

Abstract
Hypertension is chronic disease with high prevalence, which can successfully be treated with antihypertensive drugs. Previous researches have shown that existing hypertension treatment guidelines are not fully implemented in practice. We have analysed antihypertensive drug utilization in Canton Sarajevo during five-year period (2004-2008). Research findings are discussed in relation to expected drug utilization according to Canton Sarajevo treatment guidelines. Objective of this research is to examine prescription patterns of antihypertensive drugs in primary health care in Canton Sarajevo during five-year period. Based on study findings we did an estimation of adherence to local treatment guidelines, which are similar to those published globally. Drug utilization data were collected from the largest pharmacy (retail) chain, representing more than 80% of pharmacies in Canton Sarajevo. Following drug groups have been analyzed: diuretics, beta-blockers, calcium- channel-blockers, ACE-Inhibitors (plain and combinations), Angiotensin-II-antagonists and alpha-blockers. Drug utilization is expressed in number of defined daily dose (DDDs), defined daily dose per thousand inhabitants per day (DDD/TID), drug utilization 90% (DU90%) and value in euros. ACE-Inhibitors are most prescribed drug class; combination of ACE-Inhibitors and diuretics account 46% of total antihypertensive budget spending. ACEIs are followed by calcium-channel-blockers. Diuretics utilization is decreasing from 2006 and being replaced with beta-blockers. Diuretics, recommended as first line therapy, are ranked as third in total antihypertensive drug utilization. It is necessary to introduce follow-up and enforce adherence to developed treatment guideline. Drug utilization studies can be used as tool for assessment of treatment guidelines adherence in primary health care.
KEY WORDS: pharmacoeconomics, antihypertensives, antihypertensives utilization, treatment guidelines, pharmaceutical expenditure
INTRODUCTION
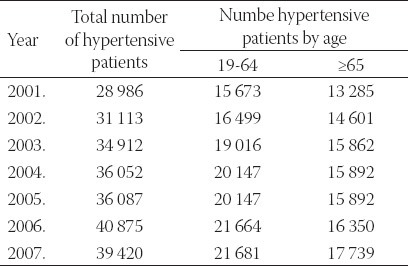
Hypertension as worldwide recognized public health problem is one of the leading causes of death influenced by cardiovascular diseases (CVD) like hart failure (HF), coronary heart disease (CHD), myocardial infarction (MI) and stroke. According to World Health Organization (WHO) and International Society of Hypertension (ISH) from 2003 it is estimated that hypertension cause 4.5% of global disease burden and is a prevalent in many developing countries as in the developed world. Hypertension related complication deaths are one third of global mortality cases [1]. WHO estimates that number of diagnosed will increase for 60% in next few years [2]. It is estimated that 11% of hypertensive patients are not diagnosed in developed countries while in developing countries including Bosnia and Herzegovina, that percentage is much higher up to 60% [3]. Canton Sarajevo is one of economically leading cantons with average net income of 450 EUR [4,5]. Table 1 shows number of inhabitants in Canton Sarajevo during analyzed period. According to Institute of Public Health of Federation of Bosnia and Herzegovina Report on public health status published in 2008, number of hypertensive patients shows constant growth during analyzed period, specially among productive population like it is shown in Figure 1 [6]. Number of hypertensive patients in Canton Sarajevo is presented in Table 2 showing increasing trend according to available data.
TABLE 1.
Number of inhabitants in Canton Sarajevo (2004-2008)

FIGURE 1.
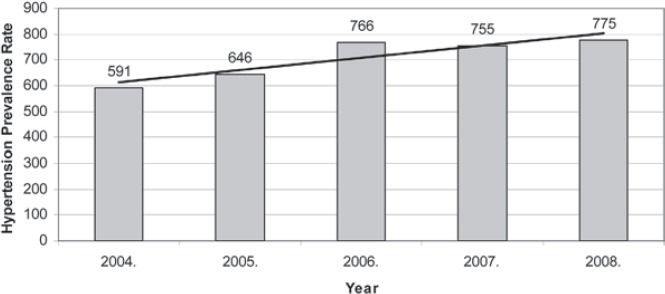
Prevalence of hypertension in Federation of Bosnia and Herzegovina during 2004-2008 (rate per 100 000 inhabitants)
TABLE 2.
