLE 1.
Participants’ characteristics based on the study groups (n=100)

TABLE 2.
Resumption of bowel function following the operation in both groups (n=100)
DISCUSSION
The women were well tolerating the gum and no feeling of dissatisfaction, and none were therefore excluded from the study. The study findings has shown reduced time to the first bowel sounds, defecation, passage of flatus, and feeling of hunger following chewing gum after the cesarean section. In this study, the mean time to the first bowel movement revealed remarkable difference between the two groups, which is in accordance with Dehcheshmeh study on the effects of chewing gum after elective cesarean section on 120 primiparous women in Shahrekord in 2011, reporting 7.4±1.71 hours and 15.7± 3.44 hours as the mean time to the first bowel movement in the gum and the control group respectively (2, 7, 17); the finding is also in consistent with Schuster study on the impact of gum chewing after sigmoid-colostomy surgery on 34 patients in 2006, in which the mean time to the first bowel movement was 63.2±5.4 hours and 89.4±2.4 hours in the gum and the control group (10). Nonetheless, in Akhlaghi survey on the effect of chewing gum on the resumption of bowel function after cesarean section on 120 patients in Mashhad in 2008, the two groups were different in terms of the feeling of bowel movement, but not statistically significant, as the mean difference was 14.7±6.5 hours and 16.6±8.4 hours in gum-chewing and the control group respectively. This study is not in agreement with the present research, and the reason behind such a contradiction may be due to sampling and/or surgical conditions (3). Other variable examined in terms of bowel function was the feeling of hunger which was 3 hours earlier in the chewing gum group than the other and was statistically significant; this finding is in consensus with Satij results following the caesarean section in 2006 (15); however, in Schuster study, the two groups were different on the feeling of hunger, but not statistically significant, as the mean time to the feeling of hunger was 63.5±10.4 hours and 72.8±31.1 hours in the chewing gum and the control group respectively (10); such a discrepancy could be owing to the small sample size in Schuster study. In the present research, the mean time to the first defecation displayed significant difference between the two groups as it happened 8 hours earlier in the gum than the control group, similar to the results obtained by Maeboud, Ghafouri, Hirayama, Hocevar and Abdollahi (1, 2, 14, 18, 19). So as, in Maeboud study on 200 patients after elective caesarean section in Egypt in 2010, the mean time of defecation was 21.1±4.7 hours and 30.00±8.2 hours earlier in gum-chewing and the control group, and in Hirayamai and Ghafouri studies, respectively on 50 patients with upper gastrointestinal tract surgery in 2008 in Tehran and colorectal surgery on 22 patients in 2006 in Japan, defecation time was 15 hours earlier in gum-chewing than the control in both studies, which was statistically meaningful. In Abdollah investigation on 46 patients following appendectomy surgery in Gorgan in 2011, the time to the first defecation was 24 hours earlier in the gum than the control group and was statistically significant. However, in a research on 38 patients after left colon cancer surgery in England in 2006, no statistical difference was observed in the time to the first defecation between the gum (3.2±1.5 hours) and the control (3.9±1.5 hours) group (16), about which small sample size and type of surgery may be the reasons for such a difference. The mean passage of flatus was the other variable evaluated on intestinal function, happening, on average, 5 hours earlier in the gum than the control group; this finding is in consistence with Kouba investigation on 102 patients undergoing bladder radical surgery in 2007 in America, in which the time to the first passage of flatus was respectively 2.4 and 2.9 days in the gum and the control group, showing acceleration of gas passage following chewing gum after bladder surgery (20). In Ngowe study in 2010 on 46 patients with open appendectomy, the mean time of gas passage was 2.2 and 3.0 days in the gum and the control group (21). In Choi survey on 60 patients in 2011, the mean time to the passage of flatus was 60 h and 48 hours in gum-chewing and the control group and statistically significant (22); whilst, Quah reported no remarkable difference between the two groups in terms of gas passage. There is not yet an independent investigation on the exact chewing gum mechanism of action. However, some theories discuss gum as a form of sham feeding that chewing resulting in propulsive gastrointestinal activity through cephalic-vagal stimulation (23, 24). It is suggested that cephalic-vagal mechanism being less effective in women undergoing cesarean section under local anesthesia (25). In addition, sugar free chewing gum that contains the artificial sweetener sorbitol and other hexitols might be having side effects such as bloating, gas, and abdominal cramps. However there is no reported about the possible effects of the ingredients of these gums (26). Moreover, in this study was found sugar free chewing gum safe and tolerated by all patients. Therefore, it is suggested that the content of maxitols in ‘sugar-free’ chewing gums may play a role in the amelioration of ileus after surgery and future studies are needed to investigate probable mechanisms involved in the observed phenomena.
