

Abstract
Background
An artificial disc prosthesis is thought to restore segmental motion in the lumbar spine. However, it is reported that disc prosthesis can increase the intervertebral translation (VT). The concept of the mobile-core prosthesis is to mimic the kinematic effects of the migration of the natural nucleus and therefore core mobility should minimize the VT. This study explored the hypothesis that core translation should influence VT and that a mobile core prosthesis may facilitate physiological motion.
Methods
Vertebral translation (measured with a new method presented here), core translation, range of motion (ROM), and distribution of flexion-extension were measured on flexion-extension, neutral standing, and lateral bending films in 89 patients (63 mobile-core [M]; 33 fixed-core [F]).
Results
At L4-5 levels the VT with M was lower than with F and similar to the VT of untreated levels. At L5-S1 levels the VT with M was lower than with F but was significantly different compared to untreated levels. At M levels a strong correlation was found between VT and core translation; the VT decreases as the core translation increases. At F levels the VT increases as the ROM increases. No significant difference was found between the ROM of untreated levels and levels implanted with either M or F. Regarding the mobility distribution with M and F we observed a deficit in extension at L5-S1 levels and a similar distribution at L4-5 levels compared to untreated levels.
Conclusion
The intervertebral mobility was different between M and F. The M at L4-5 levels succeeded to replicate mobility similar to L4-5 untreated levels. The M at L5-S1 succeeded in ROM, but failed regarding VT and mobility distribution. Nevertheless M minimized VT at L5-S1 levels. The F increased VT at both L4-5 and L5-S1.
Clinical Relevance
This study validates the concept that the core translation of an artificial lumbar disc prosthesis minimizes the VT.
Keywords: Lumbar segmental motion, Mobile-core prosthesis, Fixed-core prosthesis, Translation measurement method
Introduction
The goal of the lumbar disc prosthesis is to restore physiological segmental motion at the operative levels, and consequently, to prevent posterior facet degradation and adjacent segment disease. However, it is reported that disc prosthesis placement could provide unnatural kinematics including a decrease of sagittal range of motion, 1, 2 a disturbance of flexion-extension distribution,1 and also an abnormal increase of axial rotation.3, 4 Some authors5 reported an increase of the intervertebral translation (VT) during flexion-extension, which consequently may increase load on the facet joints and may generate arthritic progression. This report5 involved different prosthesis designs providing different amounts of excess VT occurring with sagittal rotation.
There are several total disc replacements that have been designed and are in various stages of testing and clinical use.6, 7 Among the different designs is the mobile-core prosthesis. The concept of the mobile-core prosthesis is to mimic the kinematic effects of the migration of the natural nucleus. The mobile-core designs do not constrain the center of rotation to a fixed point. The locus of points that define the different instantaneous centers of rotation can be theoretically replicated. Therefore, core mobility should minimize the VT because the natural migration of the nucleus minimizes the VT and core mobility replicates the natural migration of the nucleus.
For the fixed-core designs, meaning ball-and-socket configurations, the center of rotation is fixed and corresponds to the geometric center of the ball. The amount of VT occurring with rotation in the sagittal plane depends on the radius of curvature of the ball. In the frontal plane (during lateralbending), frontal rotation and axial rotation and axial VT are coupled as the axial center of rotation is posterior to the disc space close to the facet joints.8 With core-translation (allowing axial VT), the coupled motion of frontal rotation and axial rotation should be facilitated
The goal of this study was to assess the concept that core translation in a lumbar artificial disc should influence VT and may facilitate physiological intervertebral mobility replication in both the sagittal and frontal planes. Radiologic intervertebral motion characteristics of levels implanted with mobile-core prosthesis were compared to (a) levels treated by fixed-core prosthesis, (b) to adjacent untreated levels, and (c) to normative data from literature.9
Materials and methods
Radiologic assessment was performed in 63 patients who received at a single level (L4-5 or L5-S1) a mobile-core prosthesis (Mobidisc; LDR Médical, Troyes, France) and in 33 patients who received a fixed-core prosthesis (Pro- Disc-L; Synthes Spine, West Chester, Pennsylvania). The mean duration of follow-up was 30 months for the mobilecore prosthesis group and 25 months for the fixed-core prosthesis group. Both devices feature a core made of polyethylene and cobalt-chrome metal endplates.
Sagittal VT, core translation, sagittal and frontal range of motion (ROM), and distribution of flexion-extension were measured on flexion-extension, neutral standing, and lateral bending films. The analysis of X-rays was computer-assisted (SpineView software; SurgiView, Paris, France).5 The measure of the translation of the mobile-core was possible because of the presence of a metal marker inserted inside the core. A method of sagittal VT measurement adapted from the Frobin's method9 was developed to optimize the accuracy of the measurements. Metal markers (eg, the edges of the prosthesis endplates) were used instead of the bony landmarks. The middles of the vertebral bodies were substituted by the middles of the prosthesis endplates (Fig. 1) and the intervertebral translation was assimilated to the translation between the superior and inferior prosthesis endplates. The incidence (orthogonal) was maintained between flexion-films and extension films, and therefore the length of the keels (easy to measure on the sharp teeth) should be the same. If not, the sagittal dynamic X-rays were not included in the analysis.
