

Abstract
Background
Due to cost-containment efforts, preparation programs for outpatient surgery are currently not available to the majority of children and parents. The recent dramatic growth in the Internet presents a unique opportunity to transform how children and their parents are prepared for surgery. In this article we describe the development of a Web-based tailored preparation program for children and parents undergoing surgery (WebTIPS).
Development of Program
A multidisciplinary taskforce agreed that a Web-based tailored intervention comprised of intake, matrix and output modules was the preferred approach. Next, the content of the various intake variables, the matrix logic and the output content was developed. The output product has a parent component and a child component and is described in http://surgerywebtips.com/about.php. The child component makes use of preparation strategies such as information provision, modeling, play and coping skills training. The parent component of WebTIPS includes strategies such as information provision, coping skills training, relaxation and distraction techniques. A reputable animation and Web-design company developed a secured Web-based product based on the above description.
Conclusions
In this article we describe the development of a Web-based tailored preoperative preparation program that can be accessed by children and parents multiple times before and after surgery. A follow-up article in this issue of Anesthesia & Analgesia describes formative evaluation and preliminary efficacy testing of this Web-based tailored preoperative preparation program.
Introduction
Over the past 2 decades, increasing numbers of pediatric surgeries have been performed in an outpatient setting in the United States.1 Unfortunately, with this shift, the number of children who have access to preoperative preparation has significantly decreased. Whereas in the past about 80% of children underwent preoperative preparation several days before undergoing surgery in a children's hospital setting,2 one survey reported that 90% of a sample of community hospitals currently offer no pediatric preoperative preparation programs for surgery.3 The survey also found that although 70% of children's hospitals currently offered inpatient preoperative child life services, only 20% of children's hospitals offered preoperative preparation for outpatient children before the day of surgery. This is problematic since hospital-based preoperative preparation programs have been shown to decrease preoperative anxiety in children and their parents.4-6
As a substitute for undergoing a preparation program several days before surgery, hospitals have now introduced preoperative programs on the morning of surgery. This is problematic because children and parents are highly anxious in the preoperative area and thus their ability to benefit and process information is limited.7 Further, a video-capture study documented that healthcare providers spend, on average, 3-5 minutes communicating with families in the holding area on the day of surgery.8
The recent dramatic growth in the use of the Internet provides an opportunity to create an innovative World Wide Web (Web) based intervention that can be accessed multiple times during the perioperative period and that integrates evidence-based treatments for reducing preoperative anxiety and improving postoperative pain. The Internet is a global system of interconnected computer networks that use the standard Internet protocol suite (TCP/IP).The Web is a system of interlinked hypertext documents accessed via the Internet.
Over the past decade, tailoring behavioral interventions has been reported in a variety of settings. The rationale for tailoring behavioral interventions is that a one-size-fits-all approach is not appropriate for everyone because it leads to messages that are not directly relevant to the patient. In contrast, by tailoring materials, superfluous information is eliminated and the remaining information is relevant and is more likely to have an effect.9 Web-based tailoring is a new modality that has gained traction and recognition in healthcare during the last decade.10-14 This modality has been shown to be effective in areas such as smoking,15 breast cancer screening,16 and healthier diets.12,15,17,18 However, no tailored interventions have been developed to prepare children and their parents for the surgical experience.
The purpose of this first article is to describe the development of an innovative Web-based tailored intervention program called WebTIPS that is directed at preparing children and parents for undergoing anesthesia and outpatient surgery. An accompanying article in this issue of Anesthesia & Analgesia will describe formative evaluation and initial efficacy testing of WebTIPS.19
Development of Program
Development of this intervention began with a task force of anesthesiologists, psychologists, surgeons, nurses, pediatricians, child-life specialists, parents and children. The general pediatric surgeon and orthopedic surgeon had more than 20 years experience and the otolaryngological surgeon had 8 years experience. This task force met over a period of 6 months to determine the specific needs of the child-parent dyad within the context of the perioperative environment. The extended task force concluded that the following characteristics were essential to an ideal surgical preparation program for children undergoing outpatient surgery:
1) The ideal intervention must be grounded in the most contemporary evidence-based medicine. 2) The ideal intervention must be accessible to most children and parents. Indeed, over the past 2 decades, access to the Internet has dramatically increased in every segment of the American population. The Pew Internet Projecta conducted in the United States in January 2014 showed that 97% of adults age 18-29 years and 93% of adults age 30-49 are Internet users.20 Also, the Internet is being used by 76% of adults who are high school graduates or less and 97% who are college graduates.
