

Abstract
Background and Aim:
Advances in biomedical technology have made medical treatment to be continued beyond a point, at which it does not confer an advantage but may increase the suffering of patients. In such cases, continuation of care may not always be useful, and this has given rise to the concept of limitation of life-sustaining treatment. Our aim was to study mortality patterns over a 6-year period in a Pediatric Intensive Care Unit (PICU) in a developing country and to compare the results with published data from other countries.
Materials and Methods:
Retrospective cohort study was conducted in a PICU of a tertiary care hospital in Pakistan. Data were drawn from the medical records of children aged 1-month – 16 years of age who died in PICU, from January 2007 to December 2012.
Results:
A total of 248 (from an admitted number of 1919) patients died over a period of 6 years with a mortality rate 12.9%. The median age of children who died was 2.8 years, of which 60.5% (n = 150) were males. The most common source of admission was from the emergency room (57.5%, n = 143). The most common cause of death was limitation of life-sustaining treatment (63.7%, n = 158) followed by failed cardiopulmonary resuscitation (28.2%, n = 70) and brain death (8.1%, n = 20). We also found an increasing trend of limitation of life-sustaining treatment do-not-resuscitate (DNR) over the 6-year reporting period.
Conclusion:
We found limitation of life support treatment (DNR + Withdrawal of Life support Treatment) to be the most common cause of death, and parents were always involved in the end-of-life care decision-making.
Keywords: Brain death, death, do-not-resuscitate, end-of-life care, failed cardiopulmonary resuscitation, Pediatric Intensive Care Unit, withdrawal of care
Introduction
Severity of disease of hospitalized patients has increased over the past decade, and advanced techniques have allowed such patients to stay alive.[1] It is well-known that advances in medicine and biomedical technology have created the likelihood for medical treatment to be continued beyond a point, of which it offers no advantage to the patient and may lengthen suffering.[2,3] It is widely recognized that continued care may not always be advantageous, and this concept has given rise to frequent limitation of life support treatment (LST).[1] The concept of limitation of LST which includes do-not-resuscitate (DNR) and Withdrawal of LST (WLST) has examined medical practices to avoid use of treatment which lengthen the patient's life and does not improve the patient's outcomes.[4,5] In North America and Europe, 28–65% of all Pediatric Intensive Care Unit (PICU) deaths follow restriction of LST.[5,6,7,8,9] In contrast to the west, where limitation proceeds up to 90% of deaths; the rate in India is 22–50%,[10,11,12] in Iran 6.7%,[13] and in Saudi Arabia[14] 34%. Different cultures, religions, philosophic, legal, and professional attitudes may in part explain these differences.[1,15,16,17,18,19]
In the context of Pakistan, the availability of PICU is largely limited to major cities in the country.[20] The cost of intensive care is high and affordable only by middle-high income groups.[10,20] Prolonged PICU stay often drains the financial resources of financially well-off families.[10,20] We could not find any published reports from Pakistan on patterns of mortality among critically ill children in PICU. Therefore, our aim was to conduct a retrospective review on mortality patterns over a 6-year period in a PICU and to compare the results with published data from other countries.
Materials and Methods
We retrospectively reviewed the medical records for all children aged 1-month to 16 years old admitted in the PICU from January 2007 to December 2012. The PICU is a tertiary care private-sector teaching hospital in Karachi, the most populous city of Pakistan. It is a 4- bedded closed, multidisciplinary, medical-surgical unit with about 350 admissions per year.
Trends of mortality were categorized into 4 groups: (1) Failed cardiopulmonary resuscitation (CPR), (2) DNR, (3) Brain Death, and (4) WLST. The decision of DNR was made by the attending physician after detail discussion and informed consent from parents/guardians. The WLST was done with the involvement of a hospital ethical committee and the attending consultant after obtaining informed consent from parents/guardians. We have Hospital Ethical Committee, having members, who are trained with Accredited Ethical Fellowship program. Ethical committee was involved in each case of WLST and most cases of DNR. Other data collected from the medial records included patient demographics (i.e. age, sex, admission source such as the emergency room [ER] or operating theatre,) along with the admitting diagnosis. Statistical analysis was conducted using SPSS, version 19 (IBM SPSS statistics). Descriptive data were reported as means, medians and percentages. The study was approved by the Ethical Review Committee of the University.
