

Abstract
Background
Novel robots have recently been developed specifically for endonasal surgery. They can deliver several thin, tentacle-like surgical instruments through a single nostril. Among the many potential advantages of such a robotic system is the prospect of telesurgery over long distances.
Objective
To describe a phantom pituitary tumor removal done by a surgeon in Nashville, Tennessee, controlling a robot located approximately 800 km away in Chapel Hill, North Carolina. This is the first remote telesurgery experiment involving tentacle-like concentric tube manipulators.
Methods
A phantom pituitary tumor removal experiment was conducted twice – once locally and once remotely – using the robotic system. Robot commands and video were transmitted across the Internet. The latency of the system was evaluated quantitatively in both local and remote cases to determine the effect of the 800 km between the surgeon and robot.
Results
We measured a control and video latency of less than 100 ms in the remote case. Qualitatively, the surgeon was able to carry out the experiment easily, and observed no discernable difference between the remote and local cases.
Conclusion
Telesurgery over long distances is feasible with this robotic system. In the longer term, this may enable expert skull base surgeons to help many more patients by performing surgeries remotely over long distances.
Keywords: Reaction Time, Remote operations, Robotics, Skull base, Telerobotics
Introduction
The concept of remote telesurgery was a central motivation in the early development of surgical robots1. This led directly to the first commercial systems and to Operation Lindbergh in 20012, a celebrated milestone in robotic telesurgery, in which a surgeon in New York performed a robotic cholecystectomy on a patient in Strasbourg, France. Recent years have seen additional telesurgery demonstrations including a laparoscopic cholecystectomy on pigs between Korea and Japan3, a method for an atrial fibrillation ablation between Boston and Milan4, and even a demonstration using a robot on the ocean floor by a surgeon on land5, among others. However, endonasal surgery has not yet been demonstrated in a telesurgical setting because traditional surgical robots6 are not well suited to transnasal surgery due to large tool diameters and inability to coordinate the delivery of multiple tools through a nostril.
Lacking a suitable robot, prior studies on remote interaction in otolaryngology have focused on telementoring for pre-operative planning and consultation over the Internet7,8,9. Remote patient monitoring in otolaryngology8, and remote endoscope control in various surgical contexts10,11, have also been explored. Transmission of navigation information12 has also been accomplished over long distances, and images (both preoperative CT and intraoperative video), 3-D models, a surgical plan, and even digitized locations of standard surgical instruments were transmitted in real-time over the Internet during an endonasal procedure13. However, remote control of surgical instruments themselves has not yet been accomplished. Fortunately, recent breakthroughs in robotics, notably the invention of concentric tube robots (a review on this technology is available here14) have inspired the development of a purpose-built teleoperated system for endonasal skull base surgery15,16,17. Previously, the surgeon using these systems has always been located in the same room as the patient, not at a remote location. Thus, in this paper we use this system to explore for the first time the idea of remotely controlling surgical tools over long distances for endonasal skull base surgery, with tool motions and endoscopic video transmitted over the Internet.
The design of our endonasal robot has been previously described in the literature15,18,19. Briefly, it functions by delivering several concentric tube manipulators (see Figure 1) through a nostril. These manipulators are constructed using concentric, elastic tubes (made of Nitinol) that can be telescopically extended and axially rotated at their bases, in a manner conceptually similar to the guide wire of a catheter. Also like a guide wire, each tube is pre-curved, and hence the tubes elastically interact as they slide over one another. The net result is a device that can both elongate and bend, and mechanics-based models are used to describe the curve of the manipulator as a function of tube base axial angles and telescopic extension distances20. Surgical instruments such as endoscopic cameras, grippers, curettes, and suction and irrigation can be delivered to the surgical site at the tips of these manipulators (see Figure 2). We note that further hardware development will be needed before this system is ready for in vivo human use: we envision the system eventually having modular instrument attachments similar to the Intuitive Surgical da Vinci system, so that instruments can be exchanged during surgery (see15,18 for further discussion of the current prototype and the long-term vision for the robot hardware). Fortunately, since similar motors and components will be used in an eventual clinical system, we need not wait until the hardware is human-ready before we do many technical tests with the system. These include exploring the ability of surgeons to use it to resect tumors, as well as the potential for remote teleoperation. Indeed, we have already completed preliminary experiments with this prototype in which experienced surgeons used it to remove anthropomorphic phantom pituitary tumors16,21. Our goal in this paper is to explore the feasibility of telesurgery with this prototype by performing a similar experiment with surgeon commands transmitted over the Internet to a remote location.