Fig. 1.
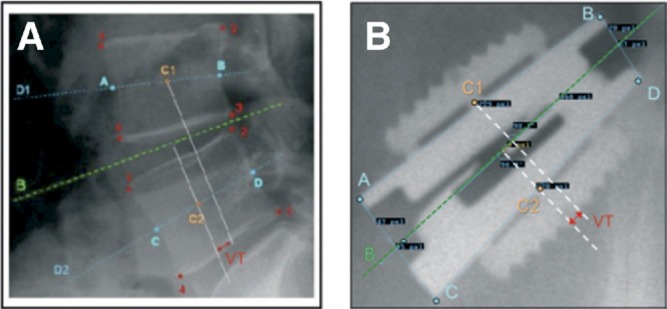
Sagittal vertebral translation measurement method. (A) The wellaccepted method of Frobin was adapted (B) to total disc arthroplasty. Metal markers (the edges of the prosthesis endplates) were used instead of the bony landmarks. The middle of the vertebral bodies (C1 and C2) were substituted by the middle of the prosthesis endplates. The intervertebral translation (TV) was replaced by the translation between the superior and inferior prosthesis endplates.
In the standard Frobin's method,9 VT is expressed as a percentage of the vertebral endplate per degree of rotation. In our study, as the sizes of the prosthesis were known, pixels could be calibrated and VT was able to be expressed in millimeters. With regard to normative data from literature, 9 which were given in percentage, VT was transformed to millimeters using the mean value of the endplate length of vertebrae implanted in our study (33 mm). Normal values were obtained from radiographs of 61 symptom-free volunteers. All the results of VT were adjusted to 10° of ROM in order to be able to compare the amount of VT between each group for the same ROM.
Special radiologic incidence was used to try to assess the axial VT at levels implanted with mobile-core prosthesis (Fig. 2) because frontal rotation during lateral bending includes an axial rotation component, and therefore axial VT (achieved by mobile core translation) could be observed.
Fig. 2.

Axial translation between mobile-core prosthesis endplates during lateral bending. (A) Antero-posterior oblique incidence was developed to obtain an equivalence of superior view of the prosthesis endplates (B) in the right and (C) the left lateral bending. (D) (E) An other example with an increase of contrast to better differentiate the superior endplate from the inferior endplate to illustrate the axial translation between the two endplates.
To evaluate reproducibility in the VT measurement, 36 flexion-extension films were analyzed by 3 different observers. Interobserver reliability of the VT measurement method was assessed by calculating the intraclass correlation coefficient (ICC).10 To approximate the interobserver precision, the difference between the measurements of the 3 observers was determined for each measurement occasion. The standard deviation of these differences were calculated (N = 36 × 3). Precision was defined as the mean of the absolute differences between measurements.11
Results
Sagittal plane
The assessment of the reliability of the VT measurement method developed in this study shows that there was no significant difference between the 3 observers (P < .001) and that the level of agreement was rather high as the ICC was 0.908. The interobserver precision corresponding to the mean absolute difference between observers was 0.2 mm.
Table 1 reports the VT at different levels with different configurations. At L4-5 levels the VT with a mobile-core (−1.1 mm) was significantly lower than with a fixed-core (−1.74 mm) and similar to the VT of untreated levels (−1.2 mm) and normal levels (−1.03 mm). At implanted L5-S1 levels the VT with a mobile-core (−0.79 mm) was still significantly lower than with a fixed core (−1.58 mm) but was also significantly different than untreated levels (+1.07 mm) and normal levels (+0.03 mm). The VT at L4-5 levels with mobile-core was significantly higher (in absolute value) than VT at L5-S1 levels with mobile core (P = .002). With the fixed-core prosthesis, the VT was higher than either the normal levels (significantly P < .001) or untreated levels (not significantly P = .08). Overall, the mobile-core prosthesis better replicated normal spine VT compared to the fixed core prosthesis.
Table 1.
Vertebral translation at normal levels (data from literature), untreated levels (below or above treated levels), mobile-core implanted levels and fixed-core implanted levels
| Levels | L2-3 | L3-4 | L4-5 | L5-S1 | Difference* between levels |
|---|---|---|---|---|---|
| Normal | −1.07 ± 0.46 n = 59 | −1.22 ± 0.60 n = 58 | −1.03 ± 0.48 n = 49 | +0.03 ± 0.97 n = 37 | |
| Untreated | −1.15 ± 1.12 n = 36 | −1.29 ± 1.02 n = 41 | −1.20 ± 1.28 n = 29 | −1.07 ± 1.61 n = 17 | |
| Mobile-core | −1.10 ± 0.59 n = 21 | −0.79 ± 0.44 n = 35 | ML4L5 versus ML5S1 p = 0.002 | ||
| Fixed-core | −1.74 ± 0.71 n = 15 | −1.61 ± 0.45 n = 18 | FL4L5 versus FL5S1 NS | ||
| Difference* between groups | N versus U NS |
N versus U NS |
N versus U NS N versus M NS N versus F P < .001 U versus M NS U versus F NS P = .08 M versus F P < .001 |
N versus U P = .02 N versus M P < .001 N versus F P < .001 U versus M P < .001 U versus F P < .001 M versus F P < .001 |
Abbreviations: n, number of cases available; N, normal levels; U, untreated levels; M, mobile-core implanted levels; F, fixed-core implanted levels; NS, not significant (P > .05)
The Wilcoxon test was used to compare U and M and F. The Student's test was used to compare N to all the other levels. Vertebral translation is expressed in millimeters for 10° of range of motion. Means ± standard deviation are shown.