Results
A total of 1919 children were admitted to the PICU over the 6 years period, of which 248 children died with mortality rate of 12.9%. Most of the children who died were male 60.5% (n = 150) with a median age of 2.8 years (interquartile range 0.4–8 years), and 65% of children who died were under 5 years old. All the children had initially aggressive supportive care including mechanical ventilation. Overall, the incidence of admission was highest from the ER (57.7%, n = 143) [Table 1].
Table 1.
Characteristics of children who died in Pediatric ICU
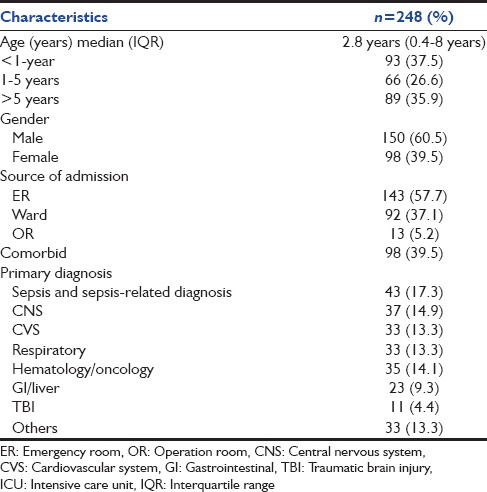
Most of the children died with a sepsis or sepsis-related diagnosis (17.3%, n = 43) followed by central nervous system (CNS) involvement. In 63.7% (n = 158) children, death was followed by some kind of limitation of LST, which involved DNR and WLST with DNR being more prevalent while in 28.2% of children (n = 70) full resuscitative procedures were carried out. Brain death occurred in 8.1% of children (n = 20) [Figure 1]. We also found an increasing trend of limitation of LST (DNR) over the period of 6 years [Figure 2].
Figure 1.
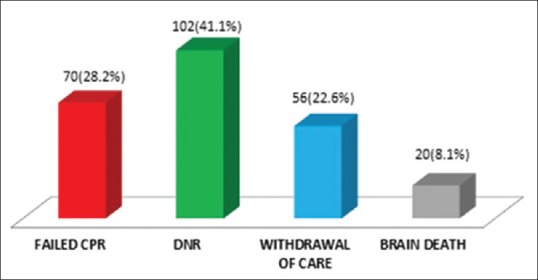
Modes of death among critically ill pediatric patients in pediatric intensive care unit
Figure 2.
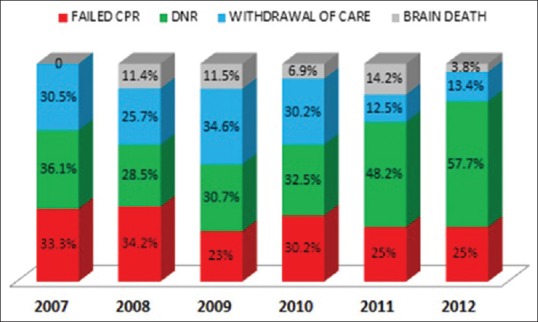
Pattern of modes of death over 6 years study period among critically ill pediatric population in pediatric intensive care unit
Discussion
We report the pattern of mortality among critically ill children admitted to the PICU over a period of 6 years. The mortality rate in our cohort was higher to those reported in US (4–6.2%),[5,21,22] Canada (7.3%),[23] UK (5.1%),[24] and Europe (5.8%).[8] However, one study reported a mortality rate of 13.7%, which was similar to the present findings.[25]
The median age of child mortality in the PICU in our report was 2.8 years which is similar to other studies ranging from 0.8 to 3.1 years,[8,23,24,25] with mostly children under 1-year of age (27.9%)[24,26] as in our cohort 37.5%. Most of these critically ill children were admitted through the ER (57.7%) which is similar to other study.[13]
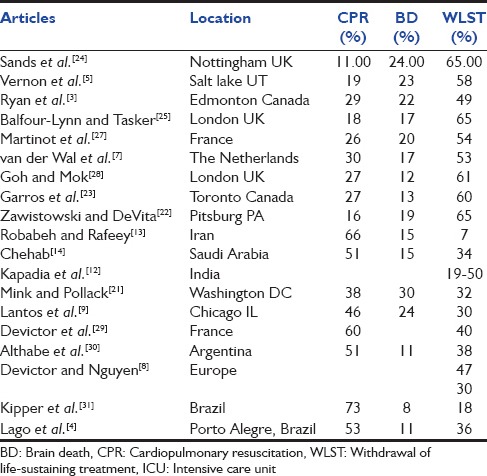
The most common primary admitting diagnosis was sepsis followed by CNS in our cohort whereas Acute Respiratory Failure and CNS were being the most common primary diagnosis in other studies.[2,13] There is a wide variation in the patterns of mortality among critically ill pediatric population in PICUs worldwide as shown in Table 2. We identified limitation of LST 63.5% (DNR and WLST) as the most frequent cause of mortality which is consistent with the majority of data from international studies followed by the failed CPR.[2,3,5,7,22,23,24,25,27]
Table 2.