3) Conceptually, interventions can be divided into generic, personalized and tailored. An example of generic preoperative information is an information leaflet. An example of a personalized preoperative intervention is a child life program which is likely personalized based on the age and gender of the child but does not consider more subtle personality characteristics. In contrast, a preoperative tailored intervention can consider multiple variables that are unique to a particular individual and have been shown to affect the desired outcome of reduced anxiety. A tailored intervention typically includes 3 elements: an intake, a matrix and an output.14 Within the context of preparation of children for surgery, ideally the intake should obtain predetermined individual characteristics of the child-parent dyad that would allow tailoring the intervention to the specific characteristics of the dyad. The data needed for tailoring can be obtained directly from an existing source or entered manually by the parent. The matrix typically functions behind the scenes to sort the child-parent dyads into appropriate categories and match the output of the intervention to the specific child-parent dyad. The output typically includes the content that we would like to be delivered to the specific child-parent dyad.11-13,15,21,22 Overall, tailored interventions are more effective in changing behavior than generic or personalized interventions.23 4) The intervention must be inexpensive. It seems intuitive that a Web-based intervention would be markedly less expensive than a hospital-based preparation program. 5) The intervention can provide behavioral data about the child and parent to healthcare providers before the day of surgery. In this way the providers are more prepared to interact with the child and parent the first time they meet with them.
It is also important to note that the conceptual framework and content WebTIPS was examined by a behavioral medicine, interventions, outcomes expert panel which is part of the Center for Scientific Review at the National Institutes of Health. Indeed, WebTIPS was revised several times based on their input. After the identification of these principles, the taskforce started the development of a tailored intervention that was based on the 3 components of intake, matrix and output.
Intake Component of WebTIPS
As a first step, an extensive literature review was conducted to ascertain child and parent individual characteristics that are reported to affect the efficacy of interventions to manage perioperative anxiety and pain. Because of the behavioral complexity of an intervention that would be developmentally appropriate to children of different ages, we decided to limit the overall intervention to 2-7 years. Also, because of developmental considerations we have appreciated that it would be difficult for a child younger than 4 years of age to interact and be engaged in modeling, information provision and coping skills with a Web-based program. As such, the child's part of WebTIPS was designed for children 4-7 years, whereas the parent part is appropriate for parents of children 2-7 years. The task force also decided that this intervention will be generalized to all children undergoing outpatient surgery and not be limited to children of certain ASA classification. WebTIPS was designed for parents who read English at the level of at least 8th grade. It is also important to note that WebTIPS is a stand-alone Internet application that does not interact with the electronic health record or any of the systems of the hospitals and ratherall data are manually entered by the parents.
After deciding on the appropriate individual characteristics that are needed for optimal tailoring, it was necessary to identify the most appropriate assessment tools for those tailoring variables. The taskforce concluded based on input from parents that the intake component should not take longer than 3-7 minutes to be completed by the parents. To address the issue of manual data entry, where required, the task force revised assessment tools to maximize their use within the clinical environment.
Parent and Child Tailoring Variables
Construct description and how the output of the intervention is adjusted based on the results of the intake are presented in Table 1.
