

Dear Editor,
A female, 27-year-old patient attended the health unit complaining of pain in her left upper limb for six months. The patient denied trauma or fever. Physical examination revealed increased limb volume, skin hardening, with no flogistic sign. Laboratory tests did not demonstrate any significant alteration.
Plain radiography of the affected limb and hip demonstrated alterations typical of melorheostosis, such as unilateral cortical hyperostosis along the bone axis resembling "melted candle wax" involving only one body segment (left hemibody) and extending from the humerus up to the hand bones (Figure 1). Similar alterations were also observed in the iliac bone at left (Figure 2)
Figure 1.

Radiographic images of left arm (A), forearm and hand (B) demonstrating cortical hyperostosis along the bone axis resembling “melted candle wax” (arrows).
Figure 2.
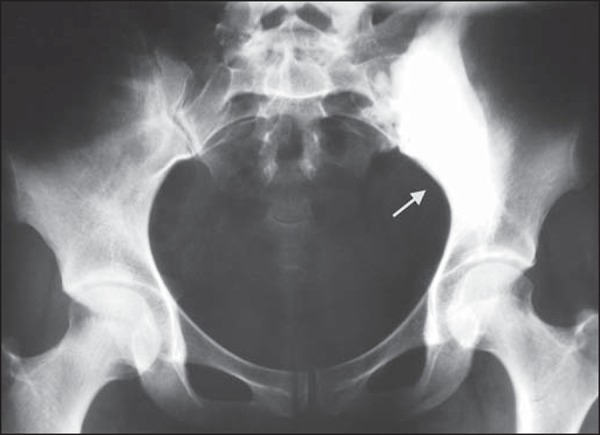
Radiographic image of hip shows iliac and sacrum hyperostosis (arrow), at left, with the same finding observed in the upper limb of the patient.
Melorheostosis is a rare sclerosing disease of unknown etiology characterized by involvement of, particularly, long bones and adjacent soft tissues. It has a peculiar radiological characteristic, i.e. cortical thickening resembling "melted candle wax"(1-3). Both female and male individuals are equally affected. The disease onset may occur at any age, but in 50% of cases it occurs before the age of 20(1).
Although it is a benign disease, it may bring clinically significant morbidity to patients. Initially it may be asymptomatic, but the association between bone sclerosis and tissue fibrosis leads to shortening of limbs, bone deformity and joints stiffness, gradually progressing to intense pain and functional incapacity of the affected limb.
Bone cortical thickening is the main pathological alteration, with both mature and immature components, thickened bone trabeculae and increased osteoblastic activity(1,2,4,5), that may extend to joints. It is common to observe involvement of adjacent soft tissues, with development of fibrotic, bone, cartilaginous and vascular tissues.
The disease distribution is peculiar and typically affects only one side of the body, and may be either mono- or polyostotic, in this latter presentation following sclerotomal distribution. Long bones of the lower limbs are most frequently affected(1-5). The disease rarely affects the spine, skull and the face. The diagnosis is essentially clinical and radiological. Laboratory tests results are usually normal and histological findings are nonspecific.
The classical radiological presentation is that of sclerosis in only one side of the cortical bone, with linear and segmental distribution, resembling melted candle wax dropping along the bone axis and projecting over the medullary space. Such an alteration may distally extend to finger bones.
Other observed presentations are similar to osteoma, striated osteopathy, osteopoikilosis, and myositis ossificans, with calcifications in adjacent soft tissues (1).
Computed tomography (CT) shows in more detail the sclerotic alterations as well as reduction of the medullary space. At magnetic resonance imaging (MRI) such alterations present with low signal intensity at T1- and T2-weighted sequences, a finding that is compatible with cortical bone. The involvement of soft tissues may also be observed, with variable calcification degrees at CT; and MRI shows images with heterogeneous signal intensities corresponding to mineralization, areas of fat and fibrovascular tissue(1,2).
Thus, melorheostosis is highlighted as a relevant differential diagnosis among bone diseases, particularly because of the characteristic radiographic findings of this disease.
REFERENCES
- 1.Suresh S, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. Clin Radiol. 2010;65:593–600. doi: 10.1016/j.crad.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 2.Nuño C, Heili S, Alonso J, et al. Melorreostosis: presentación de un caso y revisión de la literatura. Rev Esp Enferm Metab Oseas. 2001;10:50–55. [Google Scholar]
- 3.Salman Monte TC, Rotés Sala D, Blanch Rubió J, et al. Melorheostosis, a case report. Reumatol Clin. 2011;7:346–348. doi: 10.1016/j.reuma.2010.11.007. [DOI] [PubMed] [Google Scholar]
- 4.Mariaud-Schmidt RP, Bitar WE, Pérez-Lamero F, et al. Melorheostosis: unusual presentation in a girl. Clin Imaging. 2002;26:58–62. doi: 10.1016/s0899-7071(01)00351-5. [DOI] [PubMed] [Google Scholar]
- 5.Gagliardi GG, Mahan KT. Melorheostosis: a literature review and case report with surgical considerations. J Foot Ankle Surg. 2010;49:80–85. doi: 10.1053/j.jfas.2009.08.004. [DOI] [PubMed] [Google Scholar]