Number of diagnosed hypertensive patients in Canton Sarajevo during last seven years
Constant drug expenditure growth is evident in Canton Sarajevo in previous years. Total drug expenditure has increased for 178% in 2008 relating to drug expenditure in 2003 according to Cantonal Health Insurance Fund (CHIF) data. Over 35% of this amount is spent on antihypertensive drugs [7].
In medical practice pharmacological treatment of hypertension is possible with use of five drug classes - diuretics, beta-blockers (BB), alpha-blockers (AB), angiotensin- converting enzyme inhibitors (ACE-I), calcium channel blockers (CCB) and angiotensin-II receptor blockers (ARB). It is also recommended to combine two different drug classes, mostly with diuretics. Antihypertensive drugs from all classes except ARBs are included in positive list in Canton Sarajevo with different reimbursement rate. Ministry of Health of Canton Sarajevo (MHCS) has formed expert group of cardiologists and pharmacologist who has developed Guidelines for diagnosing and therapy of hypertension which are published in 2005 and have been presented to health professionals, especially general practitioners (GPs). These guidelines do not differ than those published by international professional organizations [8]. According to this guidelines therapy should be initiated with diuretics or with ACEI or BB may be considered if targeted therapeutically outcome has not been reached or other medical reasons exists. Thiazide diuretic based therapy has been anticipated as cost-effective according to results of studies published previously [9]. Aim of therapy guidelines is, not only to reduce practice variation, guide appropriateness and measure quality of care, but also to improve rational pharmacotherapy and cost savings [10-12]. Research conducted by Avanzini et al. [13] has shown that hypertension guidelines implementation can be effective in rising quality of antihypertensive therapy in routine care. Beside fact and scientific evidence that guidelines positively affect therapeutic outcomes treatment guidelines are often not fully applied and implemented in practice [14, 15]. Research by Malacco et al. [16] has shown that majority of internist in Italy agree with guidelines but do not adhere to them completely in clinical practice. According to recommendations it is expected that first line drugs are mostly prescribed, so analysis of drug utilization can be useful to estimate adherence to treatment guidelines. Objective of this paper is to examine prescription patterns related to antihypertensive drugs in primary health care in Canton Sarajevo during five-year period.
After detailed antihypertensive drug utilization research, adherence to international and local hypertension treatment guidelines and its introduction effects on proscribing habits will be assessed.
MATERIALS AND METHODS
Drug utilization data are collected from the largest public pharmacy (retail) chain, representing more than 80% of pharmacies in Canton Sarajevo. Public pharmacy chain has been selected due to ability to provide data on drug utilization during analyzed period based on drug utilization database implemented in this institution. This data are used for calculation of drug utilization indicators. Only oral dosage forms have been taken into calculation, and defined daily dose has been calculated for each tablet. Five-year period is observed, from 2004 to 2008 collected data are representative, because from beginning of 2009 all other retail pharmacies in Canton Sarajevo became able to dispense CHIF reimbursed medicines including antihypertensives. Cantonal Ministry of Health has implemented Hypertension treatment guideline in 2005, so it will be possible to analyze its possible effects on proscribing habits. Assessment of adherence to this guidelines are based on assumption that first line medicines recommended for hypertension management should be most prescribed drugs with the highest share of utilization. Drug utilization is analyzed using ATC/DDD methodology proposed by World Health Organization. Drugs groups with these ATC codes are analyzed: C03 (diuretics), C07 (beta blockers), C08 (calcium channel blockers), C09 (ACE inhibitors, ACE inhibitors in combination with diuretics and Angiotensin II antagonists) and C02 (alpha blockers). For each of these drugs utilization is expressed in following utilization indicators: number of defined daily dose (DDD), number of defined daily dose per one thousand inhabitants per day (DDD/TID) and drug utilization 90% (DU90%) - the number of drugs accounting for 90% of drug use, serving as an indicator of the quality of drug prescribing. Financial value expressed in EUR currency has been used to stress financial impact of antihypertensive drug utilization. Local currency (convertible mark - BAM) is converted according to official conversion rate provided by Central Bank of Bosnia and Herzegovina (1 EUR = 1,95583 BAM). Prices used in calculation are retail prices. Because of VAT introduction in 2006 drug prices for years 2006-2008 are reduced for VAT rate of 17% so it was possible to compare with years 2004 and 2005 when drugs were treated as tax-free goods. Discounting to medication costs is not applied. Calculation of above mentioned utilization parameters has been based on WHO and EURO-MED-Stat recommendations. DDDs for each drug published on WHO Collaboration center for Drug Statistic Methodology internet site has been used for calculations. We have also analyzed all ATC subgroups at ATC 5th level (International Non-proprietary Names, INN) for above defined ATC groups.
