

Abstract
Extra-cranial schwannomas although common in head and neck region are very rarely seen originating from the infra-orbital nerve. We report a case of schwannoma arising from infra-orbital nerve in a 40-year-old male patient. The case presented as an isolated, asymptomatic, slow growing sub-cutaneous nodular swelling over left side of mid-face. On ultrasonography, a localized lesion within the sub-cutaneous tissue of cheek was observed, without involvement of orbital, maxillary sinus or underlying bone. Aspiration biopsy of the lesion showed spindle shaped cells predominantly arranged in Antoni A pattern around verocay bodies, with less organized Antoni B tissue in few places. Diagnosis of schwannoma, probably arising from terminal branch of infra-orbital nerve was established. The tumor was approached through skin incision. At the time of exploration, the lesion was found to emanate from the nerve trunk of peripheral branch of infra-orbital nerve, which was dissected and preserved. We correlate our experience with previously reported cases of infra-orbital nerve schwannoma.
Keywords: Infra-orbital nerve, mid-face, schwannoma, swelling
INTRODUCTION
Schwannoma is a benign tumor arising from neuroectodermal schwann cell of cranial, intraspinal, peripheral and autonomic nerve sheaths.[1] Lesions in head and neck region account for 25-45% of extra-cranial schwannomas.[2] However, it rarely involves infra-orbital nerve and are uncommon in the maxillary and buccal space.[3] These tumors usually present as slow growing nodular mass and can mimic any benign growth in the head and neck. The treatment of extra-cranial head and neck schwannomas is surgical and the approach depends on the location and extent of the tumor and the nerve involved.
This paper describes a case of schwannoma arising from infra-orbital nerve, presenting as slow growing nodular swelling in the buccal space. The lesion was approached through skin incision and completely resected. At the time of exploration, the lesion was observed to emanate from the nerve trunk of peripheral branch of infra-orbital nerve, which was dissected and preserved. Only nine cases of infra-orbital nerve schwannoma are previously reported, which we discuss in relation to our experience.
CASE REPORT
A 40-year-old male patient presented with a chief complaint of painless swelling over left side of face. The patient first noticed the swelling about a year back, which had grown gradually to its present size. Patient also complained of mid paresthesia over left cheek since past few months. On examination, a localized, nontender, firm, round swelling of about 4 cm was evident over left side of mid-face, extending from below the infra-orbital margin to upper lip [Figure 1]. The overlying skin appeared stretched and tense. The skin was pinch-able over the lesion, except at the center of the lesion. The naso-labial fold was obliterated. Intra-oral examination showed no swelling over anterior maxilla. The maxillary anterior teeth were firm and nontender on percussion. There was no proptosis and vision was normal. The cervical lymph nodes were not palpable. No significant medical history or history of previous trauma was reported. The overall clinical presentation was suggestive of a benign sub-cutaneous lesion and differential diagnosis included lipoma, fibroma, dermoid cyst, epidermoid cyst and neurogenic tumor.
Figure 1.

Lesion presenting as large sub-cutaneous nodular swelling
Ultrasonography was advised to study nature, size and extent of the lesion. The ultrasonogram showed well-defined, heterogeneous oval mass of 45 mm × 30 mm × 23 mm within the buccal sub-cutaneous tissue with no orbital, maxillary sinus or underlying bone involvement [Figure 2]. Aspiration biopsy of the lesion showed spindle shaped cells predominantly arranged in Antoni A pattern around verocay bodies, with less organized Antoni B tissue in few places [Figure 3]. Diagnosis of schwannoma, probably arising from terminal branch of infra-orbital nerve was established.
Figure 2.