Published articles on mode of deaths in pediatric ICU
Do-not-resuscitate is considered by most authors as an intermediate option between full support of patient and WLST.[4] DNR was the most frequently used form of limitation of LST in our cohort. However, failed CPR was reported as most common mode of death in other parts of the world.[4,8,9,13,14,21,30,31] The variation in the rate of active decision making at end-of-life (EOL) care may reflect either differences in attitudes and clinical behavior with respect to the active management of dying or may be due to variation in cultures or resources based on the PICU admission criteria whereby children with poor prognosis are not admitted in ICUs.[1,2,15,16,17,18,19] We found considerable parental involvement in the decision-making procedure. Our results echoed those from Canada,[3,23] USA,[5,9,21] and the UK[25,28] where parental involvement and consultation in decision-making regarding limitation of LST is common, and where parental sovereignty and informed consent are highlighted.[2] However, current practices in France[27,29] and South America[4,30,31] appear to be different. Their doctors take up a more authoritarian role in the decision-making process with little or no family consultation.
Studies have shown that children who die after limitation of LST are more likely to have chronic diseases as in our cohort where 72.5% of patients with chronic diseases had limitation of LST,[2,4,23] probably because these children have sufficiently recognized disease, with poor prognosis, and lengthening their lives would sometimes result in unnecessary treatment and needless suffering. One study showed that parents of children who had chronic disease were more likely to be satisfied with EOL care compared with parents whose children had undergone sudden or acute insults.[2,29] The families of children with chronic conditions may have more time to respond and accept an outcome of death.[2]
Advances in biology, science, and medical technology have intensely altered the medical landscape and our place in it.[13] The capacity to extend life beyond the point of which it may appear to have little or no benefit has forced us to scrutinize difficult questions regarding human identity, personhood, rights, and responsibilities with regard to access to medical care, the goals of health care, and the way managing dying patients.[13] More commonly, patients die not only as a result of the natural course of the disease but because of an active decision to limit the LST.[13] However, such decisions are always challenging. They are mostly complex, both clinically and morally, in relation to the care of neonates and children for the reason that there is often substantial diagnostic and prognostic ambiguity in these patients, and it may be challenging to assess accurately and predict the quality-of-life and functional capacity.[13]
There were several limitations in this study. First, it is a retrospective study which may have some recall and interpretation bias that could lead to incomplete data. Second, we did not examine the discussion between physician and families about EOL care. Qualitative evaluation may further elucidate the discussions between physicians and families. Third, the number of children died in the ward or at home after discharge with a terminal disease, and the patients who stayed alive in spite of limitation of LST (DNR order or WLST) are unknown. Fourth, this study might represent the reality in just one tertiary care center and, therefore, other studies are necessary to assess EOL circumstances in the PICUs all over the country.
Conclusion
We found limitation of LST (DNR + WLST) as the most common cause of death in our PICU. Parents were always involved in the EOL care decision-making. We also found an increasing trend of limitation of LST (DNR) over the 6-year period of the study.