The mean core translation was calculated by cumulating L4-5 and L5-S1 implanted levels and 1.12 ± 0.8 mm. No relation was found between the amount of core translation and the postoperative implanted segment lordosis (Fig. 3).
Fig. 3.

Relation between core translation (in millimeters) and implanted segment lordosis (in degrees) with mobile-core prosthesis.
At levels implanted with a mobile-core prosthesis no correlation was found between VT and ROM nor between core translation and ROM. A strong correlation was found between VT and core translation; the VT decreases as the core translation increases (r = .7619; P < .0001) (Fig. 4). At levels implanted with a fixed-core prosthesis the VT increases as the ROM increases (P < 0.05) (Fig. 5).
Fig. 4.

Relation between core translation (in millimeters) and vertebral translation (in millimeters) with mobile-core prosthesis. The vertebral translation decreases as the core translation increases.
Fig. 5.

Relation between vertebral translation (in millimeters) and ROM (in degrees) with fixed-core prosthesis.
Sagittal ROM and mobility distribution are reported in Figure 6. The ROM at levels implanted with a mobile-core prosthesis were higher (but not significantly) at both L4-5 and L5-S1 levels compared to levels implanted with a fixedcore prosthesis: 10.3° ± 5 and 6.9° ± 3.5 at L4-5 levels and 8.9° ± 3.9 and 6.4° ± 3.8 at L5-S1 levels. No significant difference was found between the ROM of untreated levels and levels implanted with a mobile-core prosthesis. Regarding the mobility distribution at L4-5 and L5-S1 implanted levels compared to normal levels, we observed a deficit predominating in extension for both the mobile-core and the fixed-core prosthesis. In opposition, a similar distribution was observed between L4-5 untreated levels and L4-5 levels treated with a mobile-core prosthesis (without deficit in extension).
Fig. 6.

Range and distribution of motion at L5-S1, L4-5, and L3-4 levels for normal (data from literature), untreated (adjacent to treated levels), implanted with a mobile-core prosthesis, and implanted with a fixed-core prosthesis levels. For untreated levels and implanted levels with a mobile-core prosthesis, the range of motion in flexion and in extension (lightest gray area) are differentiated.
Frontal plane
The special incidence used to assess axial VT of the prosthesis endplates is shown in Figure 2. Axial VT seemed to be obvious in a few cases, but overall the small range of segmental axial VT prohibited measurements. Furthermore, the frontal translation of the core was also not measurable in this plane because of the combined axial rotation which generated errors in the location of the metal marker inside the core. However, some X-rays seemed to show the frontal displacement to the metal marker (Fig. 7). The mean frontal ROM were 4.15° ± 2.8 at L4-5 and 3.01° ± 2.5 at L5-S1 levels implanted with a mobile-core prosthesis. On lateral bending we observed, in a few cases, where segmental tilting in the frontal plane at the implanted level was opposite to the whole of the lumbar spine (Fig. 7). At levels implanted with a mobile-core prosthesis no correlation was found between sagittal core translation and frontal ROM.
Fig. 7.

Two examples of lateral bending assessment with mobile-core prosthesis showing two different tilting directions at implanted levels compared to the tilting direction of the whole lumbar spine. (A) An operated segment tilting opposite to the whole lumbar spine tilting and (B) in the same direction. Blue arrow indicates the metal marker inside the core. Lateral bending films (A) and (B) also illustrate two different frontal displacements of the metal marker.
Discussion
This study revealed that intervertebral mobility was different between levels implanted with a mobile-core than with a fixed-core prosthesis and validated the concept that the prosthesis core translation better replicates normal vertebral translation.
The main results of the current study focusing on VT are based on an adaptation of the well-accepted Frobin's method to total disc arthroplasty. The adapted method provided a high accuracy (0.2 mm of interobserver precision) and a strong reliability (ICC = 0.908) as the metal landmarks substituted by bony landmarks are accurate. Other authors reached the same accuracy for sagittal translatory motion (0.2 mm) with a very precise technique: roentgen stereophotogrammetric analysis. 12, 13 Also, Ordway et al. applied this technique to measure motion following intervertebral disc replacement with an accuracy of 100 micrometers in translation.14 This work, analyzing the VT of a fixed-core prosthesis, revealed an increase compared to normal physiology: 2.4 mm for 6.3° of ROM.14 The metal markers implanted for the roentgen stereophotogrammetric method could correspond to the sharp metal angular limits of the endplates and keels of the disc prosthesis. The principle to use the metal limits of prosthesis as markers to increase the accuracy of the measurements was also validated in the assessment of ROM of total disc replacement.11, 15
The VT (adjusted to 10° of ROM) of L2-3 and L3-4 and L4-5 untreated levels in the present study were similar to corresponding reference normal levels9 and to untreated levels as reported in other studies.1 This suggests that untreated levels could be used as reference levels to compare the treated levels within the same population.