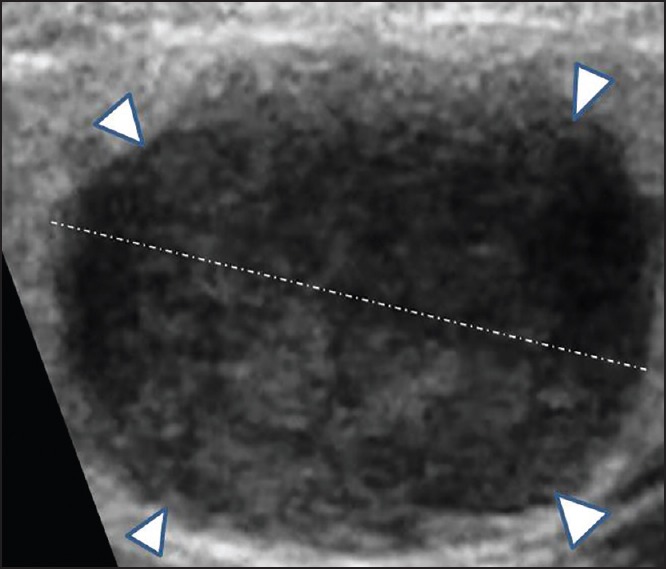
Ultrasonogram showing a heterogeneous oval mass within the sub-cutaneous tissue
Figure 3.
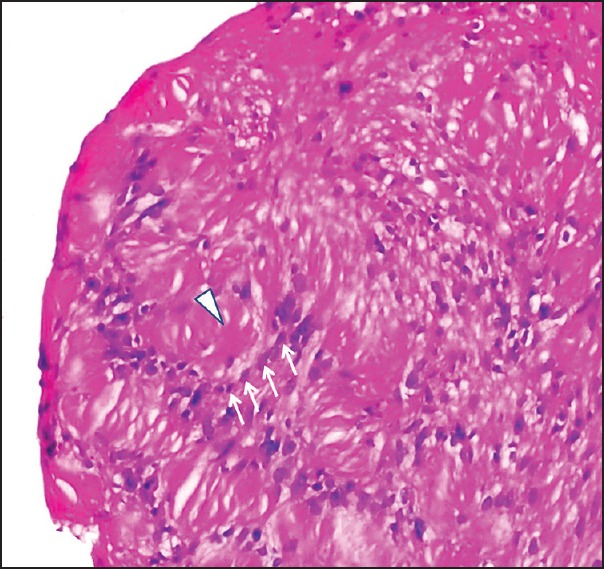
H and E stained section of aspirate showing verocay bodies (arrow head) surrounded by spindle shaped cells arranged in orderly parallel fashion (arrows)
Surgical excision of the lesion was planned and executed under local anesthesia. After attaining adequate anesthesia, linear incision of about 3 cm was placed over skin along the natural skin crease of naso-labial fold. The lesion was well-encapsulated, and freed from surrounding tissue by blunt dissection [Figure 4a]. Portion of skin overlying the center of the lesion appeared thinned and was included in the excised nodule. At the time of exploration, the lesion was found to emanate from the nerve trunk of peripheral branch of infra-orbital nerve, which was dissected and preserved [Figure 4b]. Histopathological examination of the excised lesion confirmed diagnosis of schwanomma [Figure 5].
Figure 4.
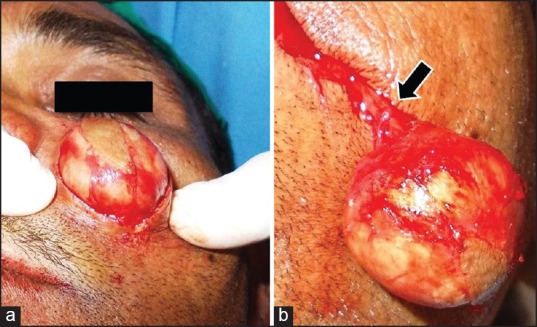
(a) Exposure of the lesion through skin incision; (b) dissected tumor attached to the nerve trunk of peripleral branch of infra-orbital nerve (block arrow)
Figure 5.