Acknowledgment
We express our warm thanks to Dr. Aisha Yousufzai for her support and guidance in extensive grammar and language editing.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Devictor D, Latour JM, Tissières P. Forgoing life-sustaining or death-prolonging therapy in the pediatric ICU. Pediatr Clin North Am. 2008;55:791–804. doi: 10.1016/j.pcl.2008.02.008. xiii. [DOI] [PubMed] [Google Scholar]
- 2.Moore P, Kerridge I, Gillis J, Jacobe S, Isaacs D. Withdrawal and limitation of life-sustaining treatments in a paediatric intensive care unit and review of the literature. J Paediatr Child Health. 2008;44:404–8. doi: 10.1111/j.1440-1754.2008.01353.x. [DOI] [PubMed] [Google Scholar]
- 3.Ryan CA, Byrne P, Kuhn S, Tyebkhan J. No resuscitation and withdrawal of therapy in a neonatal and a pediatric intensive care unit in Canada. J Pediatr. 1993;123:534–8. doi: 10.1016/s0022-3476(05)80946-1. [DOI] [PubMed] [Google Scholar]
- 4.Lago PM, Piva J, Kipper D, Garcia PC, Pretto C, Giongo M, et al. Life support limitation at three pediatric intensive care units in southern Brazil. J Pediatr (Rio J) 2005;81:111–7. [PubMed] [Google Scholar]
- 5.Vernon DD, Dean JM, Timmons OD, Banner W, Jr, Allen-Webb EM. Modes of death in the pediatric intensive care unit: Withdrawal and limitation of supportive care. Crit Care Med. 1993;21:1798–802. doi: 10.1097/00003246-199311000-00035. [DOI] [PubMed] [Google Scholar]
- 6.ten Berge J, de Gast-Bakker DA, Plötz FB. Circumstances surrounding dying in the paediatric intensive care unit. BMC Pediatr. 2006;6:22. doi: 10.1186/1471-2431-6-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van der Wal ME, Renfurm LN, van Vught AJ, Gemke RJ. Circumstances of dying in hospitalized children. Eur J Pediatr. 1999;158:560–5. doi: 10.1007/s004310051147. [DOI] [PubMed] [Google Scholar]
- 8.Devictor DJ, Nguyen DT. Forgoing life-sustaining treatments in children: A comparison between Northern and Southern European pediatric intensive care units. Pediatr Crit Care Med. 2004;5:211–5. doi: 10.1097/01.PCC.0000123553.22405.E3. [DOI] [PubMed] [Google Scholar]
- 9.Lantos JD, Berger AC, Zucker AR. Do-not-resuscitate orders in a children's hospital. Crit Care Med. 1993;21:52–5. doi: 10.1097/00003246-199301000-00012. [DOI] [PubMed] [Google Scholar]
- 10.Mani RK. End-of-life care in India. Intensive Care Med. 2006;32:1066–8. doi: 10.1007/s00134-006-0185-7. [DOI] [PubMed] [Google Scholar]
- 11.Mani RK. Limitation of life support in the ICU. Ethical issues relating to end of life care. Indian J Crit Care Med. 2003;7:112–7. [Google Scholar]
- 12.Kapadia F, Singh M, Divatia J, Vaidyanathan P, Udwadia FE, Raisinghaney SJ, et al. Limitation and withdrawal of intensive therapy at the end of life: Practices in intensive care units in Mumbai, India. Crit Care Med. 2005;33:1272–5. doi: 10.1097/01.ccm.0000165557.02879.29. [DOI] [PubMed] [Google Scholar]
- 13.Robabeh G, Rafeey M. Prediction of mortality circumstances in the pediatric intensive care unit. Res J Biol Sci. 2008;3:1034–6. [Google Scholar]
- 14.Chehab M. Modes of death in a pediatric intensive care unit in the Muslim community of Saudi Arabia. Clin Intensive Care. 2003;14:135–9. [Google Scholar]
- 15.Yaguchi A, Truog RD, Curtis JR, Luce JM, Levy MM, Mélot C, et al. International differences in end-of-life attitudes in the intensive care unit: Results of a survey. Arch Intern Med. 2005;165:1970–5. doi: 10.1001/archinte.165.17.1970. [DOI] [PubMed] [Google Scholar]
- 16.Miccinesi G, Fischer S, Paci E, Onwuteaka-Philipsen BD, Cartwright C, van der Heide A, et al. Physicians’ attitudes towards end-of-life decisions: A comparison between seven countries. Soc Sci Med. 2005;60:1961–74. doi: 10.1016/j.socscimed.2004.08.061. [DOI] [PubMed] [Google Scholar]
