

Abstract
To investigate shoulder scoring systems used in Europe and North America and how outcomes might be classified after shoulder joint replacement. All research papers published in four major journals in 2012 and 2013 were reviewed for the shoulder scoring systems used in their published papers. A method of identifying how outcomes after shoulder arthroplasty might be used to categorize patients into fair, good, very good and excellent outcomes was explored using the outcome evaluations from patients treated in our own unit. A total of 174 research articles that were published in the four journals used some form of shoulder scoring system. The outcome from shoulder arthroplasty in our unit has been evaluated using the constant score (CS) and the oxford shoulder score and these scores have been used to evaluate individual patient outcomes. CSs of < 30 = unsatisfactory; 30-39 = fair; 40-59 = good; 60-69 = very good; and 70 and over = excellent. The most popular shoulder scoring systems in North America were Simple Shoulder Test and American shoulder and elbow surgeons standard shoulder assessment form score and in Europe CS, Oxford Shoulder Score and DASH score.
Keywords: Shoulder joint, Arthroplasty, Replacement, Scoring methods, Operations, Surgery, Surgical therapy, Assessment, Patient outcomes, Classification
Core tip: We have identified the most commonly used shoulder scoring systems used when results of surgery are published. The constant score (CS) can be used to categorize the outcomes after shoulder arthroplasty into unsatisfactory; fair; good; very good; and excellent. This be carried out using both the original CS and the Adjusted (for age and sex) CS. For the majority of orthopaedic surgeons the reporting of outcomes in this way is clearer than providing the mean and standard deviation of one of the commonly used shoulder scoring systems.
INTRODUCTION
Functional shoulder disabilities are frequently reported by patients with a wide variety of conditions, such as arthritis, rotator cuff disease, breast carcinoma, trauma and radiation therapy[1]. Upper limb disabilities may include pain, stiffness, decreased range of movement, lymphoedema and reduced activity tolerance. There are a myriad of scoring systems used in everyday orthopaedic practise and research, and a number of scoring systems have been developed and established to assess the function and limitations of the shoulder. None of these are ideal methods for correlating both the physician’s and the patient’s perspective[2] as some are more inclined towards the opinion of the physician while others are more centred on the patient’s self-assessment. A review of four popular journals (see below) showed that in their 2012 volumes 16 different scoring systems were commonly used to evaluate shoulder conditions. This can make it difficult to compare outcomes between studies and interventions, and makes it more problematic for practising orthopaedic surgeons to decide which of their treatment options is providing the best outcomes if the scoring systems used are different. This review aims to evaluate the evidence behind the scoring systems, and will provide some guidance as to which to rely on.
Many shoulder scoring systems are used inappropriately without being tested for their sensitivity, reproducibility and validity[3]. In order to apply any scoring system, their complete validation must be documented. Over the last 5 years the use of patient reported outcome measures (PROMs) have been promoted as they are considered to place a greater emphasis on the quality of life perceived by the patient[4]. There is therefore a need to develop questionnaires or shoulder scoring outcome measures which can address specific conditions or abnormalities of the shoulder so that they can fulfil both the patient’s and clinician’s perspective[5]. Above all, shoulder scoring systems need to be evaluated and modified for specific condition to produce a valid, sensitive and reproductive outcome.
COMMONLY USED SCORING SYSTEMS
Constant score
The constant score (CS)[6] is one of the most commonly used shoulder scoring systems[7], and is considered the gold standard in Europe[8]. It is comprised of 4 parts - Pain reported by the patient (15 points); Activities of Daily Living reported by the patient (20 points); Range of Movement - assessed by the examiner (40 points) and strength - assessed by the examiner (25 points), with the better functioning shoulders having a greater number of points up to a maximum of 100 points. It has a long history and is easy to apply, hence it is used very extensively[7,9]. Because of its long term use since it was formally published in 1987, it is likely to remain popular so that treatment outcomes previously reported in the literature can be compared with more modern surgical or non-surgical treatments. Authors have criticised the CS, suggesting its level of standardisation is poor[10,11]. It does not evaluate shoulder instability and this is a weakness[12], as is the non-standardised strength evaluation[13] although Bankes et al[14] have described the fixed spring balance modification (fixed to a desk or to the floor) as a low-cost technique, which gave similar and equally reproducible values for power when compared with an electronic measuring device[15]. However, it does reliably detect improvements in shoulder function after intervention[16]. Some concerns have been expressed about the different results reported for males and females and the reduction of scores with increasing age[15] but these have been addressed by the use of the modified CS, which corrects for both age and gender[17].