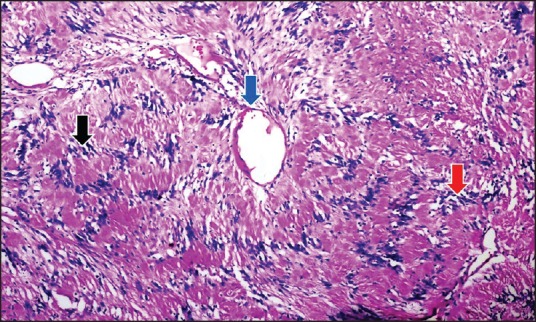
H and E stained section (×10) of excised specimen showing spindle shaped cells predominantly arranged in Antoni A pattern around verocay bodies (black arrow), with less organized Antoni B tissue in few places (red arrow). Vessel in schwannoma having wide lumen, fibrotic wall and adjacent hyalinization (blue arrow)
DISCUSSION
Schwannoma (neurinoma, peripheral glioma, perineural fibriblastoma and neurilemmoma) is ectodermal benign neoplasm, which originates from schwann cell of cranial, intraspinal, peripheral and autonomic nerve sheaths. They are common in head and neck region, accounting for 25-45% of extra-cranial schwannomas and 1-8% of all head and neck tumors.[4] It can involve any of the 12 cranial nerves, except the olfactory and optic nerves since they lack schwann cells in their sheaths.[5,6] Schwannoma arising from infra-orbital nerve (branch of maxillary division of fifth cranial nerve) is extremely rare. To best of our knowledge, only nine cases of infra-orbital schwannoma has been previously described in English literature.[3,7,8,9,10,11,12,13,14]
Schwannoma generally presents as slow growing painless sub-cutaneous or submucosal swelling. Depending on the site of nerve trunk or branch from which it arises, it may be located within the lower part of orbit,[7,8,9] maxillary sinus[3] or present as sub-cutaneous mass in infra-orbital region[10,11,12] [Table 1]. Intraorbital schwannoma generally develop from supraorbital or supratrochlear nerves, and less frequently from infra-orbital nerves.[9] Lesions arising from infra-orbital nerve grow to involve surrounding structures such as maxillary sinus, nasal cavity, infratemporal fossa and pterygopalatine fossa.[13,14] However, it is rare to find schwannoma in the paranasal sinus, especially in the maxillary sinus.[15] Swelling in the cheek, nasal atresia, downward transversion of the palate and pain, rarely accompanying exophthalmosis are common symptoms. However in our case, a well-localized painless infra-orbital sub-cutaneous swelling was observed without any ocular lesions or involvement of underlying osseous skeleton.
Table 1.