RESULTS
The results clearly showed an increased utilization of antihypertensive drugs during observed 5-years period. Total utilization of antihypertensive drugs utilization increased each year compared to the previous one as follows: 10.59, 22.11, 11.16 and 6.5%, in 2005, 2006, 2007 and 2008, respectively. Table 3 shows overview of antihypertensive drugs utilization in Canton Sarajevo for each ATC expressed in total number of DDDs, DDD/TID and value in euro. Trends of antihypertensive drugs utilization is shown in Figure 2 with special linear representation for ACE inhibitors as leading drug group in consumption according to all indicators (especially DDD/TID and value). DU 90% segment related to utilization expressed in DDD/TID for each of analyzed ATC subgroups is shown in Table 4. We have found that diuretics, recommended as first line medicines fall out DU90% segment during the observed period, while ACE inhibitors persistently keeps the highest rate of utilization as Figure 3 shows. Our analysis has been conducted at 5th ATC level so we were able to analyze prescription of each INN. Cumulative overview of first ten proscribed ATC subgroups analyzed with DU90% segment is shown in Figure 4. According to DDD as measure for drug utilization, ACE inhibitors are most prescribed drug class. Second drug class is CCB, and third ranked are diuretics. We notice that diuretics utilization is decreasing from 2006 and being switched with BB which has constant growth during the observed period. The most prescribed plain ACEI is lizinopril followed by enalapril. Lizinopril share in total utilization among plain ACEI shows slight decrease mostly because of enalapril and ramipril share increase, but all of these drugs record constant growth when DDD/TID is analyzed; lizinopril growth is the highest. ACEIs in combination with thiazide diuretics shows same trend in consumption. Amlodipin and verapamil are two most proscribed CCB while amlodipin is prescribed almost two times more than verapamil. During 2004-2005 year period most of drug budget is spent on ACE inhibitors in combination with thiazide diuretics representing 46% of total antihypertensives expenditure (3 507 895 EUR on average per year). Right after this drug class we found ACE inhibitors with 26% participation in total expenditure. Calcium channel blockers (CCB) are third drug class followed by beta blockers representing 11% of total antihypertensive drug expenditure. The lowest budget impact is found for thiazide diuretics where average annual expenditure for these drug classes was 188 693 EUR or 2% total expenditure. The number of analyzed ATC groups in the DU90% segment varied from 2 during 2004, 2005 and 2006, to 1 in 2007 and 2008. C09 (ACEIs plain or in combination) and C08 comprises this segment, but from 2007 only C09 are covered by DU90%.
TABLE 3.
Overview of antihypertenzive drug utilization in Canton Sarajevo per different indicators during 2004-2008 period
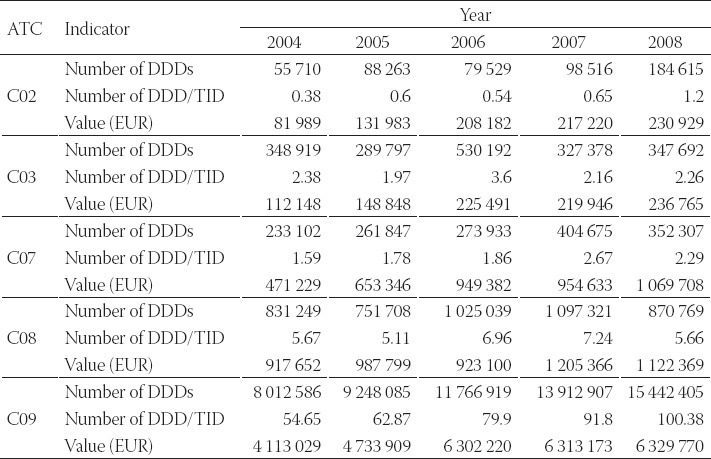
FIGURE 2.