CONCLUSION
The results of the present study indicate that chewing is acceptable and inexpensive physiologic method for decreasing the time to the passage of flatus, bowel movements, and feeling of hunger in patients undergoing cesarean section. It can be added to post-caesarean care without any concern on early post-operation feeding as a low-cost, safe and tolerable treatment in early intestinal stimulation to reduce ileus associated complications.
ACKNOWLEDGMENTS
The present study is a research project, Contract No.8827921 and IRCT registration No. 201008093902N2, approved by Babol University of Medical Sciences; hereby, the authors would like to appreciate the university authorities, and Ms. Shokat Asghari, and also respected personnel of the surgical ward of Rouhani Hospital of Babol for their sincere cooperation.
DECLARATION OF INTEREST
The authors declare that there is no conflicting interest.
REFERENCES
- [1].Hirayama I, Suzuki M, Ide M, Asao T, Kuwano H. Gum-chewing stimulates bowel motility after surgery for colorectal cancer. Hepatogastroenterology. 2006;53(68):206–8. [PubMed] [Google Scholar]
- [2].Ghafouri A, Soroush AR, Moini N, Hedayat A, Khorgami Zh. The efficacy of sugar free gum chewing after upper GI tract operation on ileus: a clinical trial IJSurgery. 2008;16(1):79–85. Farsi. [Google Scholar]
- [3].Akhlaghi F, Pourjavad M, Mansouri A, Tara F, Vahedian M. Effect of gum chewing on prevention of post cesarean ileus Hayat. 2008;14(2):35–40. Farsi. [Google Scholar]
- [4].Johnson MD, Walsh RM. Current therapies to shorten postoperative ileus. Cleve Clin J Med. 2009;76(11):641–8. doi: 10.3949/ccjm.76a.09051. [DOI] [PubMed] [Google Scholar]
- [5].Yaghmaei M, Arbabi FK, Mokhtari M, Behzadian A. Comparison of oral intake profiles at 2 and 8 hours following cesarean section under spinal anesthesia. JRMS. 2009;11(4):43–51. Farsi. [Google Scholar]
- [6].Pearl ML, Frandina M, Mahler L, Valea FA, DiSilvestro PA, Chalas E. A randomized controlled trial of a regular diet as the first meal in gynecologic oncology patients undergoing intraabdominal surgery. Obstet Gynecol. 2002;100(2):230–4. doi: 10.1016/s0029-7844(02)02067-7. [DOI] [PubMed] [Google Scholar]
- [7].Dehcheshmeh DF, Salehian T, Gangi F, Beigi M. The effect of chewing sugar free gum after elective cesarean-delivery on return of bowel function in primiparous women. QJRMS. 2011;4(4):16–20. Farsi. [Google Scholar]
- [8].Han-Geurts IJ, Jeekel J, Tilanus HW, Brouwer KJ. Randomized clinical trial of patient-controlled versus fixed regimen feeding after elective abdominal surgery. Br J Surg. 2001;88(12):1578–82. doi: 10.1046/j.0007-1323.2001.01934.x. [DOI] [PubMed] [Google Scholar]
- [9].Soffer EE, Adrian TE. Effect of meal composition and sham feeding on duodenojejunal motility in humans. Dig Dis Sci. 1992;37(7):1009–14. doi: 10.1007/BF01300279. [DOI] [PubMed] [Google Scholar]
- [10].Schuster R, Grewal N, Greaney GC, Waxman K. Gum chewing reduces ileus after elective open sigmoid colectomy. Arch Surg. 2006;141(2):174–6. doi: 10.1001/archsurg.141.2.174. [DOI] [PubMed] [Google Scholar]
- [11].Chewing gum for postoperative ileus (Protocol). Cochrane Database of Systematic Reviews 2007 [database on the Internet] 2007. doi/10.1002/14651858.CD006506/abstract. Available from: http://onlinelibrary.wiley.com/
- [12].Hitti M. Chewing gum may shorten hospital stays after colon surgery. Feb. 21. 2006. [cited January 25 2012]. Available from: http://www.webmd.com/colorectal-cancer/news/20060221/gum-may-aid-colon-surgery-recovery .