Oxford shoulder score
The oxford shoulder score (OSS)[18] is a joint specific scoring system that is patient assessed, and scored out of 48. It is an outcome measure based on the patient’s perspective of their outcome and using standard questions where 4 of the 12 questions are related to pain. The OSS is a reliable, easy to use outcome measure which is sensitive to surgical outcome and clinical changes[19,20]. It has good correlation with clinical findings. Again the OSS does not assess shoulder instability[21] and, as a consequence the oxford instability score (OSIS) has been developed subsequently[22] (see below). Olley et al[20] concluded that the OSS can be used for audit purposes, however, they have suggested that larger prospective studies should be carried out to identify whether OSS varies with age, gender, and size of rotator cuff tear or not. Frich et al[23] studied the Danish version of the OSS, reporting that the OSS psychometric properties are valid and reliable. They also reported that the OSS is appropriate to evaluate individuals suffering from degenerative or post-traumatic shoulder diseases.
OSIS
The OSIS[22] is based on a 5-option response (Likert scale) for each item, with each response scored from 0 to 4, with 4 being the best outcome. All questions are laid out similarly with response categories denoting least (or no) symptoms being to the left of the page (scoring 4) and those representing greatest severity lying on the right hand side (scoring 0). The overall OSIS score is reached by simply summing the scores received for individual questions. This results in a continuous score ranging from 0 (most severe symptoms) to 48 (least symptoms).
Disability of the arm, shoulder and hand
The disability of the arm, shoulder and hand (DASH) score is a 30-item patient-reported tool to assess symptoms and physical disability in the arm. The DASH parameters are symptoms, physical, social and psychological functions. The score evaluates pain, physical disability and sleep disturbance. The pain score and physical disability assessment make a large part of this outcome measure. The DASH score has been shown to assess improvement after surgery [Lewis (2012)], and multiple authors have found it to be a valid and reliable score [Slobogean et al[24] (2010) Huisstede et al[25] (2009) Bilberg et al[26] (2012)]. As with the OSS, the DASH score has also been used cross-culturally and has provided similar results (Jianmongkol et al[27] 2012). However, as the name suggests, it is not a shoulder specific scoring system, and being a patient self-reported scoring system, DASH may fall victim to patient bias. In addition the DASH score results are inverted with the higher scores (maximum = 100) representing a greater disability and the lower scores occurring in a good functioning arm.
Simple shoulder test
The simple shoulder test (SST) was developed by Rick Matsen, initially in San Antonio and later in Seattle at the University of Washington Shoulder and Elbow Service. It has been reported as simple, valid, highly reliable and free practical patient self-assessment tool. The SST is a questionnaire with 12 questions designed for “yes/no” answers. It is validated for pre and post-operative shoulder function, and, is popular in North America[28]. However, it has also been validated in a number of other countries[29], including Brazil[30], Holland[16] and Italy[31] and is considered to be user friendly[16]. Drawbacks associated with the SST are perhaps its generosity (high scores when significant disability is present), and the different effects of age and type of injury or disease on the scores.
American shoulder and elbow surgeons standard shoulder assessment form
The American shoulder and elbow surgeons standard shoulder assessment form (ASES)[32] is easy to apply and consists of an assessment of the patients activities of daily living and a patient self-evaluation. It can be applied to all shoulder patients regardless of diagnosis. Some authors report it has good reliability, high constructive validity and high responsiveness[32]. However, Bafus et al[33] have reported that the ASES is not a valid and reliable scoring system for shoulder pathology as there are questions like “do usual sport” and “throw ball overhand” which are not easy for some patients to answer as they do neither. Although ASES is a highly accepted shoulder scoring system, it does contain several shortcomings in its construction.
Western ontario shoulder instability index
The Western ontario shoulder instability index (WOSI)[34] is a specific instability score designed to address the lack of validity of other scores in assessing shoulder instability symptoms. It is a self-assessment shoulder scoring tool that is disease-specific and also assesses the quality of life of patients with symptomatic shoulder instability. It is highly accepted by patients and surgeons because of the perceived importance of the items questioned, and has been found to be valid and reliable[35,36]. The disadvantages of the WOSI are that it has 21 questions each scored using 100 mm visual analogue scales, and its research usability is moderate as it is specific to instability conditions.
Japanese orthopaedic association shoulder score
The Japanese orthopaedic association (JOA) shoulder score is extensively used throughout Japan but it is not commonly reported outside that country. It is a much more complicated scoring system. For each of the 36 questions, patients are asked to self-interpret their symptoms using a scoring system divided into five levels (0 to 4) in which the larger values mean a better shoulder. The grades are: I have no difficulties (= 4); I have minor difficulties (= 3); I have some difficulties but I can manage on my own (= 2); I have major difficulties and require help from someone (= 1); and I cannot do it at all (= 0). These are very similar to the answers to the OSS questions, but 32 questions are used by the JOA while only 12 are used for the OSS. However the complex part is the final calculation which involves transferring scores from one domain to another, and as a result, it has not found popularity outside Japan.