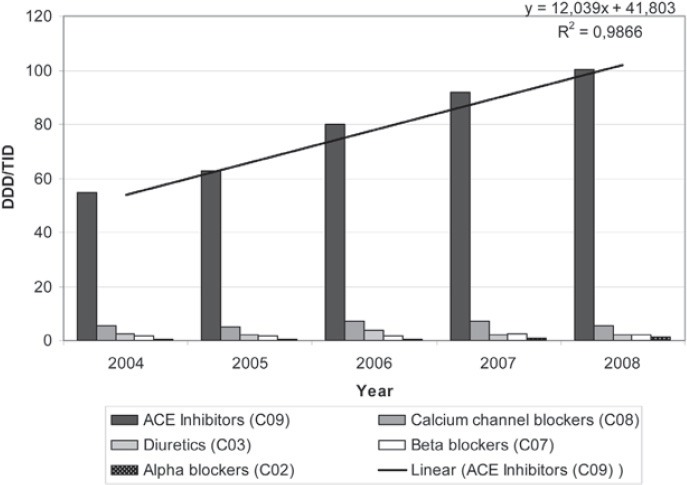
Trends of consumption antihypertensive drugs (therapeutic subgroups C02-C09) in Canton Sarajevo by years.
TABLE 4.
DU90% segment and DDD/TID utilization indicator for all analyzed antihypertensives, (ATC codes and generic names) in Canton Sarajevo (2004-2008).
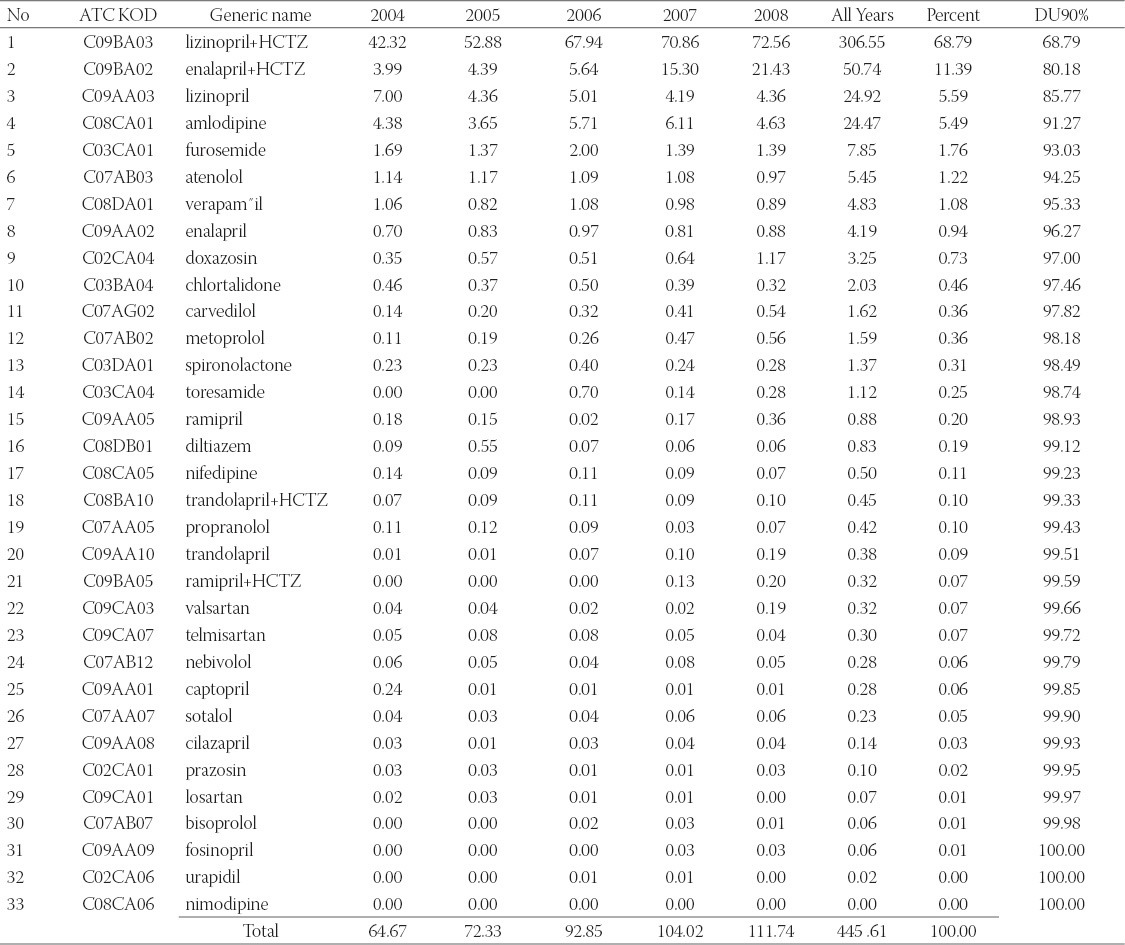
FIGURE 3.