At mobile-core implanted L4-5 levels, the VT can be described as “physiologic” because no significant differences were found in comparison to the VT of untreated levels and normal levels. At mobile-core implanted L5-S1 levels, VT was significantly different than either untreated L5-S1 levels or normal L5-S1 levels. Thus, at the L5-S1 level the mobile-core disc implantation failed to restore physiologic VT. Finally, mobile-core L4-5 VT was significantly higher than the mobile-core L5-S1 VT as in physiology (normal L4-5 VT is higher than normal L5-S1 VT).9
Comparison with the fixed-core prosthesis revealed that, at both L4-5 and L5-S1 levels, VT with mobile-core prosthesis was significantly lower. Furthermore, fixed-core VT was also higher at both L4-5 and L5-S1 levels compared to normal levels (significantly) and untreated levels (significantly only at the L5-S1 level). Finally, no differences were observed between VT at L4-5 land L5-S1 levels implanted with a fixed-core prosthesis. Consequently, it can be concluded that a fixed-core prosthesis did not replicate physiologic VT at any level. Long-term clinical consequences of the increase VT on facet joints after total disc replacement is still questionable.6, 16 Most of the papers describe an increased of the facet loads after total disc replacement but with some contrasting results.6, 7 Moumene et al. reported in an experimental work that a mobile-core prosthesis reduced facet loading compared with a fixed-core design.17
This study showed that the majority of the core was effectively mobile. A mean amount of motion equal to 1.12 ± 0.8 mm was observed for a design that allows 2.5 mm multidirectional translation between flat surfaces of the inferior part of the core and the superior part of the inferior prosthesis endplate. Translation is limited because of the presence of stops at the level of the inferior prosthesis endplate. The translation of the core did not appear to be affected by the postoperative treated segment lordosis. The strong correlation found between VT and core translation was that the VT decreases as the core translation increases. This demonstrated that the core mobility minimizes the intervertebral mobility. Also, this study confirmed that core mobility allowed a moving center of rotation during flexion-extension intervertebral motion, as expected. Furthermore, the absence of relation between VT and sagittal ROM indirectly confirmed that the axis of rotation moved during the flexion-extension intervertebral displacement. The VT increased proportionally to the ROM with a fixed-core prosthesis, which is logical because the center of rotation is fixed.
The reported amount of ROM at treated levels after total disc replacement is indeed variable among the literature.6 Nevertheless, in the current study no statistical difference was observed between treated levels (either with a mobile-core or a fixed-core prosthesis) and untreated levels which could be established as a reference. However, if the reference is the population called normal composed of healthy symptom free volunteers results exhibited a decrease in ROM.9 Again, adjacent untreated levels in the same population seem to be a better adapted reference as this population generally still continue to feel some low-back pain after surgery and still fair well to perform maximum flexion and extension during the dynamic film procedure. Also, regarding the mobility distribution, interpretation depends on the reference population. At L4-5 and L5-S1 implanted levels, compared to normal distribution, we observed a deficit predominating in extension for both the mobile-core and the fixed-core prostheses. This deficit in extension with respect to normal distribution appeared stronger at the L5-S1 level. Some authors found an opposite deficit in flexion with the same type of fixed-core prosthesis at the L4-5 level and a deficit in extension as well as in flexion at the L5-S1 level.1 The design appears to be not the only parameter which systematically influences the domain of deficit in motion distribution.
In contrast, in the current study a similar distribution was observed between L4-5 untreated levels and L4-5 levels treated with the mobile-core prosthesis. With regard to reference population comparison with other works of our untreated levels, motion distribution revealed similar distribution at adjacent levels L3-4 and L2-3.1 At all levels qualified as untreated from L2 to S1 the disc were nonpathologic, which supports the principle to choose untreated levels as reference levels.
Axial VT seemed to be obvious on some special radiologic incidences (Fig. 2) but it happened in few cases and the small range of segmental axial VT prohibited measurements. Furthermore, the frontal translation of the core was also not measurable in this plane because of the combined axial rotation which generated errors in the location of the metal marker inside the core. However, some X-rays seemed to show the frontal displacement of the metal marker (Fig. 7). Lateral bending films were only available for the mobile-core prosthesis. The mean frontal ROM were 4.2° ± 2.8 at L4-5 and 3.0° ± 2.5 at the L5-S1 levels implanted with the mobile-core prosthesis. On lateral bending, segmental paradoxical frontal motion was observed in few cases: the segmental frontal tilting at the implanted level was opposite to the whole tilting of the lumbar spine (Fig. 7). Finally, no correlation was found between frontal ROM and sagittal core translation.