Table 1. Details of how WebTIPS is tailored.
| Tailoring Variables | Construct Description | How WebTIPS output is adjusted |
|---|---|---|
| Parent Characteristics | ||
| Coping Style (Measured by MBSS short form) | ||
| High Monitor | Seek out and attend to health-related information | Comprehensive information provided (applied to all content) |
| Low Monitor/Blunter | Distract from health information Prefer minimal details of threat | Concise, benefit focused (applied to all content) |
| Anxiety (Measured by STAI trait form) | ||
| High | High emotional reactivity in response to anticipation of real or imagined threat | Detailed information on identifying and managing own anxiety (training in behavioral and cognitive coping) |
| Low | Low emotional reactivity to real or imagined threat | Acknowledgement of anxious feelings |
| Concise information on distraction with options to access additional information if desired | ||
| Pain Medication Attitudes (measured by MAQ) | ||
| Endorsement of misconceptions regarding pain management | Information to challenge specific misconception | |
| Induction of Anesthesia Intervention Preference | ||
| Parental Presence | Desire to accompany child to operating room | Information on what to expect in the operating room |
| Behaviors to engage in and to avoid in the operating room | ||
| Midazolam | Desire to have child receive sedative premedication | What to expect when child has midazolam (sleepy, silly) |
|
| ||
| Child Characteristics | ||
| Fearfulness (Measured by CBQ Fear subscale) | ||
| High | High levels of worry or nervousness related to anticipated pain or distress | Reassurance, focus on gentle approaches to gaining compliance modeling of coping skills (distraction, breathing) |
| Low | Low levels of worry or nervousness More likely to show approach behaviors in novel situations | Concise information about surgical environment, tailored modeling of coping skills by child animated character (character demonstrating approach behaviors) |
| Surgical Procedure | ||
| Surgical procedure the child will undergo | Appropriate pain expectations for recovery room and at home and appropriate directions for analgesics | |
| Expectations about activity at home following surgery | ||
Note. WebTIPS = Web-based Tailored Intervention for Preparation of parents and children undergoing Surgery; MBSS = Miller Behavioral Style Scale; STAI = State-Trait Anxiety Inventory; CBQ = Child Behavioral Questionnaire; MAQ = Medication Attitude Questionnaire
Anxiety
The most widely used instrument to assess trait anxiety in adults is the State-Trait-Anxiety-Inventory (STAI24). This instrument, however, consists of 20 items and takes at least 6-8 minutes to complete. To shorten this instrument for use in clinical settings, we made use of our extensive database of 2500 data points. Items with the highest correlations with the STAI total scores in the database and face validity were selected for the shortened version (10 items). We next enrolled 48 parents of children undergoing surgery and asked them to complete both the original instrument and the shortened instrument on a laptop computer. We achieved adequate correlation coefficients of 0.87 to 0.91 between the total score of the original and revised scale.b
Parental Coping Style
The Monitor/Blunter framework developed by Miller and colleagues,25,26 indicates that individuals who are high “monitors” review health-related information and respond better to information than to lack of information.27-29 Blunters respond best to short messages that are directed and do not include statistics or figures.29 For the purposes of tailoring WebTIPS, a shortened version of the Miller Behavioral Style Scale was used that was developed by Williams-Piehota et al. and demonstrated adequate reliability and validity.29
Parental Pain Management Attitudes
In order to tailor the intervention based on this variable we decided to use the Medication Attitudes Questionnaire30 which was developed to examine attitudes about using pain medication for treating children's pain. Based on our previous studies31-33 we chose to include the 5 pain-management misconceptions most frequently endorsed by parents. These include: Side Effects are something to worry about when giving children pain medication; When giving children pain medication, one should be concerned about addiction or later abuse; Pain medication works best when taken rarely and for the worst pain; Children feel less pain than adults; and Children in pain will express themselves by crying or whining.
Induction of Anesthesia Intervention Preference
it is also important for WebTIPS to provide data that are specific to the type of perioperative intervention that a parent requests for their child. The most common interventions to be used during induction of anesthesia are parental presence at anesthesia induction and preoperative sedative premedication,34 thus questions about parental preference for both interventions were included in the intake.
Fearfulness
Child fearfulness was assessed using the fearfulness scale of the Children's Behavior Questionnaire-Short Form 35(Table 1).
Type of Surgery
We surveyed 6 pediatric surgeons of various specialties and incorporated their suggestions for postoperative pain management based on the particular surgery.