- 17.Vincent JL. Forgoing life support in western European intensive care units: The results of an ethical questionnaire. Crit Care Med. 1999;27:1626–33. doi: 10.1097/00003246-199908000-00042. [DOI] [PubMed] [Google Scholar]
- 18.Sprung CL, Cohen SL, Sjokvist P, Baras M, Bulow HH, Hovilehto S, et al. End-of-life practices in European intensive care units: The Ethicus Study. JAMA. 2003;290:790–7. doi: 10.1001/jama.290.6.790. [DOI] [PubMed] [Google Scholar]
- 19.Young RJ, King A. Legal aspects of withdrawal of therapy. Anaesth Intensive Care. 2003;31:501–8. doi: 10.1177/0310057X0303100502. [DOI] [PubMed] [Google Scholar]
- 20.Haque A, Ladak LA, Hamid MH, Mirza S, Siddiqui NR, Bhutta ZA. A national survey of pediatric intensive care units in Pakistan. J Crit Care Med 2014. 2014:1–4. [Google Scholar]
- 21.Mink RB, Pollack MM. Resuscitation and withdrawal of therapy in pediatric intensive care. Pediatrics. 1992;89:961–3. [PubMed] [Google Scholar]
- 22.Zawistowski CA, DeVita MA. A descriptive study of children dying in the pediatric intensive care unit after withdrawal of life-sustaining treatment. Pediatr Crit Care Med. 2004;5:216–23. doi: 10.1097/01.pcc.0000123547.28099.44. [DOI] [PubMed] [Google Scholar]
- 23.Garros D, Rosychuk RJ, Cox PN. Circumstances surrounding end of life in a pediatric intensive care unit. Pediatrics. 2003;112:e371. doi: 10.1542/peds.112.5.e371. [DOI] [PubMed] [Google Scholar]
- 24.Sands R, Manning JC, Vyas H, Rashid A. Characteristics of deaths in paediatric intensive care: A 10-year study. Nurs Crit Care. 2009;14:235–40. doi: 10.1111/j.1478-5153.2009.00348.x. [DOI] [PubMed] [Google Scholar]
- 25.Balfour-Lynn IM, Tasker RC. At the coalface – Medical ethics in practice. Futility and death in paediatric medical intensive care. J Med Ethics. 1996;22:279–81. doi: 10.1136/jme.22.5.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ramnarayan P, Craig F, Petros A, Pierce C. Characteristics of deaths occurring in hospitalised children: Changing trends. J Med Ethics. 2007;33:255–60. doi: 10.1136/jme.2005.015768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Martinot A, Grandbastien B, Leteurtre S, Duhamel A, Leclerc F. No resuscitation orders and withdrawal of therapy in French paediatric intensive care units. Groupe Francophone de Réanimation et d’Urgences Pédiatriques. Acta Paediatr. 1998;87:769–73. doi: 10.1080/080352598750013860. [DOI] [PubMed] [Google Scholar]
- 28.Goh AY, Mok Q. Identifying futility in a paediatric critical care setting: A prospective observational study. Arch Dis Child. 2001;84:265–8. doi: 10.1136/adc.84.3.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Devictor DJ, Nguyen DT. Groupe Francophone de Réanimation et d’Urgences Pédiatriques. Forgoing life-sustaining treatments: How the decision is made in French pediatric intensive care units. Crit Care Med. 2001;29:1356–9. doi: 10.1097/00003246-200107000-00010. [DOI] [PubMed] [Google Scholar]
- 30.Althabe M, Cardigni G, Vassallo JC, Allende D, Berrueta M, Codermatz M, et al. Dying in the intensive care unit: Collaborative multicenter study about forgoing life-sustaining treatment in Argentine pediatric intensive care units. Pediatr Crit Care Med. 2003;4:164–9. doi: 10.1097/01.pcc.0000059428.08927.a9. [DOI] [PubMed] [Google Scholar]
- 31.Kipper DJ, Piva JP, Garcia PC, Einloft PR, Bruno F, Lago P, et al. Evolution of the medical practices and modes of death on pediatric intensive care units in southern Brazil. Pediatr Crit Care Med. 2005;6:258–63. doi: 10.1097/01.PCC.0000154958.71041.37. [DOI] [PubMed] [Google Scholar]