Cadaveric and clinical studies showed that the lateral bending is a complex motion accompanied by axial rotation coupled to axial translation and sagittal flexion.4, 8, 18 The concept of the mobile-core postulates that the possibility of multidirectional translation for the core should facilitate the lateral bending because axial VT is permitted.
Our study confirmed the possibility of axial VT between the two prosthesis endplates but failed to quantify it because of the coupling 3D motions. The quantification of the core translation in the frontal plan was also not possible because of the coupling 3D motions providing errors in image analysis. In theory, frontal ROM and axial VT should be related: when frontal ROM increases axial VT should increase. As axial core translation was not measurable, a relation was sought between frontal ROM and sagittal core translation with the hypothesis that more mobility of the core in the sagittal plane could be related to more mobility in the frontal plane. No relation was found.
Few papers deal with frontal ROM restoration after total disc replacement.14, 19 Compared to normal physiology (mean frontal ROM: 8.3°)20, mainly decreased frontal ROM was observed after total disc replacement.14, 19 Comparing with other studies, frontal ROM of the mobile-core prosthesis of the present study (4.2° at L4-5 levels and 3° at L5-S1 levels) were slightly higher than the amount reported by Ordway et al.14 with a fixed-core prosthesis (between 3° and 4° at L4-5 levels and around 1° at L5-S1 levels) and slightly lower than those reported by Lemaire et al.19 with a different type of mobile-core prosthesis design (mean 5.4°).
Conclusion
This in vivo study revealed that intervertebral mobility was different between levels implanted with a mobile-core prosthesis than with a fixed-core prosthesis. This study proposes to choose the healthy adjacent untreated levels within the same operated population as the reference lumbar segments. The mobile-core prosthesis at L4-5 levels succeeded to replicate mobility similar to L4-5 untreated levels including VT, sagittal ROM, and mobility distribution but failed at L5-S1 levels regarding VT and mobility distribution. These conclusions suggest that the L5-S1 level could need a specific disc arthroplasty design. Nevertheless, core mobility minimized VT even at L5-S1 levels. The fixed-core prosthesis increased VT at both L4-5 and L5-S1 levels. The long-term consequences of the differing kinematics (including the increase of VT) on clinically important outcomes such as low-back pain and facet arthritis have yet to be determined.
Extended references
Mobility of lumbar segments instrumented with a ProDisc II prosthesis – A two-year follow-up study.
Leivseth G, Braaten S, Frobin W, Brinckmann P.
STUDY DESIGN: Longitudinal prospective study on a sample of 41 consecutive disc prosthesis patients, covering a postoperative time period of at least 2 years. OBJECTIVES: To document the rotational and translational range of segmental motion of patients instrumented with ProDisc II prostheses in the lumbar spine and to compare motion between instrumented and untreated adjacent segments with respect to a normative database. To discuss potential causes of the low range of rotational motion observed after instrumentation with a Prodisc II prosthesis. SUMMARY OF BACKGROUND DATA: Disc replacement is intended to restore physiologic motion and height of the affected levels. Published reports show, however, that the goal of restoring motion at the operated segment is missed in the majority of cases. The cause of this failure is unresolved. METHODS: Rotational and translational segmental motion in the sagittal plane, disc height, and posteroanterior displacement were measured from lateral radiographic views taken standing (before surgery) and in flexion and extension (1 year and 2 years after surgery) by Distortion Compensated Roentgen Analysis (DCRA). The protocol permits to take measurements from all segments imaged on the radiographic views and compensates for variations in stature, magnification, and posture. Data from instrumented and untreated segments can be compared and related to a previously determined normative database. RESULTS: The rotational range of motion of segments instrumented with a ProDisc II prosthesis was low, especially at L4-L5 and L5-S1. In the majority of cases, it amounted to less than 45% of the normal range. Virtually no improvement occurred between 1 and 2 years after surgery. Malalignment of the axis of rotation of the prosthesis with respect to the anatomic axis, persisting clinical symptoms, or the significant increase of intervertebral space documented after instrumentation are unlikely to cause the low range of motion. As the range of rotational motion of the untreated segments was low with respect to normal as well, it is conjectured that tissue adaptation during the preoperative symptomatic time period might have caused the postoperative motion deficit. This conjecture complies with fragmentary previous observations of a low postoperative segmental range of motion from untreated segments of fusion patients. CONCLUSIONS: Disc replacement in the lumbar spine by a ProDisc II implant fails to restore normal segmental rotational motion in the sagittal plane, specifically at levels L4-L5 and L5-S1. As segmental motion of the untreated segments was lower than normal as well, though not quite as conspicuous as that of instrumented segments, adaptation of soft tissue taken place during the preoperative symptomatic time period is conjectured to cause the observed motion deficit. Postoperative physical therapy might be considered if restoration of a normal range of rotational motion is desired.
Total disc arthroplasty: consequences for sagittal balance and lumbar spine movement.
Tournier C, Aunoble S, Le Huec JC, Lemaire JP, Tropiano P, Lafage V, Skalli W.