Short form-36, short form-12, EQ-5D and short form-6D for general health
The short form (SF)-36 and the shorter SF-12 have become the most widely used measures of general health in clinical studies throughout the world. The SF-36 currently generates eight dimension scores and two summary scores for physical and mental health. Whilst such scores provide an excellent means for judging the effectiveness of health care interventions, they have only a limited application in economic evaluation because they are not based on preferences. The SF-6D[37] provides a means for using the SF-36 and SF-12 in economic evaluation by estimating a preference-based single index measure for health from these data using general population values. The SF-6D allows the analyst to obtain quality adjusted life years from the SF-36 for use in cost utility analysis. The EQ-5D is a similar, five-dimension, questionnaire and is now becoming popular in evaluating cost utility analysis and changes in general health after surgical operations in the United Kingdom and Europe.
REVIEW OF THE MOST COMMONLY USED SHOULDER OUTCOME SCORES IN EUROPE AND AMERICA
A review was carried out of all the articles in the 2012 and 2013 volumes of four major MEDLINE/PubMed referenced journals: The Journal of Bone and Joint Surgery (Am); The Journal of Bone and Joint Surgery (Br - now called the Bone and Joint Journal); The Journal of Shoulder and Elbow Surgery; and the American Journal of Sports Medicine. That review is summarised in Figures 1 and 2 and Table 1. The CS and the ASES are those most frequently used. This may be because of their long history, and the tradition of combining both objective and subjective assessments of patients. Both have also been extensively validated. However, there is evidence that patient self-reported scoring is not only easier and cheaper, but may also be a more accurate method of assessing orthopaedic outcomes[38-40]. Other popular scoring systems include the DASH, the SST and the university of California-Los Angeles shoulder scale (UCLA). The remainder are used far less commonly, sometimes for specialised situations (i.e., the Kerlan-Jobe Orthopaedic Clinic - KJOC overhead athlete score). Different shoulder scoring systems appear to be used in different countries. In Europe the CS, DASH and the OSS appear to be the most common, while in North America, the ASES, SST, and UCLA are used to assess the shoulder most often. All of these scoring systems either test different things or features in different ways to assess shoulder function. However, one would presume some kind of inter-correlation might be found between the scoring systems used in Europe and those being performed in United States as all of them intend to evaluate the shoulder function.
Figure 1.
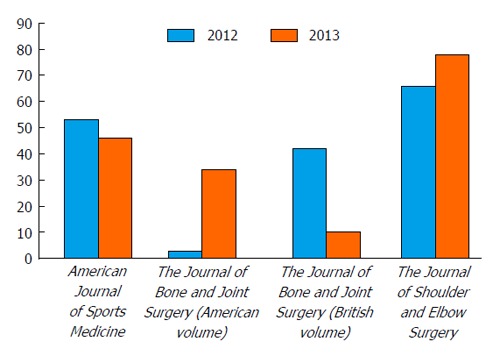
Number of articles that used different shoulder scoring systems during 2012 and 2013.
Figure 2.
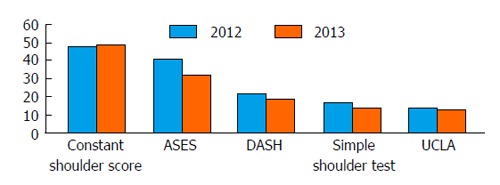
Most popular shoulder scoring systems during 2012 and 2013. ASES: American shoulder and elbow surgeons standard shoulder assessment form; DASH: Disabilities of the arm, shoulder and hand; UCLA: University of California-Los Angeles shoulder scale.
Table 1.
Shoulder scoring systems used in 2012 and 2013
| Shoulder scoring system | No. of times used | No. of times used | No. of times used in |
| in articles in 2012 | in articles in 2013 | articles in 2012 and 2013 | |
| CS | 47 | 44 | 91 |
| American shoulder and elbow surgeons evaluation form | 41 | 32 | 73 |
| The disability of the arm, shoulder and hand score | 22 | 13 | 35 |
| SST | 16 | 13 | 29 |
| University of California/Los Angeles shoulder score | 15 | 13 | 28 |
| Western ontario osteoarthritis score | 6 | 0 | 6 |
| The OSS | 4 | 6 | 10 |
| SF-12 general health | 3 | 7 | 10 |
| Western ontario rotator cuff score | 3 | 5 | 8 |
| SF-36 general health | 1 | 8 | 9 |
| Penn shoulder score | 1 | 2 | 3 |
| Shoulder pain and disability index | 1 | 4 | 5 |
| Western ontario shoulder instability score | 1 | 2 | 3 |
| Rowe shoulder instability score | 1 | 2 | 3 |
| Single assessment numeric evaluation score | 1 | 7 | 8 |
| Kerlan-Jobe orthopaedic clinic overhead athlete score | 1 | 2 | 3 |
| Hospital for special surgery shoulder score | 0 | 0 | 0 |
| OSIS | 0 | 2 | 2 |
CS: Constant score; SST: Simple shoulder test; OSS: Oxford shoulder score; SF-12: Short form-12; OSIS: Oxford instability score.