Figure 1.

An active cannula gripper together with a DaVinci gripper.
Figure 2.

Setup trial of transnasal skull base surgery robot system in a human cadaver head and the endoscopic view of the pituitary gland.
Methods
Our experiment was conducted as illustrated in Figure 3, and the goal of this experiment is to examine whether distance and Internet transmission of surgeon’s commands would significantly affect the surgeon’s ability to resect pituitary tumors using the robot. The surgeon manipulated a master interface (Phantom Omni, Sensable, Inc.) to control the concentric tube manipulators under endoscopic visualization. The surgeon’s motions were mapped to robot motions using a standard resolved rates algorithm15. The robot was placed locally (i.e. in the same room as the surgeon) in one trial and remotely (approximately 800 km away) in the other using the same type of connection (1 GB/s) and the same framework described by Haoran et al.22 (the connection between the two universities was 10 GB/s, but the bottleneck is the 1 GB/s connection from each laboratory to the Internet backbone of the university). Thus, the only difference between the two cases is the presence of the Internet connection in the remote experiment, which introduces some latency. In each case, a phantom tumor was placed in the sella of an artificial skull according to procedures developed previously for local experiments of the same type15,16,17,23,24. During the remote experiment, the surgeon was located at Vanderbilt University (Nashville, Tennessee, USA) and the robot was located at the University of North Carolina at Chapel Hill (Chapel Hill, North Carolina, USA). We used a computer to capture the endoscope video and send this video to the surgeon using the free, publicly available Skype software which is designed for low latency videoconferencing25.
Figure 3.
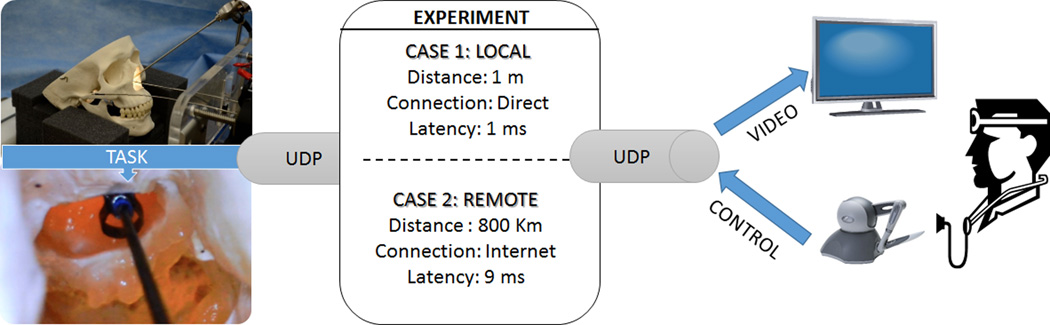
The left two images show the endoscope view of the curette in the sella and the setup of the robot with the skull. The two experimental conditions (local and remote) are illustrated in the central square, with the surgeon interface indicated on the rightmost image.
To explore the quality of the connection quantitatively, we used two well-established metrics: Latency26,27 and Inter-Arrival Time (IAT)28. Latency is the time that one control packet takes to travel from where it originates to its destination and its value directly depends of factors such as network congestion and the specifics of operating systems and routers that handle the packets during their transit. If latency becomes large, the robot will move sluggishly, and excessive latency will affect surgical performance29; IAT is defined as the time between the receipt of two consecutive packets at the surgeon-side computer, which can also vary due to network congestion. Large variations in IAT will reduce the smoothness of robot’s response to the surgeon’s commanded motions.