This in vivo biomechanical study was undertaken to analyze the consequences for sagittal balance and lumbar spine movement in three different lumbar disc prostheses. A total of 105 patients underwent total disc replacement in three different centers. The Maverick prosthesis was used in 46 patients, the SB Charité device was used in 49 patients and the Prodisc device was utilized in 10 patients. The analysis was computer assisted, using Spineview and Matlab softwares. The intra and inter-observer reliability and measurement uncertainty was performed. The analysis of lateral X-ray films in flexion-extension allowed to measure the prosthesis positioning, the range of motion (ROM), the localization of the mean center of rotation (MCR), the vertebral translation and the disc height, for each prosthesis device. The sagittal balance was analyzed on a full spine film. The parameters studied were described by Duval- Beaupère. The results were compared to the data found in literature, and compared to 18 asymptomatic volunteers, and 61 asymptomatic subjects, concerning the sagittal balance. The prostheses allowed an improvement of the ROM of less than 2 degrees. The ROM of L5-S1 prostheses ranged from 11.6 to 15.6% of the total lumbar motion during flexion-extension. At L4-L5 level, the ROM decreased when there was an arthrodesis associated at the L5-S1 level. There was no difference of ROM between the three prostheses devices. The MCR was linked to the ROM, but did not depend on the prosthesis offcentering. The disc height improved for any prosthesis, and decreased in flexion or in extension, when the prosthesis was offcentered. An increase of translation indicated a minor increase of the ROM at L4-L5 level after Maverick or SB Charité implantation. The L5-S1 arthrodesis was linked with an increase of the pelvic tilt. The lumbar lordosis curvature increased between L4 and S1, even more when a prosthesis was placed at the L3-L4 level. Total disc arthroplasty is useful in the surgical management of discogenic spinal pathology. The three prostheses studied allowed to retorate the disc height, the ROM, without disrupting the sagittal balance, but induced modification of the lumbar curvature.
Precision measurement of disc height, vertebral height and sagittal plane displacement from lateral radiographic views of the lumbar spine.
Frobin W, Brinckmann P, Biggemann M, et al.
OBJECTIVE.: To compile a database of disc height, vertebral height and sagittal plane displacement from lateral radiographic views of the lumbar spine, valid for male and female subjects in the age range 16–57 years. The protocols used to measure these parameters compensate for distortion in central projection, off-centre position, axial rotation and lateral tilt of the spine as well as for variation in radiographic magnification and stature. STUDY DESIGN.: The study comprised designing and testing of measurement protocols, together with subsequent data collection from archive radiographs. BACKGROUND.: Attempts to quantify primary mechanical damage to lumbar vertebrae and discs have been limited due to imprecision when measuring disc height, vertebral height and sagittal plane displacement. Age-related, normative values for these parameters were not previously available. Consequently, important issues like the effectiveness of past and present guidelines for safe manual handling with respect to prevention of overload injuries could not be resolved and judgement on pathological alterations in the morphology of the individual lumbar spine could only be performed in a qualitative, subjective manner. METHODS.: Based on the analysis of vertebral contours in the lateral radiographic image of the lumbar spine, new protocols for measuring disc height, vertebral height and sagittal plane displacement were developed. The measured data are virtually independent of distortion, axial rotation and lateral tilt. Furthermore, description of height and displacement using dimensionless parameters guarantees independence of radiographic magnification and stature. Subjective influence in the measurement procedure was minimized by automatic computation of contour-landmarks and derived parameters. Measurement errors were assessed from sets of radiographs of spine specimens and serial flexion-extension radiographs; interobserver and intraobserver errors were assessed from repeated measurements of lateral views. For compilation of a database, measurements were performed of a set of 892 lateral views of the lumbar spine of male and female subjects between 16 and 57 years of age. Data from pathologically deformed vertebrae or discs, or from motion segments exhibiting spondylolisthesis or retrolisthesis were excluded by normal radiological inspection; data from spines showing normal, agerelated degenerative changes were included. RESULTS.: The new protocols allow height and displacement of lumbar vertebrae as well as height of lumbar discs to be measured for all motion segments on a lateral view, rather than just those vertebrae or discs close to the central beam, to facilitate recognition of localized abnormalities. Since the results are independent of exposure geometry, retrospective investigations are feasible. The relative measurement error in vertebral height amounts to 2.2%; for a vertebra of 30 mm height this corresponds to an error of approximately 0.7 mm. The error in sagittal plane displacement amounts to 0.015 (measured in units of mean vertebral depth); for a vertebra of 35 mm depth this corresponds to an error of 0.5 mm. The relative error in disc height amounts to 4.15%; for a disc of 10 mm height this corresponds to an error of approximately 0.5 mm. For both genders, the database contains age-dependent, normative values of disc height, vertebral height and sagittal plane displacement. In addition, the database describes intersegmental shape correlation, i.e. the relation between height of neighbouring discs and between height as well as displacement of neighbouring vertebrae. On average, height of lumbar vertebrae is larger in females than in males; height of lumbar discs is larger in males than in females and shows a minute dependence on age in males; in both genders, sagittal plane displacement increases, but only by a small amount, with age. CONCLUSIONS.: The new measurement protocols for disc height, vertebral height and sagittal plane displacement, together with the database of normative age-related values, permit quantitative assessment of the prevalence of pathological morphological changes in the human lumbar spine. The new method and the database will serve to explore the effect of potentially detrimental influences such as high spinal loading and to provide quantitative documentation of existing injury to vertebrae and discs in individual cases.