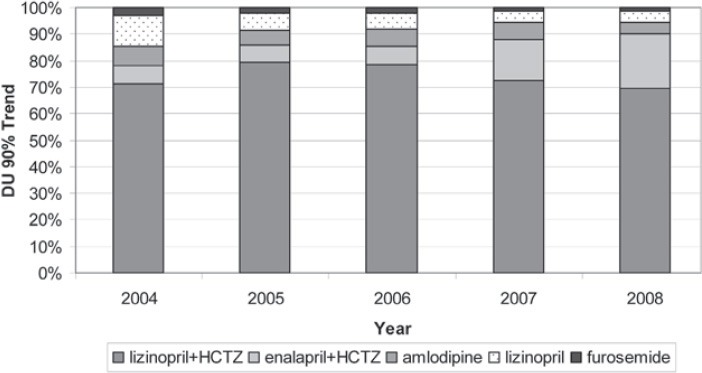
Drug utilization 90% (DU90%) for five most prescribed antihypertensive drugs and trends for Years 2004-2008
FIGURE 4.
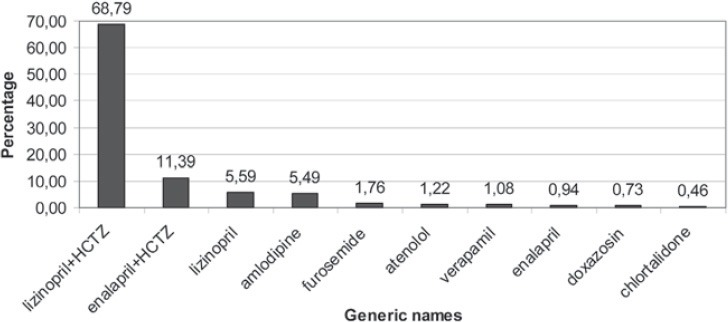
Cumulative DU90% for first ten most proscribed ATC subgroups during analysed period
DISCUSSION
Rising number of diagnosed hypertensive patients has direct impact on antihypertensive drugs consumption and expenditure, even data on the rate of disease are uncertain because of inconsistencies in health statistic system. According to available data, in Canton Sarajevo 30% of all drug expenditure in 2008 is spent for antihypertensive drugs [7]. Majority of drug budget is spent on ACE inhibitors in combination with thiazide diuretics representing 46% of total antihypertensive drug expenditure. It is interesting that Cantonal Health Insurance Fund has not introduced pure hydrochlorthiazide into list of reimbursed drugs even this diuretic is included in fixed combination of ACEIs. Positive reimbursement status of this medicine would contribute to greater prescribing of diuretics and directed prescribing patterns in cost saving direction. Positive effects of reimbursement is demonstrated on ramipril, as ACE inhibitor of new generation, recording consumption increase especially after year 2006 when reimbursement status has changed from 25% to 50%. Increase is represented by 10 times more proscribing than before. On the other hand, nebivolol is not reimbursed we found that this drug is almost consumed as sotalol which is 50% reimbursed. Most prescribed BB is atenolol which is fully reimbursed. Increased utilization trend of antihypertensive drugs was observed as a global one existing in most of developed and developing countries. In Croatia, C09 and C08 groups are leading antihypertensives and lizinopril shows the highest utilization during 2004-2008 period. Amlodipine is leading calcium channel blocker [17-21]. Same trend is present in Serbia and Montenegro as neighbouring countries [22,23]. Increasing utilization trend of cardiovascular medicines is also presented in Republic of Srpska, but with different prescribing patters than dose observed in Canton Sarajevo. In Republic of Srpska, most prescribed ACEI are captopril and enalapril from C09 group due to reimbursement status of these drugs. Amlodipine and atenolol has similar utilization as Canton Sarajevo [24]. Global hypertension treatment guidelines as well as local one implemented in 2005 suggest that first choice for treatment of early stage one hypertension should be treated with thiazide diuretics which are cost-effective but ACE inhibitors or beta blocker could be used regarding patient health status and presence of comorbidities. This research has shown that ACE inhibitors in combination with diuretics as well as plain ACE inhibitors are most prescribed anti- hypertensive drugs, while diuretics, which are recommended as first line therapy are ranked as forth in total antihypertensive drug utilization. Thiazide diuretic utilization dominates in Nordic countries [25]. Due to proven cost-effectiveness of diuretic based hypertension therapy use of these medicines, especially in treatment of uncomplicated hypertension, as first choice should be more in place. There are several approaches to monitor adherence to treatment guidelines and one of them are studies on drug utilization. Main limitation of this methodology in our paper is lack of detailed analysis of patient records. Systematic approach to this issue could improve analysis on patients or GPs level by providing data on diagnosis, previous prescriptions and justification of prescribed drugs.