Review of previously reported cases of schwannoma involving ION*
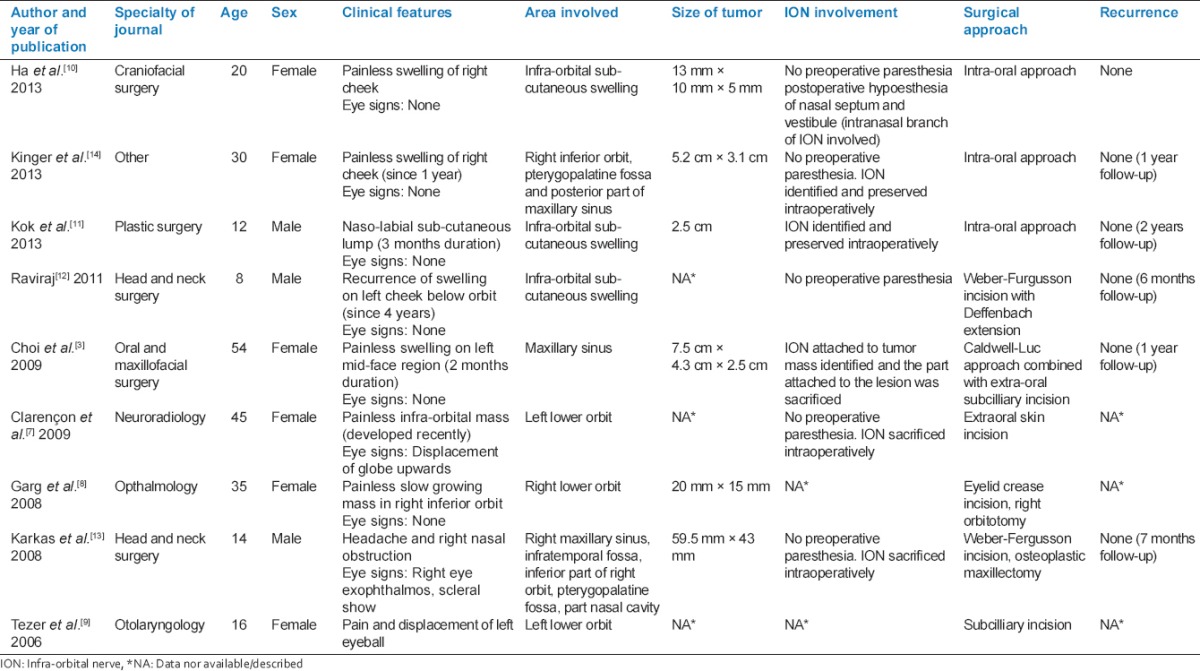
Rarely schwannomas may present with numbness in the distribution of involved nerve or with pain.[16] Our patient reported paresthesia localized over area of distribution of superior labial branch of infra-orbital nerve, which was probably due to pressure or direct involvement of the peripheral branch of the nerve. However during the surgical dissection, lesion was found to emanate from the nerve trunk of peripheral branch of infra-orbital nerve, which was dissected and preserved. None of the previous cases of infra-orbital schwannoma reported preoperative paresthesia [Table 1].
Fine-needle aspiration cytology (FNAC), ultrasonography, magnetic resonance imaging and computed tomography image are diagnostic tools for schwannoma. Diagnosis using FNAC is characterized by the presence of spindle cells and has only 17.6% accuracy.[17] Aspiration of our lesion yielded blood tinged aspirate, which showed spindle shaped cells predominantly arranged in Antoni A pattern around verocay bodies, with less organized Antoni B tissue in few places confirming the diagnosis of schwanomma.
The treatment of schwannomas is exclusively surgical and the appropriate approach is dictated by the extent and location of the tumor. In our case, the tumor originated from the peripheral branch of infra-orbital nerve and presented as nodular swelling immediately underlying the skin. Incision placed in the natural skin crease of naso-labial fold was used to approach and completely remove the lesion. Other approaches used include intra-oral vestibular incision for smaller lesions localized in the buccal space,[10,11,14] Caldwell-Luc approach for tumor within the maxillary sinus,[3] Subcilliary or eyelid crease incision for intraorbital schwannoma.[8,9] Larger lesion involving greater areas of mid-face are treated by extra-oral Weber-Furgusson incision combined with ostectomy[13] [Table 1]. Although malignant transformation and recurrence of schwannoma is very low, a case of recurrent infra-orbital schwannoma[12] attributed to incomplete removal of the lesion through a limited skin incision was reported.