Matrix Component of WebTIPS
The matrix component of WebTIPS functions behind the scenes to assure a specific output is provided to a specific child-parent dyad.
Parent and Child Variables
Anxiety
After an examination of the literature we concluded that a median split was the most meaningful cutoff between anxiety groups as assessed by the modified STAI.
Coping style
Consistent with the methodology of Williams-Piehota et al., participants with scores above the median of 4 are categorized as “high monitors.”29
Parent Pain Management Attitudes
Parents endorsing any pain misconception with a score of higher than 3, receive education about that particular belief.
Temperament
Based on data from the Children's Behavior Questionnaire-Short Form, the mean score on the fear subscale is 3.99. Children above this mean are classified as “high fear.”
Type of Surgery
Based on type of procedure the child is undergoing, the output will contain pain and recovery expectations and information specific to the surgical condition (Figure 1).
Figure 1.
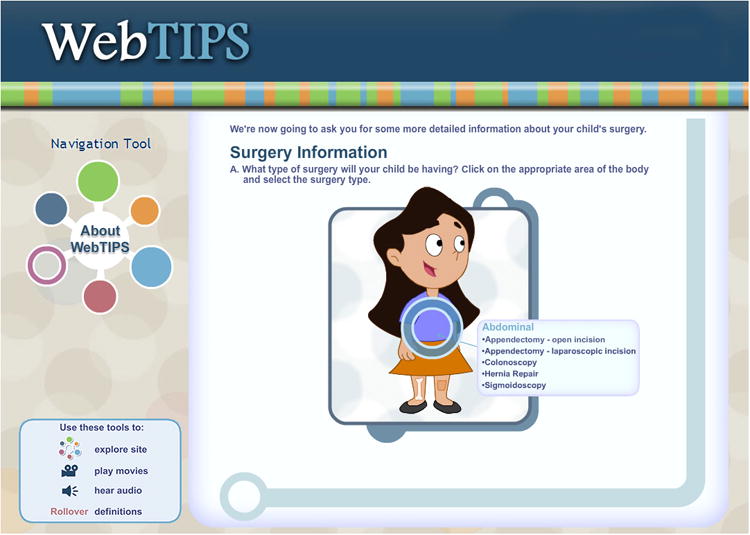
Section of the intake in which parents select their child's surgery using the character Anna from the child's Website.
Output Component of WebTIPS
Overall, the output component is divided into 4 modules: 1) Home before surgery; 2) Holding area and anesthesia induction; 3) Recovery room; and 4) Home after surgery. Each output module contains a parent component and a child component, with various educational and anxiety management skills included in each (Figure 2). Parents first access the parent Website and once completed, access is given to the child Website, which is intended for parents to complete with their children. Relevant information is accessible via a clinician Web-based module before the day of surgery to view parent and child data relevant to the perioperative management of the child. An appreciation of WebTIPS is best achieved by accessing http://surgerywebtips.com/about.php.
Figure 2.
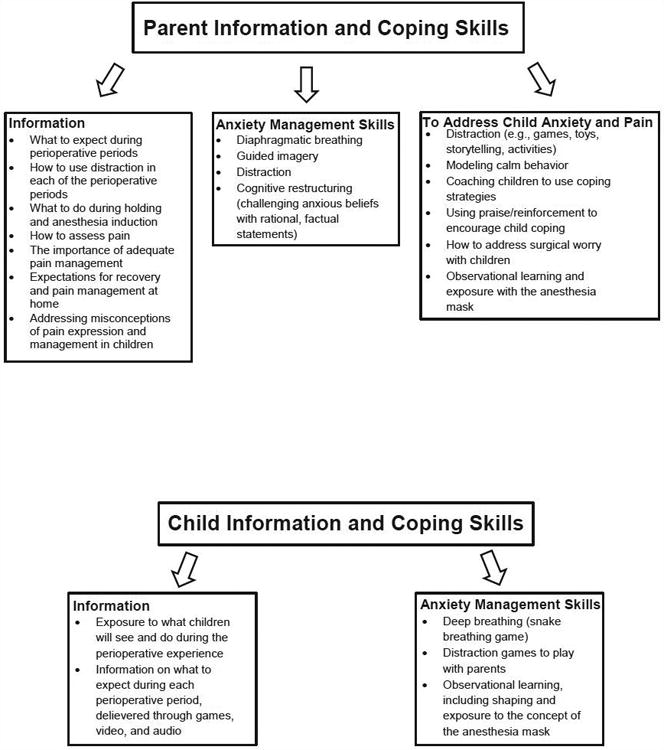
Description of the informational topics and coping strategies provided in the parent and child component of Web-based Tailored Intervention for Preparation of parents and children undergoing Surgery (WebTIPS).