EQUIVALENCE OF SHOULDER SCORING SYSTEMS
A number of papers have evaluated whether different scoring systems are comparable. The CS is a combination of both a clinically-based and patient assessment outcome measure for patients with shoulder problems, while most other scores focus on more patient-based outcome measures. One would therefore suspect that the CS cannot be interchanged or merged with the other scoring systems which are based on self-assessment by the patients. In contrast, OSS, DASH, SST and WOSI scoring systems can be compared and interchanged to some extent. However there are confounding factors which will influence these scores. All the patient-based assessment outcome measures may be affected by personal or patient response biases. Scott et al[41] have compared the CS and OSS, and found that using the OSS gave a higher proportionate overall score for the shoulder patient than the CS and that the agreement between the scores was poor. However, other studies have revealed that OSS is more stable than CS in terms of outcome measures[18,42]. Skutek et al[43] have also shown only moderate correlation between the CS and SST. Hirschmann et al[13] suggested that CS is poor at measuring shoulder strength and should be re-evaluated for its sensitivity and reliability. Lewis[44] reviewed patients with subacromial impingement, and measured CS, DASH and the EuroQol (EQ-5D) quality of life measurement. He found that CS and DASH were both significantly improved in the intervention exercise group, but CS improved more than DASH, suggesting poor agreement between the two systems.
As the OSS and DASH are patient self-assessment measurement outcomes they could be expected to be interrelated to each other but may sometimes be used combined. Studies have reported that OSS is better to assess the surgical outcome in patients with rheumatoid arthritis as compared to the DASH and SF-36[45].
In order to check the reliability and validity of DASH and SF-6D, Slobogean et al[24] studied patients with treated proximal humeral fractures. They reported that DASH and SF-6D questionnaires were adequate in assessing psychometric properties, and suggested that these scoring systems are appropriate to assess the outcome in patients treated for proximal humeral fractures. Interestingly, van de Walter et al[46] reviewed five scoring systems-CS, -OSS, -DASH, -UCLA and a Subjective Shoulder Value following proximal humeral fractures and concluded that currently available shoulder scoring systems may not offer significant value for assessing functional improvement after such fractures.
Godfrey et al[29] conducted a study on 1077 patients suffering from shoulder instability to assess the reliability, validity, and responsiveness of the SST. They found that the SST is significantly correlated with the ASES score and both responded to change in shoulder function. However, they reported that the results were different for different age groups and different types of shoulder injury. The study conducted by van Kampen et al[16] also revealed that the SST is highly correlated with the DASH, OSS and SF-36 in terms of physical subscales; however, it did not correlate well with the CS.
WHEN TO USE SCORING SYSTEMS
Many surgical and non-surgical shoulder interventions take months to gain full benefit after shoulder treatment, so any follow up has to be measured over months and years to evaluate longer term outcomes. Our preference is to score all our patients preoperatively, then at 6 mo and 1 year if the patient continues to be followed up. For shoulder joint replacement patient’s scores are then repeated at 3, 5 and 10 years unless the patients are scored more regularly as part of a research protocol.
USING THE CONSTANT SCORE TO EVALUATE THE OUTCOME FOLLOWING SHOULDER ARTHROPLASTY
It has been standard practice in our unit for 20 years to use the CS to evaluate the outcome from shoulder operations and, in particular shoulder arthroplasty. Previous studies, reported in 2007[15] have highlighted the changes in the CS in normal people with increasing age and between the sexes. Table 2 shows the estimated normal CSs for age and sex.
Table 2.
Estimated normal constant scores for age and sex[15]
| Age (yr) | Men | Women |
| 50-59 | 95 ± 2 | 88 ± 2 |
| 60-69 | 92 ± 2 | 85 ± 2 |
| 70-79 | 89 ± 2 | 82 ± 2 |
| 80-89 | 86 ± 2 | 79 ± 2 |
As a practical example from our unit, in 2013 we evaluated the outcomes from all our primary anatomic and inverse (or reverse) shoulder replacements using a new Vaios shoulder replacement design[47] and the results are shown in Table 3 for anatomic shoulder arthroplasty and Table 4 for reverse shoulder arthroplasty. However these means and standard deviations are difficult to understand for most orthopaedic surgeons but they become more meaningful if they are converted into different grades of improvement.
Table 3.
Constant and oxford shoulder scores for the vaios anatomic shoulder replacements
| Outcome measure | No. of | Oxford score | Pain | ADL | ROM | Strength | Total CS | Constant score adjusted |
| shoulders | (/48) | (/15) | (/20) | (/40) | (/25) | (/100) | for age and sex (%) | |
| Pre-op mean (SD) | 49 | 16.8 (7.8) | 4.8 (3.2) | 6.7 (3.7) | 10.1 (5.1) | 1.0 (2.2) | 21.9 (9.7) | 29.2 (12.4) |
| Post-op 1 yr mean (SD) | 49 | 33.0 (12.8) | 11.3 (4.1) | 13.3 (4.7) | 20.0 (11.3) | 4.0 (4.8) | 44.6 (17.6) | 59.6 (24.0) |
| Post-op 2 yr Mean (SD) | 30 | 36.5 (12.3) | 12.0 (3.9) | 14.0 (6.0) | 20.5 (10.7) | 6.7 (6.0) | 47.2 (19.4) | 62.1 (22.8) |
| Post-op 3 yr mean (SD) | 8 | 38.4 (10.6) | 10.8 (2.9) | 11.8 (4.0) | 16.4 (6.2) | 6.4 (3.6) | 45.4 (10.4) | 63.6 (21.0) |
ADL: Activities of daily living; CS: Constant score.