CONCLUSION
Schwannoma arising from the infra-orbital nerve is rare, making the clinical diagnosis often difficult. Although uncommon, schwannoma involving the peripheral branch of infra-orbital nerve may present as localized mid-face swelling and should be included in differential diagnosis of benign sub-cutaneous swelling in infra-orbital region.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Marx RE, Stern D. United States Quintessence Publishing Co. Inc. 2nd ed 2003. Oral and Maxillofacial Pathology: A Rationale for Diagnosis and Treatment. [Google Scholar]
- 2.Samet A, Podoshin L, Fradis M, Simon J, Lazarov N, Boss H. Unusual sites of schwannoma in the head and neck. J Laryngol Otol. 1985;99:523–8. doi: 10.1017/s0022215100097176. [DOI] [PubMed] [Google Scholar]
- 3.Choi BH, Park SW, Son JH, Cho YC, Sung IY, Byun KJ, et al. Schwannoma in the maxillary sinus and buccal space: Case report. J Korean Assoc Oral Maxillofac Surg. 2009;35:494–8. [Google Scholar]
- 4.Yoon E, Rhee SC. Solitary trigeminal schwannoma of paranasal region. Int J Pediatric Otorhinolaryngol Extra 01. 2007;2:120–4. [Google Scholar]
- 5.Leu YS, Chang KC. Extracranial head and neck schwannomas: A review of 8 years experience. Acta Otolaryngol. 2002;122:435–7. doi: 10.1080/00016480260000157. [DOI] [PubMed] [Google Scholar]
- 6.Katz AD, Passy V, Kaplan L. Neurogenous neoplasms of major nerves of face and neck. Arch Surg. 1971;103:51–6. doi: 10.1001/archsurg.1971.01350070077018. [DOI] [PubMed] [Google Scholar]
- 7.Clarençon F, Jafari A, Lefevre M, Périé S, Angelard B, Marsault C, et al. Infraorbital nerve schwannoma. J Neuroradiol. 2009;36:301–3. doi: 10.1016/j.neurad.2009.02.006. [DOI] [PubMed] [Google Scholar]
- 8.Garg R, Dhawan A, Gupta N, D’Souza P. A rare case of benign isolated schwannoma in the inferior orbit. Indian J Ophthalmol. 2008;56:514–5. doi: 10.4103/0301-4738.43380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tezer MS, Ozcan M, Han O, Unal A, Ozlugedik S. Schwannoma originating from the infraorbital nerve: A case report. Auris Nasus Larynx. 2006;33:343–5. doi: 10.1016/j.anl.2005.11.015. [DOI] [PubMed] [Google Scholar]
- 10.Ha W, Lee JW, Choi J, Yang SW, Kim SY. Schwannoma originating from infraorbital nerve. Arch Craniofac Surg. 2013;14:61–4. [Google Scholar]
- 11.Kok YO, Yeo MS, Nallathamby V, Lee SJ. Infraorbital nerve schwannoma presenting as an upper lip mass in an adolescent boy. Ann Plast Surg. 2013;71:196–7. doi: 10.1097/SAP.0b013e318248b8a2. [DOI] [PubMed] [Google Scholar]
- 12.Raviraj GA, Thomas R, Dhanraj GA, Rao US. Pediatric infraorbital nerve schwannoma: A rare clinical entity. Int J Head Neck Surg. 2011;2:73–5. [Google Scholar]
- 13.Karkas AA, Schmerber SA, Bettega GV, Reyt EP, Righini CA. Osteoplastic maxillotomy approach for infraorbital nerve schwannoma, a case report. Head Neck. 2008;30:401–4. doi: 10.1002/hed.20702. [DOI] [PubMed] [Google Scholar]
- 14.Kinger A, Kawatra M, Chaudhary TS, Chaudhary A. Plexiform schwannoma of infraorbital nerve – A rare case report. Int J Bioassays. 2013;02:534–6. [Google Scholar]
- 15.Sarioglu S, Ozkal S, Güneri A, Ada E, Sis B, Erdag TK, et al. Cystic schwannoma of the maxillary sinus. Auris Nasus Larynx. 2002;29:297–300. doi: 10.1016/s0385-8146(02)00009-3. [DOI] [PubMed] [Google Scholar]
- 16.Dervin JE, Beaconsfield M, Wright JE, Moseley IF. CT findings in orbital tumours of nerve sheath origin. Clin Radiol. 1989;40:475–9. doi: 10.1016/s0009-9260(89)80250-8. [DOI] [PubMed] [Google Scholar]
- 17.Salemis NS, Karameris A, Gourgiotis S, Stavrinou P, Nazos K, Vlastarakos P, et al. Large intraparotid facial nerve schwannoma: Case report and review of the literature. Int J Oral Maxillofac Surg. 2008;37:679–81. doi: 10.1016/j.ijom.2008.01.018. [DOI] [PubMed] [Google Scholar]