It is obvious that first choice for initial hypertension treatment are ACE inhibitors, plain or in combination with thiazide diuretics. Possible reason for this is evident late hypertension diagnosis when disease is actually advanced as well as non-adherence to previous prescribed therapy and health professional advices for life style changes and avoid of risk factors. Previous studies shown good effectiveness and safety of lisinopril plus hydrochlorthiazide used in patients with mild, moderate and severe hypertension, as well as effects on regression of left ventricular hypertrophy. This may be other reason for prescribing patterns present in Canton Sarajevo. [26,27] Since the C09 drug group with the highest price is first choice in the prescription which price, economic justification is questionable especially for a country like Bosnia and Herzegovina. All this indicate that it is necessary to educate health professionals in health economic and pharmacoeconomic area what can help them to make right decision. Development and further promotion of treatment guidelines implementation in routine practice is also recommended.
CONCLUSION
This research has showed increasing trend of antihypertensive drug utilization in Canton Sarajevo during five years period (2004-2008). ACE inhibitors plus thiazide diuretics as fixed combinations are most prescribed antihypertensive drugs. Due to low utilization of thiazide diuretics in Canton Sarajevo the adherence to the guidelines is not as consistent as it could be. Total drug expenditure and antihypertensives utilization in Canton Sarajevo is in constant growth so cost-effective treatment choice will lead to proper resource of scarce resources.
DECLARATION OF INTEREST
Authors do not have any commercial affiliations, or potential conflicts of interest associated with this work submitted for publication.
REFERENCES
- [1].2003. World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–1992. doi: 10.1097/00004872-200311000-00002. [DOI] [PubMed] [Google Scholar]
- [2].Wolf-Maier K, Cooper RS, Banegas JR, et al. Hypertension Prevalence and Blood Pressure Levels in 6 European Countries, Canada, and the United States. JAMA. 2003;289(18):2363–2369. doi: 10.1001/jama.289.18.2363. [DOI] [PubMed] [Google Scholar]
- [3].Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- [4].Federal Office of Statistics. [accessed on 30.08.2009]. URL: http://www.fzs.ba/Podaci/us-troj11.htm .
- [5].Chamber of Economy of Canton Sarajevo. [accessed on 30.08.2009]. URL: http://www.pksa.com.ba/bosanski/poslovni_ambijent/stanje_privrede_ks/stanje_privrede.pdf .
- [6].Institute of Public Health of Federation of Bosnia and Herzegovina. [accessed on 30.08.2009]. URL: http://www.zzjzfbih.ba/publikacije/izvjestaji .