Table 4.
Constant and oxford shoulder scores for the vaios inverse shoulder replacements
| Outcome measure | No. of shoulders | Oxford score | Pain | ADL | ROM | Strength | Total CS | Constant score adjusted |
| (/48) | (/15) | (/20) | (/40) | (/25) | (/100) | for age and sex (%) | ||
| Pre-op mean (SD) | 63 | 18.9 (9.0) | 6.6 (4.0) | 8.0 (4.2) | 11.2 (8.1) | 0.8 (2.1) | 25.9 (13.1) | 37.0 (18.2) |
| Post-op 1 yr mean (SD) | 63 | 35.4 (11.7) | 12.3 (3.7) | 13.5 (5.4) | 22.8 (10.5) | 4.7 (5.3) | 49.4 (18.1) | 69.0 (25.5) |
| Post-op 2 yr mean (SD) | 28 | 34.4 (13.8) | 12.4 (3.7) | 13.7 (5.5) | 23.9 (11.5) | 5.6 (4.3) | 49.8 (19.0) | 69.7 (27.7) |
| Post-op 3 yr mean (SD) | 6 | 33.0 (10.6) | 11.8 (4.7) | 16.3 (3.9) | 24.0 (9.8) | 7.8 (0.5) | 59.8 (17.0) | 81.6 (23.5) |
ADL: Activities of daily living; CS: Constant score.
We have therefore developed a meaningful grading system for assessing the outcomes following arthroplasty using either the CS as shown in Table 5 or the age and sex adjusted CS as shown in Table 6. These results are more meaningful than means and standard deviations and allow us to appreciate that 60% of patients achieve a good, very good or excellent result after anatomic Total Shoulder Replacement while 76% achieve a good, very good or excellent result after Inverse or Reverse shoulder replacement using the age and sex adjusted CS.
Table 5.
Categories of outcome after shoulder arthroplasty using the constant score
| Category | Total CS (/100) | Age and sex adjusted CS (%) |
| Average shoulder function before arthroplasty | < 30 | < 40 |
| Post-op unsatisfactory | < 30 | < 40 |
| Post-op fair outcome | 30-39 | 40-49 |
| Post-op good outcome | 40-59 | 50-69 |
| Post-op very good outcome | 60-69 | 70-79 |
| Post-op excellent outcome (i.e., a virtually normal shoulder) | ≥ 70 | ≥ 80 |
CS: Constant score.
Table 6.
Stratified outcome for the vaios primary total shoulder replacements using the adjusted constant score (adjusted for age and sex)
| Post-op outcome | Adjusted CS (%) | No. of anatomic TSRs n = 46 | % anatomic TSRs using adjusted CS | No. of inverse TSRs n = 58 | % inverse TSRs using adjusted CS |
| Unsatisfactory outcome | < 40 | 10 | 22 | 9 | 16 |
| Fair outcome | 40-49 | 9 | 20 | 5 | 9 |
| Good outcome | 50-69 | 9 | 20 | 14 | 24 |
| Very good outcome | 70-79 | 3 | 7 | 5 | 9 |
| Excellent outcome | ≥ 80 | 15 | 33 | 25 | 43 |
| Totals | 46 | 100 | 58 | 100 |
CS: Constant score.
CONCLUSION
It is difficult to choose the best scoring system as a “best choice of outcome measurement tool” for patients with shoulder problems. There remains a need to develop a comprehensive outcome measurement tool that can adequately deal with both the clinician’s and the patient’s perspective. None of the scoring systems ideally fulfil this criterion. For instance, the clinically-based outcome measuring tool may not satisfy the patient, and the patient self-assessment tools may not provide the information that the clinician believes is important. Patient-based assessment tools may fall a victim to bias as the patient may under or over report symptoms: under-reporting if they wish to please the surgeon or over-reporting for secondary (or compensation related) gain. Similarly, physician-based tools may not truly reflect what the patient feels about their outcome. Therefore it makes sense to combine scoring systems when collecting data for outcome measures, and we would recommend using multiple scores, including clinically - based and patient self-assessment tools. We currently use the CS and OSS in our unit for the majority of our patients but the SST has also been proven to be a valuable outcome assessment in North America. These assessment do need to be carried out at the appropriate time and our policy in Nottingham is to always carry out a pre-operative assessment and then to carry out the first post-operative evaluation at 6 mo after surgery when the patient’s condition is reaching a plateau. The United Kingdom health service has become much more focused on using PROMs and many are moving towards using the OSS as their preferred PROM for general shoulder assessment.