Parent Website
The parent component of WebTIPS includes 2 primary strategies: information provision and coping skills training. Information provided to parents is presented in both audio and visual formats, including video, text, motion graphics, and audio clips.
Preoperatively at Home
After an introduction detailing what parents will find throughout this module, parents are provided information regarding how to prepare for their child's upcoming surgery, from basic information about the importance of good sleep and nutrition to specific information to address common child and parent anxieties about surgery [e.g., I will have to leave my child (parent), will I get any needle pokes? (child)]. Parents are then guided through several self-management anxiety management exercises, including deep breathing and imagery using both audio and visual information (Figure 3). One of the most effective strategies of preparing a child for surgery is behavioral shaping and exposure to the anesthesia mask before surgery;36 therefore, this module contains a 10-step behavioral shaping tutorial for parents to practice exposing their child to the anesthesia mask. Finally parents were provided information specific to the morning of surgery, such as a review of overnight fasting (NPO) guidelines, directions to the hospital/surgery center, and information about hospital registration (Figure 4). This part of the module will change based on the particular details of the hospital that is using the program.
Figure 3.
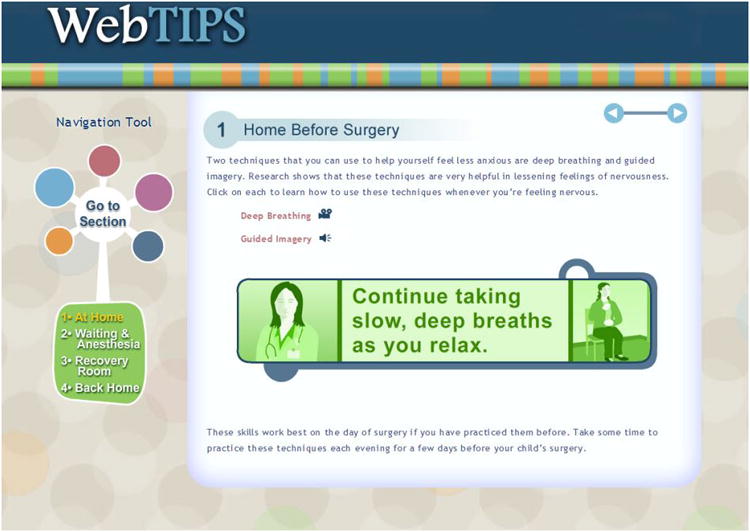
Screen shot of the Home Before Surgery output module for parents illustrating relaxation strategies provided via audio and video modalities.
Figure 4.
Screen shot of the introductory movie of the child component of Web-based Tailored Intervention for Preparation of parents and children undergoing Surgery (WebTIPS) illustrating the animated narrators of the program, Billy Bot and his sidekick Tot Bot, as well as the main characters of the Website, Anna and her parents.
Preoperative Holding Area, Anesthesia Induction, and Surgery
Parents are provided with information and with behavioral strategies to manage their child's anxiety (e.g., distraction) in both the preoperative holding area and during anesthesia induction. These strategies are aimed to increase child comfort and compliance with the induction progress (e.g., breathing games, coaching child to engage in coping).