Results
The surgeon carried out each phantom tumor resection experiment in 20 minutes, in both the local case (where the robot was in the same room as the surgeon) and the remote case (where the robot was located 800km distant). See Figure 4 and Figure 5 for an illustration of the experimental setup. During this 20-minute period, approximately 120,000 packets were transferred and analyzed to determine latency and IAT (see Table 1). In Figure 6, a random sample of 500 packets of raw latency data is shown for both cases. Five minutes was selected simply because it is convenient visualization of differences between local and remote experiment, and the data was sufficiently consistent that one five minute window looked visually much like any other. Table 1 summarizes all packets collected during the 20-minute experiment. Figure 7 shows a sample of the IAT data for the same time period illustrated in Figure 6. Note that the IAT is nominally 10 ms in both cases, since packets are transmitted at 10 ms intervals. As one would expect, the average IAT in both experiments was close to 10 ms, with larger maximum and minimum values in the remote experiment due to Internet congestion.
Figure 4.


(A) Surgeon in Nashville using a robot located in North Carolina to remove phantom pituitary tissue. (B) Experimental setup of the local experiment with both the robot and surgeon at Vanderbilt.
Figure 5.

Setup trial of transnasal skull base surgery robot system with the endoscopic view of the phantom tumor and the Sella.
Table 1.
Data for both the local and remote experiments. (StDev= Standard Deviation)
| Case 1: Local | Case 2: Remote | |||||||
|---|---|---|---|---|---|---|---|---|
| Average | Max | Min | StDev | Average | Max | Min | StDev | |
| Latency | 1.1 ms | 4 ms | 1 ms | 0.66 ms | 10.37 ms | 22 ms | 9 ms | 2.77 ms |
| IAT | 10 ms | 18 ms | 1 ms | 2.51 ms | 10.17 ms | 50 ms | > 0 ms | 4.83 ms |
Figure 6.

The Latency in the surgeon’s control commands for both experiments
Figure 7.

Sample of IAT for the same time period shown in Figure 6. The moving average over 5 packets is shown.
Finally, the surgeon was asked to describe his perception of operating the remote system in comparison to operating the same system locally. He noted that he observed no discernable difference in system performance, and had to keep reminding himself that the robot was hundreds of miles away from him, because the experience for him was the same locally or remotely. He noted that he did not experience any difficulty with control smoothness or hand-eye coordination in either case.
Discussion
When considering latency in surgery, the most important issue is whether the surgeon perceives the robot as lagging behind his or her hand motions during use. It is well established in the engineering literature that this dissociation between input and output motions starts at about 100ms29,30, and can become problematic at latencies greater than 300 ms31, at which point a latency control/manager32 must generally be introduced to assist the user. Operation Lindbergh2 reported a control latency of approximately 40 ms and found that this latency did not affect surgeon’s perception of the safety of the operation, since all surgeons gave the system a perfect subjective score in “perception of the safety of the operation”33.
We note that Operation Lindbergh used a dedicated telecommunications connection, which is useful for ensuring quality of service, but is challenging to set up and costly. Thus, it is desirable to use an Internet-based approach, though future hurdles do exist in terms of ensuring quality of service over the Internet. Still, we believe that since Internet networking protocols are improving all the time, it is reasonable to foresee a time in the not too distant future when Internet protocols are sufficiently reliable to enable Internet-based telesurgery. Indeed, by 2006 networking technology improvements enabled 6.5 ms of control latency in a laparoscopic cholecystectomy between Korea and Japan3. In our experiment, even in the presence of standard Internet traffic, the surgeon’s control signal had an average latency of 10.37 ms, which is lower than the latency of Operation Lindbergh, which was sufficient for laparoscopic cholecystectomy. In our experiments, standard deviations (Table 1) illustrate that as one would expect, there is more variation in control signal latency and IAT in the remote case than the local case (see also Figures 6 and 7 for illustration). However, as mentioned previously, these variations were sufficiently low that they did not affect surgeon perception of teleoperation.