Footnotes
P- Reviewer: Juneja D S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Conflict-of-interest: This article focuses on shoulder scoring systems used world-wide. None of the authors have any conflict of interest in relation to any of these shoulder scoring systems. The shoulder replacement results reported are for the Vaios shoulder replacement (marketed by JRI Orthopaedics Ltd) and are the results for a consecutive series of primary shoulder replacements carried out by the Senior Author (WAW) who was the co-designer of the Vaios shoulder replacement and has a Consultancy agreement with JRI Orthopaedics Ltd. None of the other co-authors have any conflict of interest in relation to shoulder replacement surgery.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: March 12, 2014
First decision: April 30, 2014
Article in press: December 19, 2014
References
- 1.Fong SS, Ng SS, Luk WS, Chung JW, Chung LM, Tsang WW, Chow LP. Shoulder Mobility, Muscular Strength, and Quality of Life in Breast Cancer Survivors with and without Tai Chi Qigong Training. Evid Based Complement Alternat Med. 2013;2013:787169. doi: 10.1155/2013/787169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Longo UG, Vasta S, Maffulli N, Denaro V. Scoring systems for the functional assessment of patients with rotator cuff pathology. Sports Med Arthrosc. 2011;19:310–320. doi: 10.1097/JSA.0b013e31820af9b6. [DOI] [PubMed] [Google Scholar]
- 3.Noorani AM, Roberts DJ, Malone AA, Waters TS, Jaggi A, Lambert SM, Bayley I. Validation of the Stanmore percentage of normal shoulder assessment. Int J Shoulder Surg. 2012;6:9–14. doi: 10.4103/0973-6042.94307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Royal College of Surgeons of England. Measuring surgical outcomes. 2013. Available from: http:// www.rcseng.ac.uk/media/media-background-briefings-and-statistics/measuring-surgical-outcomes. [Google Scholar]
- 5.Croft P. Measuring up to shoulder pain. Ann Rheum Dis. 1998;57:65–66. doi: 10.1136/ard.57.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;(214):160–164. [PubMed] [Google Scholar]
- 7.Blonna D, Scelsi M, Marini E, Bellato E, Tellini A, Rossi R, Bonasia DE, Castoldi F. Can we improve the reliability of the Constant-Murley score? J Shoulder Elbow Surg. 2012;21:4–12. doi: 10.1016/j.jse.2011.07.014. [DOI] [PubMed] [Google Scholar]
- 8.Rocourt MH, Radlinger L, Kalberer F, Sanavi S, Schmid NS, Leunig M, Hertel R. Evaluation of intratester and intertester reliability of the Constant-Murley shoulder assessment. J Shoulder Elbow Surg. 2008;17:364–369. doi: 10.1016/j.jse.2007.06.024. [DOI] [PubMed] [Google Scholar]
- 9.Ge Y, Chen S, Chen J, Hua Y, Li Y. The development and evaluation of a new shoulder scoring system based on the view of patients and physicians: the Fudan University shoulder score. Arthroscopy. 2013;29:613–622. doi: 10.1016/j.arthro.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 10.Razmjou H, Holtby R, Christakis M, Axelrod T, Richards R. Impact of prosthetic design on clinical and radiologic outcomes of total shoulder arthroplasty: a prospective study. J Shoulder Elbow Surg. 2013;22:206–214. doi: 10.1016/j.jse.2012.04.016. [DOI] [PubMed] [Google Scholar]
- 11.Roy JS, MacDermid JC, Woodhouse LJ. A systematic review of the psychometric properties of the Constant-Murley score. J Shoulder Elbow Surg. 2010;19:157–164. doi: 10.1016/j.jse.2009.04.008. [DOI] [PubMed] [Google Scholar]
- 12.Kemp KA, Sheps DM, Beaupre LA, Styles-Tripp F, Luciak-Corea C, Balyk R. An evaluation of the responsiveness and discriminant validity of shoulder questionnaires among patients receiving surgical correction of shoulder instability. ScientificWorldJournal. 2012;2012:410125. doi: 10.1100/2012/410125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hirschmann MT, Wind B, Amsler F, Gross T. Reliability of shoulder abduction strength measure for the Constant-Murley score. Clin Orthop Relat Res. 2010;468:1565–1571. doi: 10.1007/s11999-009-1007-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bankes MJ, Crossman JE, Emery RJ. A standard method of shoulder strength measurement for the Constant score with a spring balance. J Shoulder Elbow Surg. 1998;7:116–121. doi: 10.1016/s1058-2746(98)90220-8. [DOI] [PubMed] [Google Scholar]