- [7].Health Insurance Fund of Canton Sarajevo. Annual report: Drug expenditure in Canton Sarajevo in 2008, Sarajevo. 2009 in Bosnian. [Google Scholar]
- [8].Ministry of Health of Canton Sarajevo. Diagnostic and therapy guidelines for hypertension, Sarajevo. 2005 in Bosnian. [Google Scholar]
- [9].Chen GJ, Ferrucci L, Moran WP, Pahor M. A cost-minimization analysis of diuretic-based antihypertensive therapy reducing cardiovascular events in older adults with isolated systolic hypertension. Cost EffResour Alloc. 2005;3:2–8. doi: 10.1186/1478-7547-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Bodnheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. JAMA. 2002;288:1909–1914. doi: 10.1001/jama.288.15.1909. [DOI] [PubMed] [Google Scholar]
- [11].Gaziano TA, Steyn K, Cohen DJ, et al. Cost-Effectiveness analysis of hypertension guidelines in South Africa. Circulation. 2005;112(23):3569–3576. doi: 10.1161/CIRCULATIONAHA.105.535922. [DOI] [PubMed] [Google Scholar]
- [12].Xu KT, Moloney M, Phillips S. Economics of suboptimal drug use: cost-saving of using JNC-recommended medication. Am J Manag Vare. 2003;9:529–536. [PubMed] [Google Scholar]
- [13].Avanzini F, Corsetti A, Maglione T, et al. Simple, shared guidelines raise the quality of antihypertensive treatment in routine care. Am Heart J. 2002;144(4):726–732. doi: 10.1067/mhj.2002.125327. [DOI] [PubMed] [Google Scholar]
- [14].Messerli FH. Antihypertensive therapy: beta-blockers and diuretics-why physicians not always follow guidelines? BUMC Proceedings. 2000;13:128–131. doi: 10.1080/08998280.2000.11927654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Pedone C, Lapane KL. Generalizability of guidelines and physicians’ adherence. Case study on the Sixth Joint National Committee's Guidelines on hypertension. BMC Public Health. 2003;3:24–34. doi: 10.1186/1471-2458-3-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Malacco E, Ferri C, Grandi AM, et al. Treatment of hypertension and adherence to treatment guidelines in clinical practice: An Italian study. Adv Ther. 2005;22(2):96–106. doi: 10.1007/BF02849881. [DOI] [PubMed] [Google Scholar]
- [17].Croatian Agency for Medicines and Medical Devices. Medicines consumption in 2004 Report [in Croatian] [accessed on 15.01.2011]. URL: http://www.almp.hr/?ln=hr&w=publikacije&d=promet_lijekova _2004 .
- [18].Croatian Agency for Medicines and Medical Devices. Medicines consumption in 2005 Report [in Croatian] [accessed on 15.01.2011]. URL: http://www.almp.hr/?ln=hr&w=publikacije&d=promet_lijekova_2005 .
- [19].Croatian Agency for Medicines and Medical Devices. Medicines consumption in 2006 Report [in Croatian] [accessed on 15.01.2011]. URL: http http://www.almp.hr/?ln=hr&w=publikacije&d=promet_lijekova_2006 .
- [20].Croatian Agency for Medicines and Medical Devices. Medicines consumption in 2007 Report [in Croatian] [accessed on 15.01.2011]. URL: http://www.almp.hr/?ln=hr&w=publikacije&d=promet_lijekova_2007 .
- [21].Croatian Agency for Medicines and Medical Devices. Medicines consumption in 2008 Report [in Croatian] [accessed on 15.01.2011]. URL: http http://www.almp.hr/?ln=hr&w=publikacije&d=promet_lijekova_2008 .
- [22].Consumption of Medicines 2004/2005 [in Serbian] Belgrade: Agency; 2006. Medicines and Medical Devices Agency of Serbia. [Google Scholar]
- [23].Health Insurance Fund of Montenegro. [accessed on 15.01.2011]. URL: http://fzocg.me/index.php#sadrzaj(22)
- [24].Markovic-Petkovic V, Stoisavljevic S, Skrbic R. Utilization of cardiovascular medicines in Republic of Srpska, Bosnia and Herzegovina, 5 years study. Pharmacoepidemiol Drug Saf. 2009;18:320–326. doi: 10.1002/pds.1704. [DOI] [PubMed] [Google Scholar]
- [25].Norwegian Institute for Public Health. [accessed on 15.01.2011]. URL: http://www.fhi.no .
- [26].Gerc V, Begovic B, Vehabovic M, Georgievich Voronkov L, et al. Fixed combination lisinopril plus hydrochlorthiazide in the treatment of essential arterial hypertension: An opened, multi-centre, prospective clinical trial. Bosn J Basic Med Sci. 2007;7(4):377–382. doi: 10.17305/bjbms.2007.3031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Gerc V, Begovic B, Vehabovic M, Georgievich Vornkov L, et al. Effects of fixed combination of lisinopril plus hydrochlorthiazide on regression of left ventricular hypertrophy in patients with essential hypertension: An opened, multi-centre, prospective clinical trial. Bosn J Basic Med Sci. 2008;8(3):214–219. doi: 10.17305/bjbms.2008.2920. [DOI] [PMC free article] [PubMed] [Google Scholar]