With regard to the video transmission, Skype delivered a video latency with an average of 20 ms, which represents better performance than both Operation Lindbergh and the Korea-Japan experiment3 mentioned previously, which reported latencies of 155 ms and 435.5 ms, respectively. We note that in the future, before our system can be used with human subjects, it will require video transmission software that has been designed for remote surgery and rigorously tested. Our results indicate that a Skype-like program could achieve this goal, but we note that other video transmission architectures designed specifically for surgery, such as the system by Klapan et al13, would be applicable to our system if needed.
In summary, our results indicate that extremely low latencies are possible over standard Internet connections using off-the-shelf software. However, a dedicated connection would be recommended to control the delay. There are many next steps with our robotic system. First, we are currently designing modular tool interfaces similar to the da Vinci robot so that tools can be easily changed during surgery. We are also simultaneously addressing sterilizability concerns. The next step will be experiments to validate the system when interacting with perfused tissues, possibly in an animal model, and additional cadaver testing. It will take a few years to complete these tests, but once they are accomplished and we are able to perform our first live human case, it is useful to know that long-distance teleoperation will be straightforwardly feasible, as we have shown in this paper.
Conclusion
In this paper we have described an initial feasibility study on telesurgery for endonasal skull base surgery. This was enabled by the recent development of the first robot specifically designed for endonasal surgery. Such a telesurgery system complements prior results in telementoring by providing a way for the remote surgeon to actively participate in the surgery for educational purposes or to bring the advantages of endonasal surgery to a wider range of patients. Our feasibility study showed that it is possible to achieve low latency and low inter-arrival time with this surgical robot, indicating that it is likely to be possible to achieve telesurgery using it. This agreed with the qualitative feel of the surgeons who used the system, who noted that the remote experiment did not feel significantly different to them than the local experiment, and that they were very confident that they could use such a robot to perform a real surgery. Thus, in summary, we demonstrated that critical components required for a telesurgery system for endonasal skull base surgery were effective, and we look forward to a future in which concentric tube robots are widely deployed in hospitals and used in endonasal skull base procedures in both a local and remote context.
Acknowledgments
This work was funded in part by award number IIS-1054331 from the National Science Foundation, and in part award numbers R01 EB017467 and R21 EB017952 from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Science Foundation or the National Institutes of Health.
Footnotes
Disclosure: The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
References
- 1.Madhani AJ, Niemeyer G, Salisbury JK. Proceedings. 1998 IEEE/RSJ International Conference on Intelligent Robots and Systems. Innovations in Theory, Practice and Applications (Cat. No.98CH36190) Vol. 2. IEEE; 1998. The Black Falcon: a teleoperated surgical instrument for minimally invasive surgery; pp. 936–944. [Google Scholar]
- 2.Marescaux J, Leroy J, Gagner M, et al. Transatlantic robot-assisted telesurgery. Nature. 2001;413(6854):379–380. doi: 10.1038/35096636. [DOI] [PubMed] [Google Scholar]
- 3.Arata J, Takahashi H, Pitakwatchara P, et al. Proceedings 2006 IEEE International Conference on Robotics and Automation, 2006. ICRA 2006. IEEE; 2006. A remote surgery experiment between Japan-Korea using the minimally invasive surgical system; pp. 257–262. [Google Scholar]