- 15.Walton MJ, Walton JC, Honorez LA, Harding VF, Wallace WA. A comparison of methods for shoulder strength assessment and analysis of Constant score change in patients aged over fifty years in the United Kingdom. J Shoulder Elbow Surg. 2007;16:285–289. doi: 10.1016/j.jse.2006.08.002. [DOI] [PubMed] [Google Scholar]
- 16.van Kampen DA, van Beers LW, Scholtes VA, Terwee CB, Willems WJ. Validation of the Dutch version of the Simple Shoulder Test. J Shoulder Elbow Surg. 2012;21:808–814. doi: 10.1016/j.jse.2011.09.026. [DOI] [PubMed] [Google Scholar]
- 17.Constant CR, Gerber C, Emery RJ, Søjbjerg JO, Gohlke F, Boileau P. A review of the Constant score: modifications and guidelines for its use. J Shoulder Elbow Surg. 2008;17:355–361. doi: 10.1016/j.jse.2007.06.022. [DOI] [PubMed] [Google Scholar]
- 18.Dawson J, Rogers K, Fitzpatrick R, Carr A. The Oxford shoulder score revisited. Arch Orthop Trauma Surg. 2009;129:119–123. doi: 10.1007/s00402-007-0549-7. [DOI] [PubMed] [Google Scholar]
- 19.Dawson J, Hill G, Fitzpatrick R, Carr A. The benefits of using patient-based methods of assessment. Medium-term results of an observational study of shoulder surgery. J Bone Joint Surg Br. 2001;83:877–882. doi: 10.1302/0301-620x.83b6.11316. [DOI] [PubMed] [Google Scholar]
- 20.Olley LM, Carr AJ. The use of a patient-based questionnaire (the Oxford Shoulder Score) to assess outcome after rotator cuff repair. Ann R Coll Surg Engl. 2008;90:326–331. doi: 10.1308/003588408X285964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Desai AS, Dramis A, Hearnden AJ. Critical appraisal of subjective outcome measures used in the assessment of shoulder disability. Ann R Coll Surg Engl. 2010;92:9–13. doi: 10.1308/003588410X12518836440522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moser JS, Barker KL, Doll HA, Carr AJ. Comparison of two patient-based outcome measures for shoulder instability after nonoperative treatment. J Shoulder Elbow Surg. 2008;17:886–892. doi: 10.1016/j.jse.2008.05.040. [DOI] [PubMed] [Google Scholar]
- 23.Frich LH, Noergaard PM, Brorson S. Validation of the Danish version of Oxford Shoulder Score. Dan Med Bull. 2011;58:A4335. [PubMed] [Google Scholar]
- 24.Slobogean GP, Noonan VK, O’Brien PJ. The reliability and validity of the Disabilities of Arm, Shoulder, and Hand, EuroQol-5D, Health Utilities Index, and Short Form-6D outcome instruments in patients with proximal humeral fractures. J Shoulder Elbow Surg. 2010;19:342–348. doi: 10.1016/j.jse.2009.10.021. [DOI] [PubMed] [Google Scholar]
- 25.Huisstede BM, Feleus A, Bierma-Zeinstra SM, Verhaar JA, Koes BW. Is the disability of arm, shoulder, and hand questionnaire (DASH) also valid and responsive in patients with neck complaints. Spine (Phila Pa 1976) 2009;34:E130–E138. doi: 10.1097/BRS.0b013e318195a28b. [DOI] [PubMed] [Google Scholar]
- 26.Bilberg A, Bremell T, Mannerkorpi K. Disability of the Arm, Shoulder and Hand questionnaire in Swedish patients with rheumatoid arthritis: A validity study. J Rehabil Med. 2012;44:7–11. doi: 10.2340/16501977-0887. [DOI] [PubMed] [Google Scholar]
- 27.Jianmongkol S, Kosuwon W, Thammaroj T, Boonard M. Validity of the Thai version of Disability of the Arm, Shoulder and Hand Questionnaire (KKU-DASH) in patients with brachial plexus injury. J Med Assoc Thai. 2011;94:71–77. [PubMed] [Google Scholar]
- 28.Roy JS, Macdermid JC, Faber KJ, Drosdowech DS, Athwal GS. The simple shoulder test is responsive in assessing change following shoulder arthroplasty. J Orthop Sports Phys Ther. 2010;40:413–421. doi: 10.2519/jospt.2010.3209. [DOI] [PubMed] [Google Scholar]
- 29.Godfrey J, Hamman R, Lowenstein S, Briggs K, Kocher M. Reliability, validity, and responsiveness of the simple shoulder test: psychometric properties by age and injury type. J Shoulder Elbow Surg. 2007;16:260–267. doi: 10.1016/j.jse.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 30.Neto JO, Gesser RL, Steglich V, Bonilauri Ferreira AP, Gandhi M, Vissoci JR, Pietrobon R. Validation of the Simple Shoulder Test in a Portuguese-Brazilian population. Is the latent variable structure and validation of the Simple Shoulder Test Stable across cultures? PLoS One. 2013;8:e62890. doi: 10.1371/journal.pone.0062890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Marchese C, Cristalli G, Pichi B, Manciocco V, Mercante G, Pellini R, Marchesi P, Sperduti I, Ruscito P, Spriano G. Italian cross-cultural adaptation and validation of three different scales for the evaluation of shoulder pain and dysfunction after neck dissection: University of California - Los Angeles (UCLA) Shoulder Scale, Shoulder Pain and Disability Index (SPADI) and Simple Shoulder Test (SST) Acta Otorhinolaryngol Ital. 2012;32:12–17. [PMC free article] [PubMed] [Google Scholar]