Measurement of total disc replacement radiographic range of motion: a comparison of two techniques.
Lim MR, Girardi FP, Zhang K, Huang RC, Peterson MG, Cammisa FP.
OBJECTIVE: Current methods used to measure total disc replacement (TDR) radiographic range of motion (ROM) have not been previously evaluated. Sagittal ROM is measured by determining the change in the Cobb angle of the prosthesis from the flexion to the extension radiographs. Either the metallic endplates or the keels of the TDR prosthesis can be used as radiographic landmarks in measuring ROM. We hypothesized that use of the prosthesis keels as radiographic landmarks, when compared with the use of prosthesis endplates, might lead to more precise measurements of TDR sagittal ROM. METHODS: Two observers (a fifth-year orthopedics resident and an attending orthopedic spine surgeon) measured the ROM of 51 Prodisc II TDRs on standard flexion and extension lumbar spine radiograph sets. Repeated measurements were made on two occasions using either the keels or the endplates as landmarks. Precision was defined as the mean of the absolute differences between measurements. RESULTS: For observer A, the mean absolute difference between two measurements was 1.4 degrees with the keel method compared with 3.0 degrees with the endplate method (P < 0.001). For observer B, the mean absolute difference between two measurements was 1.8 degrees with the keel method and 3.3 degrees with the endplate method (P < 0.001). When the interobserver differences were examined, the mean absolute difference was 1.8 degrees with the keel method and 3.3 degrees with the endplate method (P < 0.001). CONCLUSIONS: Our results show that the use of TDR prosthesis keels as radiographic landmarks, when compared with the use of prosthesis endplates, yields greater precision in ROM measurement. For TDR prostheses with a keel, we recommend using the keel to measure ROM.
Reliability of motion measurements after total disc replacement: the spike and the fin method.
Cakir B, Richter M, Puhl W, Schmidt R.
As motion preservation is one of the main postulated advantages after total disc replacement (TDR) of the lumbar spine, the quantification of the mobility after TDR seems of special clinical interest. Yet, the best method to assess range of motion (ROM) after TDR remains unclear. The aim of the study was the calculation of 95%-confidence intervals (95%-C.I.) for the measurement error accompanying: (1) different methods (2) different observers and (3) different levels of training for radiographic motion analysis after TDR. In 12 patients the level L4-L5 and in another 12 patients level L5-S1 were measured with the Cobb and the superimposition method on flexionextension X-rays after monosegmental TDR. Both methods were adopted as the landmarks used the spikes of the prosthesis instead the endplates (spike method) and the fin of the prosthesis instead the whole vertebral body (fin method). Measurements were performed by two experienced (O-I and O-III) and one inexperienced observer (O-II). The adopted spike and fin method showed a better reliability compared to the reported results of the original Cobb and superimposition method. The method used was not clinically relevant for the intraobserver reliability in the experienced observer (95%-C.I.: +/− 2.0 degrees for the fin and +/− 2.1 for the spike method) and for the interobserver reliability for two experienced observers (95%-C.I.: −2.8 degrees/ + 2.8 degrees for the fin and −2.9 degrees/ +3.1 degrees for the spike method). The intraobserver reliability for the inexperienced observer was inferior for both methods compared to the experienced observer but no clinically relevant differences could be observed in interobserver reliability measures. The spike and fin method are reliable methods for study protocols dealing with angular motion after TDR as clinically valid conclusions can be drawn with an accuracy of about +/− 2 degrees for the same observer and with an accuracy of about +/− 3 degrees for a different observer.