- 4.Pappone C, Vicedomini G, Manguso F, et al. Robotic magnetic navigation for atrial fibrillation ablation. J Am Coll Cardiol. 2006;47(7):1390–1400. doi: 10.1016/j.jacc.2005.11.058. [DOI] [PubMed] [Google Scholar]
- 5.Malik T. Deep Diving Team to Test Robotic Surgeons on Sea Floor. [Accessed December 6, 2014];2007 Available at: http://www.space.com/3771-deep-diving-team-test-robotic-surgeons-sea-floor.html. [Google Scholar]
- 6.Sekhar LN, Tariq F, Kim LJ, Pridgeon J, Hannaford B. Commentary: Virtual reality and robotics in neurosurgery. Neurosurgery. 2013;72(Suppl 1):1–6. doi: 10.1227/NEU.0b013e31827db647. [DOI] [PubMed] [Google Scholar]
- 7.Freysinger W, Gunkel AR, Thumfart WF, Truppe MJ. Teleprescence in ear, nose, and throat surgery. In: Beretta GB, Schettini R, editors. Photonics West 2001 - Electronic Imaging. International Society for Optics and Photonics; 2000. pp. 316–324. [Google Scholar]
- 8.Klapan I, Vranjes Z, Risavi R, Simicić L, Prgomet D, Glusac B. Computer-assisted surgery and computer-assisted telesurgery in otorhinolaryngology. [Accessed March 27, 2014];Ear Nose Throat J. 2006 85(5):318–321. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16771024. [PubMed] [Google Scholar]
- 9.Shenai MB, Dillavou M, Shum C, et al. Virtual interactive presence and augmented reality (VIPAR) for remote surgical assistance. Neurosurgery. 2011;68:200–207. doi: 10.1227/NEU.0b013e3182077efd. (1 Suppl Operative) discussion 207. [DOI] [PubMed] [Google Scholar]
- 10.Suzuki N, Hattori A, Ieiri S, et al. Tele-control of an endoscopic surgical robot system between Japan and Thailand for tele-NOTES. [Accessed April 8, 2014];Stud Health Technol Inform. 2009 142:374–379. Available at: http://www.ncbi.nlm.nih.gov/pubmed/19377187. [PubMed] [Google Scholar]
- 11.Hopf NJ, Kurucz P, Reisch R. Three-dimensional HD endoscopy – first experiences with the Einstein Vision system in neurosurgery. [Accessed May 15, 2014];Innov Neurosurg. 2013 1(2):125–131. Available at: http://www.degruyter.com/view/j/ins.2013.1.issue-2/ins-2013-0009/ins-2013-0009.xml. [Google Scholar]
- 12.Kawamata T, Iseki H, Shibasaki T, Hori T. Endoscopic augmented reality navigation system for endonasal transsphenoidal surgery to treat pituitary tumors: technical note. Neurosurgery. 2002;50(6):1393–1397. doi: 10.1097/00006123-200206000-00038. [DOI] [PubMed] [Google Scholar]
- 13.Klapan I, Risavi R, Simicic L, Simovic S. Tele-3D-C-FESS approach with high-quality video transmission. Otolaryngol - Head Neck Surg. 1999;121(2):P187–P188. [Google Scholar]
- 14.Gilbert HB, Rucker DC, Webster RJ. Concentric Tube Robots: The State of the Art and Future Directions. To appear in Springer Tracts in Advanced Robotics [Google Scholar]
- 15.Burgner J, Rucker DC, Gilbert HB, et al. A Telerobotic System for Transnasal Surgery. IEEE/ASME Trans Mechatronics. 2014;19(3):996–1006. doi: 10.1109/TMECH.2013.2265804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gilbert HB, Swaney PJ, Burgner J, Weaver KD, Russell PT, Webster RJ. A Feasibility Study on the use of Concentric Tube Continuum Robots for Endonasal Skull Base Tumor Removaltle; Hamlyn Symposium on Medical Robotics; 2012. Available at: http://research.vuse.vanderbilt.edu/MEDLab/pub_files/GilbertFeasibilityHamlyn12.pdf. [Google Scholar]
- 17.Schneider JS, Burgner J, Webster RJ, Russell PT. Robotic surgery for the sinuses and skull base: what are the possibilities and what are the obstacles? Curr Opin Otolaryngol Head Neck Surg. 2013;21(1):11–16. doi: 10.1097/MOO.0b013e32835bc650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Swaney PJ, Croom JM, Burgner J, et al. Design of a Quadramanual Robot For Single-Nostril Skull Base Surgery. [Accessed June 11, 2014];Proc 2012 Dyn Syst Control Conf. 2012 3:387–393. Available at: http://proceedings.asmedigitalcollection.asme.org/proceeding.aspx?articleid=1739352. [Google Scholar]