- 32.Michener LA, McClure PW, Sennett BJ. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: reliability, validity, and responsiveness. J Shoulder Elbow Surg. 2002;11:587–594. doi: 10.1067/mse.2002.127096. [DOI] [PubMed] [Google Scholar]
- 33.Bafus BT, Hughes RE, Miller BS, Carpenter JE. Evaluation of utility in shoulder pathology: Correlating the American Shoulder and Elbow Surgeons and Constant scores to the EuroQoL. World J Orthop. 2012;3:20–24. doi: 10.5312/wjo.v3.i3.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kirkley A, Griffin S, Dainty K. Scoring systems for the functional assessment of the shoulder. Arthroscopy. 2003;19:1109–1120. doi: 10.1016/j.arthro.2003.10.030. [DOI] [PubMed] [Google Scholar]
- 35.Salomonsson B, Ahlström S, Dalén N, Lillkrona U. The Western Ontario Shoulder Instability Index (WOSI): validity, reliability, and responsiveness retested with a Swedish translation. Acta Orthop. 2009;80:233–238. doi: 10.3109/17453670902930057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hatta T, Shinozaki N, Omi R, Sano H, Yamamoto N, Ando A, Sugaya H, Aizawa T, Kuriyama S, Itoi E. Reliability and validity of the Western Ontario Shoulder Instability Index (WOSI) in the Japanese population. J Orthop Sci. 2011;16:732–736. doi: 10.1007/s00776-011-0141-4. [DOI] [PubMed] [Google Scholar]
- 37.University of Sheffield. SF-6D. 2013. Available from: http:// www.shef.ac.uk/scharr/sections/heds/mvh/sf-6d. [Google Scholar]
- 38.Barrack RL, McClure JT, Burak CF, Clohisy JC, Parvizi J, Hozack W. Revision total hip arthroplasty: the patient’s perspective. Clin Orthop Relat Res. 2006;453:173–177. doi: 10.1097/01.blo.0000246537.67500.50. [DOI] [PubMed] [Google Scholar]
- 39.Marx RG, Jones EC, Atwan NC, Closkey RF, Salvati EA, Sculco TP. Measuring improvement following total hip and knee arthroplasty using patient-based measures of outcome. J Bone Joint Surg Am. 2005;87:1999–2005. doi: 10.2106/JBJS.D.02286. [DOI] [PubMed] [Google Scholar]
- 40.O’Holleran JD, Kocher MS, Horan MP, Briggs KK, Hawkins RJ. Determinants of patient satisfaction with outcome after rotator cuff surgery. J Bone Joint Surg Am. 2005;87:121–126. doi: 10.2106/JBJS.C.01316. [DOI] [PubMed] [Google Scholar]
- 41.Scott MA, Neumann L, Wallace WA. Agreement between the Constant Score and the Oxford Shoulder Score. 2007. [Google Scholar]
- 42.Amadio PC. Outcomes measurements. J Bone Joint Surg Am. 1993;75:1583–1584. doi: 10.2106/00004623-199311000-00001. [DOI] [PubMed] [Google Scholar]
- 43.Skutek M, Fremerey RW, Zeichen J, Bosch U. Outcome analysis following open rotator cuff repair. Early effectiveness validated using four different shoulder assessment scales. Arch Orthop Trauma Surg. 2000;120:432–436. doi: 10.1007/s004020000133. [DOI] [PubMed] [Google Scholar]
- 44.Lewis JS. A specific exercise program for patients with subacromial impingement syndrome can improve function and reduce the need for surgery. J Physiother. 2012;58:127. doi: 10.1016/S1836-9553(12)70093-0. [DOI] [PubMed] [Google Scholar]
- 45.Dawson J, Doll H, Boller I, Fitzpatrick R, Little C, Rees J, Carr A. Specificity and responsiveness of patient-reported and clinician-rated outcome measures in the context of elbow surgery, comparing patients with and without rheumatoid arthritis. Orthop Traumatol Surg Res. 2012;98:652–658. doi: 10.1016/j.otsr.2012.05.011. [DOI] [PubMed] [Google Scholar]
- 46.van de Water AT, Shields N, Davidson M, Evans M, Taylor NF. Reliability and validity of shoulder function outcome measures in people with a proximal humeral fracture. Disabil Rehabil. 2014;36:1072–1079. doi: 10.3109/09638288.2013.829529. [DOI] [PubMed] [Google Scholar]
- 47.Wallace WA, Thyagarajan D, Gooding BWT, Johnson G, Kontaxis A, Kocsis G, Scott M, Blacknall J, Edwards K. Early outcomes from the Vaios dual platform total shoulder replacement - anatomic & inverse or reverse. Shoulder and Elbow: 2015. p. Submitted for publication. Available from: http: //sel.sagepub.com/ [Google Scholar]