A major component of this section is specific information on using distraction to manage child anxiety. Parents are provided with video examples of the characters from the child Website (Anna and her parents) engaged in distraction and a variety of distracting “games” that parents can use with young children to both distract their attention away from distressing stimuli and engage children in coping and breathing into the anesthesia mask. After discussion of sedative premedication such as midazolam and parental presence at anesthesia induction, parents are provided with information specific to anesthesia induction, such as what to expect and strategies to manage their child's anxiety (e.g., use of eye contact and calm, soothing voice; following lead of anesthesiologist). Finally, parents are reminded of the parental anxiety management techniques that were first introduced during the preoperative period.
Postanesthesia Care Unit (PACU)
In addition to pharmacological management, this module provides parents with specific instructions on the implementation of behavioral strategies to minimize pain and distress. Parents are first provided with expectations for PACU recovery and the PACU environment. Information about pain assessment and management by hospital staff is provided followed by instruction in the use of distraction and other behavioral strategies specific to the PACU. It is important to note that this module is tailored based on the responses of parents to the Medication Attitudes Questionnaire that was administrated in the intake section.
Postoperatively at Home
This module extends the utility of this preparation program to management of children's pain at home. In addition, general expectations for clinical and behavioral recovery are provided based upon the child's specific surgery. Parents are instructed in general principles of pain assessment (e.g., focus on behavioral cues), as well as information on pharmacological and behavioral management of children's pain. Any misconceptions regarding pain expression and analgesic use for children reported by parents during intake are addressed in this section as well as a thorough review of distraction techniques.
Child Website
The child Website is age-appropriate, fully animated, includes games and videos to teach concepts such as a game for breathing slowly for a calm body (Figure 5), and a memory game to prepare children for what they may see in the operating room. The site makes use of 3 strategies that have been previously used in preoperative preparation programs: a) information provision; b) modeling; c) and coping skills teaching. In order for the child to identify with the animated figures displayed in the Website, we designed a set of unique animated characters that were gender and ethnic neutral. The main character, Billy Bot, and his sidekick Tot Bot help the user to navigate the experience, alleviate anxiety and model prescribed coping behaviors and humor. The child, Anna, experiences the entire perioperative process in videos and games for children to observe. Based on the fear level of the child, Billy Bot provides more or less information about the surgical process and Anna displays more or less fearful responses throughout the process (tailoring). The child needs to learn about the process, feel safe with the adults around him/her and know what to do to manage anxiety. Children progress through each of the 4 video sequences reflecting the temporal divisions of surgery in order, and are prompted throughout to play 4 different games (placing the anesthesia mask on animals to provide exposure to the mask; a breathing game to practice calm, deep breathing; a search and find game to introduce children to objects to be encountered in the operating room; a memory game to introduce children to objects in the PACU) (Figure 6). The games are designed to model, reinforce, and practice the strategies covered. Children are also provided with various printable activities, including coloring sheets and a certificate of completion from the program.
Figure 5.

Screen shot of the videos of the child component of Web-based Tailored Intervention for Preparation of parents and children undergoing Surgery (WebTIPS), including the three games designed to get children familiar with the anesthesia mask, the operating room (OR), and the postanesthesia care unit (PACU), as well as the 4 videos that provide children information and coping strategies for each of the sections of the output (Home Before Surgery, Waiting Area & Anesthesia Induction, Recovery Room, and Home After Surgery).
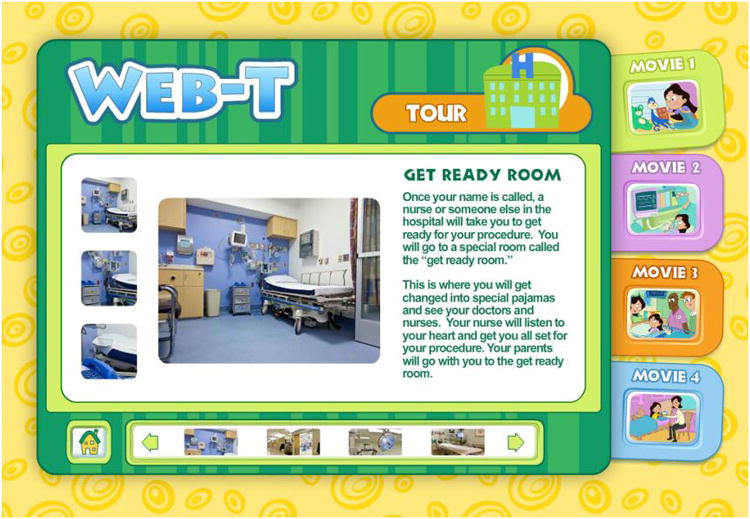
Figure 6.