- 19.Burgner J, Gilbert HB, Webster RJ. 2013 IEEE International Conference on Robotics and Automation. IEEE; 2013. On the computational design of concentric tube robots: Incorporating volume-based objectives; pp. 1193–1198. [Google Scholar]
- 20.Rucker DC, Jones BA, Webster RJ. A Geometrically Exact Model for Externally Loaded Concentric-Tube Continuum Robots. IEEE Trans Robot. 2010;26(5):769–780. doi: 10.1109/TRO.2010.2062570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Swaney PJ, Gilbert HB, Webster RJ, III, Russell PT, III, Weaver KD. Endonasal Skull Base Tumor Removal Using Concentric Tube Continuum Robots: A Phantom Study. J Neurol Surg Part B Skull Base. doi: 10.1055/s-0034-1390401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yu H, Shen J-H, Joos KM, Simaan N. 2013 IEEE International Conference on Robotics and Automation. IEEE; 2013. Design, calibration and preliminary testing of a robotic telemanipulator for OCT guided retinal surgery; pp. 225–231. [Google Scholar]
- 23.Bekeny JR, Swaney PJ, Webster RJ, Russell PT, Weaver KD. Forces Applied at the Skull Base during Transnasal Endoscopic Transsphenoidal Pituitary Tumor Excision. J Neurol Surg B Skull Base. 2013;74(6):337–341. doi: 10.1055/s-0033-1345108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gilbert HB, Hendrick R, Remirez A, Webster R. A robot for transnasal surgery featuring needle-sized tentacle-like arms. Expert Rev Med Devices. 2014;11(1):5–7. doi: 10.1586/17434440.2013.854702. [DOI] [PubMed] [Google Scholar]
- 25.Kryczka A, Arefin A, Nahrstedt K. 2013 IEEE International Symposium on Multimedia. IEEE; 2013. AvCloak: A Tool for Black Box Latency Measurements in Video Conferencing Applications; pp. 271–278. [Google Scholar]
- 26.Rayman R, Primak S, Patel R, et al. Effects of latency on telesurgery: an experimental study. [Accessed June 11, 2014];Med Image Comput Comput Assist Interv. 2005 8(Pt 2):57–64. doi: 10.1007/11566489_8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16685943. [DOI] [PubMed] [Google Scholar]
- 27.Rayman R, Croome K, Galbraith N, et al. Long-distance robotic telesurgery: a feasibility study for care in remote environments. Int J Med Robot. 2006;2(3):216–224. doi: 10.1002/rcs.99. [DOI] [PubMed] [Google Scholar]
- 28.Wirz R, Marin R, Ferre M, Barrio J, Claver JM, Ortego J. Bidirectional Transport Protocol for Teleoperated Robots. IEEE Trans Ind Electron. 2009;56(9):3772–3781. [Google Scholar]
- 29.Tatematsu A, Ishibashi Y, Fukushima N, Sugawara S. 2010 IEEE International Workshop Technical Committee on Communications Quality and Reliability (CQR 2010) IEEE; 2010. QoE assessment in haptic media, sound and video transmission: Influences of network latency; pp. 1–6. [Google Scholar]
- 30.Jeffay K, Hudson T, Parris M. Proceedings 27th EUROMICRO Conference. 2001: A Net Odyssey. IEEE Comput. Soc; 2001. Beyond audio and video: multimedia networking support for distributed, immersive virtual environments; pp. 300–307. [Google Scholar]
- 31.Richard Held, Aglaia Efstathiou MG. Adaptation to displaced and delayed visual feedback from the hand. [Accessed May 21, 2014];J Exp Prychol. 1966 :887–891. Available at: http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.211.4439. [Google Scholar]
- 32.Anderson RJ, Spong MW. Bilateral control of teleoperators with time delay. IEEE Trans Automat Contr. 1989;34(5):494–501. [Google Scholar]
- 33.Marescaux J, Leroy J, Rubino F, et al. Transcontinental robot-assisted remote telesurgery: feasibility and potential applications. [Accessed September 8, 2014];Ann Surg. 2002 235(4):487–492. doi: 10.1097/00000658-200204000-00005. Available at: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1422462&tool=pmcentrez&rendertype=abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]