References
- 1.Leivseth G, Braaten S, Frobin W, Brinckmann P. Mobility of lumbar segments instrumented with a ProDisc II prosthesis: A two-year follow-up study. Spine (Phila Pa 2006) 1976;15:1726–33. doi: 10.1097/01.brs.0000224213.45330.68. [DOI] [PubMed] [Google Scholar]
- 2.McAfee PC, Cunningham BW, Holsapple G, et al. A prospective, randomized, multicenter food and drug administration investigation device exemption study of lumbar total disc replacement with the Charité artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes. Spine. 2005;30(14):1576–83. doi: 10.1097/01.brs.0000170561.25636.1c. [DOI] [PubMed] [Google Scholar]
- 3.McAfee PC, Cunningham BW, Hayes V, et al. Biomechanical analysis of rotational motions after disc arthroplasty: implications for patients with adult deformities. Spine (Phila Pa 1976) 2006;31(Suppl 19):S152–60. doi: 10.1097/01.brs.0000234782.89031.03. [DOI] [PubMed] [Google Scholar]
- 4.SariAli EH, Lemaire JP, Pascal-Mousselard H, Carrier H, Skalli W. In vivo study of the kinematics in axial rotation of the lumbar spine after total intervertebral disc replacement: long-term results: a 10–14 years follow up evaluation. Eur Spine J. 2006;15(10):1501–10. doi: 10.1007/s00586-005-0016-5. [DOI] [PubMed] [Google Scholar]
- 5.Tournier C, Aunoble S, Le Huec JC, Lemaire JP, Tropiano P, Lafage V, Skalli W. Total disc arthroplasty: consequences for sagittal balance and lumbar spine movement. Eur Spine J. 2007;16(3):411–21. doi: 10.1007/s00586-006-0208-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Guyer RD, Ohnmeiss DD. Intervertebral disc prostheses. Spine. 2003;28(15S):S15–S23. doi: 10.1097/01.BRS.0000076843.59883.E1. [DOI] [PubMed] [Google Scholar]
- 7.Galbusera F, Bellini CM, Zweig T, et al. Design concepts in lumbar total disc arthroplasty. Eur Spine J. 2008;17(12):1635–50. doi: 10.1007/s00586-008-0811-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Panjabi M, Oxland T, Yamamoto I, Crisco J. Mechanical behavior of the human lumbar and lumbosacral spine shown by three-dimensional load-displacement curves. J Bone Joint Surg. 1994;76-A:413–24. doi: 10.2106/00004623-199403000-00012. [DOI] [PubMed] [Google Scholar]
- 9.Frobin W, Brinckmann P, Biggemann M, et al. Precision measurement of disc height, vertebral height and sagittal plane displacement from lateral radiographic views of the lumbar spine. Clin Biomech. 1996;12(suppl 1):1–63. doi: 10.1016/s0268-0033(96)00067-8. [DOI] [PubMed] [Google Scholar]
- 10.Bonnet DG. Sample size requirements for estimating intraclass correlations with desired precision. Stat Med. 2002;21(9):1331–5. doi: 10.1002/sim.1108. [DOI] [PubMed] [Google Scholar]
- 11.Lim MR, Girardi FP, Zhang K, Huang RC, Peterson MG, Cammisa FP. Measurement of total disc replacement radiographic range of motion: a comparison of two techniques. J Spinal Disord Tech. 2005;18:252–6. [PubMed] [Google Scholar]
- 12.Johnson R, Axelsson P, Strömqvist B. Mobility provocation of lumbar fusion evaluated bys radiostereometric analysis. Acta Orthop Scand. 1996;67(Suppl):45–6. [Google Scholar]
- 13.Leivseth G, Brinckmann P, Frobin W, Johnson R, Strömqvist B. Assessment of sagittal plane segmental motion in lumbar spine: a comparison between distortion-compensated and stereophotogrammetric roentgen analysis. Spine (Phila Pa 1976) 1998;23(23):2648–55. doi: 10.1097/00007632-199812010-00021. [DOI] [PubMed] [Google Scholar]
- 14.Ordway NR, Fayyazi AH, Abjornson C, et al. Twelve-month follow-up of lumbar spine range of motion following intervertebral disc replacement using radiostereometric analysis. SAS Journal Winter. 2008;2:9–15. doi: 10.1016/SASJ-2007-0115-RR. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cakir B, Richter M, Puhl W, Schmidt R. Reliability of motion measurements after total disc replacement: the spike and the fin method. Eur Spine J. 2006;15(2):165–73. doi: 10.1007/s00586-005-0942-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Park CK, Ryu KS, Jee WH. Degenerative changes of discs and facet joints in lumbar total disc replacement using ProDisc II: minimum two-Year follow-up. Spine (Phila Pa 1976) 2008;33(16):1755–61. doi: 10.1097/BRS.0b013e31817b8fed. [DOI] [PubMed] [Google Scholar]
- 17.Moumene M, Geisler FH. Comparison of biomechanical function at ideal and varied surgical placement for two lumbar artificial disc implant designs: Mobile-core versus fixed-core. Spine (Phila Pa 1976) 2007;17:1840–51. doi: 10.1097/BRS.0b013e31811ec29c. [DOI] [PubMed] [Google Scholar]
- 18.Pearcy MJ, Tibrewal SB. Axial rotation and lateral bending in the normal lumbar spine measurement by three dimensional radiography. Spine. 1984;9(6):582–7. doi: 10.1097/00007632-198409000-00008. [DOI] [PubMed] [Google Scholar]
- 19.Lemaire JP, Carrier H, Sariali el-H, Skalli W, Lavaste F. Clinical and radiological outcomes with the Charité artificial disc: a 10-year minimum follow-up. J Spinal Disord Tech. 2005;18(4):353–9. doi: 10.1097/01.bsd.0000172361.07479.6b. [DOI] [PubMed] [Google Scholar]
- 20.Dvorák J, Vajda EG, Grob D, Panjabi MM. Normal motion of the lumbar spine as related to age and gender. Eur Spine J. 1995;4(1):18–23. doi: 10.1007/BF00298413. [DOI] [PubMed] [Google Scholar]