- [13].Yazdi K, Abdollahi AA, Behnampour N, Niazi M, Arya B, Azadrah M. Effect of chewing gum on the bowel motility after cholecystectomy. ZJRMS. 2011;13(3):65–9. Farsi. [Google Scholar]
- [14].Abd-El-Maeboud KH, Ibrahim MI, Shalaby DA, Fikry MF. Gum chewing stimulates early return of bowel motility after caesarean section. Bjog. 2009;116(10):1334–9. doi: 10.1111/j.1471-0528.2009.02225.x. [DOI] [PubMed] [Google Scholar]
- [15].Satij B, Cohen SA. Evaluation of Gum Chewing on the Return of Bowel Function in Cesarean-Delivery Patients. Obstetrics & Gynecology. 2006;107(4):10S. [Google Scholar]
- [16].Quah HM, Samad A, Neathey AJ, Hay DJ, Maw A. Does gum chewing reduce postoperative ileus following open colectomy for left-sided colon and rectal cancer? A prospective randomized controlled trial. Colorectal Dis. 2006;8(1):64–70. doi: 10.1111/j.1463-1318.2005.00884.x. [DOI] [PubMed] [Google Scholar]
- [17].Shang H, Yang Y, Tong X, Zhang L, Fang A, Hong L. Gum chewing slightly enhances early recovery from postoperative ileus after cesarean section: results of a prospective, randomized, controlled trial. Am J Perinatol. 2010;27(5):387–91. doi: 10.1055/s-0029-1243313. [DOI] [PubMed] [Google Scholar]
- [18].Hocevar BJ, Robinson B, Gray M. Does Chewing Gum Shorten the Duration of Postoperative Ileus in Patients Undergoing Abdominal Surgery and Creation of a Stoma? Journal of Wound Ostomy & Continence Nursing. 2010;37(2):140–6. doi: 10.1097/WON.0b013e3181d0b92b. 10.1097/WON.0b013e3181d0b92b. [DOI] [PubMed] [Google Scholar]
- [19].Abdollahi AA, yazdi k, Behnampur N, Neyaze M. The effect of chewing gum on bowel movements after appendectomy. Arak University of Medical Sciences Journal. 2011;13(4):38–43. [Google Scholar]
- [20].Kouba EJ, Wallen EM, Pruthi RS. Gum chewing stimulates bowel motility in patients undergoing radical cystectomy with urinary diversion. Urology. 2007;70(6):1053–6. doi: 10.1016/j.urology.2007.07.048. [DOI] [PubMed] [Google Scholar]
- [21].Ngowe MN, Eyenga VC, Kengne BH, Bahebeck J, Sosso AM. Chewing gum reduces postoperative ileus after open appendectomy. Acta Chir Belg. 2010;110(2):195–9. doi: 10.1080/00015458.2010.11680596. [DOI] [PubMed] [Google Scholar]
- [22].Choi H, Kang SH, Yoon DK, Kang SG, Ko HY, Moon du G, et al. Chewing gum has a stimulatory effect on bowel motility in patients after open or robotic radical cystectomy for bladder cancer: a prospective randomized comparative study. Urology. 2011;77(4):884–90. doi: 10.1016/j.urology.2010.06.042. [DOI] [PubMed] [Google Scholar]
- [23].Vasquez W, Hernandez AV, Garcia-Sabrido JL. Is gum chewing useful for ileus after elective colorectal surgery? A systematic review and meta-analysis of randomized clinical trials. J Gastrointest Surg. 2009;13(4):649–56. doi: 10.1007/s11605-008-0756-8. [DOI] [PubMed] [Google Scholar]
- [24].Byrne H. Gum chewing stimulates early return of bowel motility after caesarean section. Bjog. 2010;117(1):117. doi: 10.1111/j.1471-0528.2009.02418.x. author reply -8. [DOI] [PubMed] [Google Scholar]
- [25].Niloff PH. Does gum chewing ameliorate postoperative ileus? Results of a prospective randomized, placebo-controlled trial. J Am Coll Surg. 2006;203(3):405. doi: 10.1016/j.jamcollsurg.2006.06.006. [DOI] [PubMed] [Google Scholar]
- [26].Tandeter H. Hypothesis: hexitols in chewing gum may play a role in reducing postoperative ileus. Med Hypotheses. 2009;72(1):39–40. doi: 10.1016/j.mehy.2008.06.044. [DOI] [PubMed] [Google Scholar]