Screen shot of the tour section of the child component of Web-based Tailored Intervention for Preparation of parents and children undergoing Surgery (WebTIPS) illustrating the “get ready room” (preoperative holding area) to prepare children for what they will see and do on the day of surgery.
Technical Development Considerations
As a first step we requested and received 3 proposals from highly reputable Web design and animation companies. After long consideration we selected Data Motion Arts from New York City as the producer for this intervention. The company has previously produced interactive CDs and Websites for clients such as Scholastic Media, Fisher-Price, Public Broadcasting Service and Nickelodeon. Data Motion Arts used its expertise in this area and built the site from the ground up including architecture, technical protocol specification, customized database, user profile matrix modules, image and text content generators, animation, security and encryption, data compilers, and customized reporting generators. Finally, security for WebTIPS includes a Secure Socket Layer certificate allowing for 128 bit encryption between client and server transactions. All data are stored and accessed in accordance with the Health Care Financing Administration's Security Policy and the Health Insurance Portability and Accountability Act. Once the HTML prototype was completed, the animation and engineering phase of the Website was then built.
It is important to note that WebTIPS was developed to be accessed from any desktop computer rather than on a smartphone or tablet. Although it is possible to view WebTIPS from a smartphone or computer tablet with internet connection and Adobe Flash capabilities, the Web-based design has not yet been optimized for these devices. In addition, software used to restrict access to Websites or domains (e.g., parental controls) need not be disabled to run the WebTIPS application, allowing less restricted access.
Discussion
In conclusion, this article describes the development of the first Web-based tailored intervention that is directed at preparing children and parents for their surgery. At the end there was a clear group consensus for simplicity and construct validity of the intervention. The intervention is contemporary and fills a much-needed void in the area of preoperative preparation of children and parents undergoing outpatient surgery with discharge home on same day as surgery. Further, the accessibility offered by this Web-based program addresses availability limitations of traditional preparation programs; parents can continue to access up-to-date information after they have left the surgical center and when questions arise at home. One should note that WebTIPS is not intended to replace meeting with the pediatric anesthesiologist before surgery or the use of any other modality to reduce anxiety of the child-parent dyad. Instead, this is an additive intervention that is aimed to improve the care we provide our patients. Our follow-up article in this issue of Anesthesia & Analgesia documents the qualitative and quantitative analyses we conducted to test the usability and preliminary efficacy of WebTIPS.19
Several parts of the output of the intervention are particularly notable. First, parents and children work together to complete the child component, ensuring that parents also learn children's skills. In addition, “parent teaching” time is built into the program. At critical points in the child component (e.g., when deep breathing is introduced), the program pauses to instruct the parent and child to practice the skills together. A second, particularly notable part of the output is its focus on postoperative pain at home, a time period often neglected in typical preparation programs. In the parent component, parents are introduced to the importance of regular pain assessment and provision of adequate pain medication. It is notable that the pain management module of the intervention can be accessed by parents both before and after surgery.
The conceptual framework outlining this intervention is particularly innovative. That is, tailored intervention has been recognized as a “gold standard” as compared to generic intervention because it can address specific child needs.23 For example, recent evidence of parental attitudes as a barrier31 is addressed by providing information tailored to parents' unique misconceptions about pain-management strategies.
One important area that should be noted is that of data security. WebTIPS resides on a server and is constantly maintained by a computer programmer. This is because of recent security lapses for data security and sensitivity about the information that is provided by the child-parent dyad. The cost for an individual hospital will depend on the business model which will be used to disseminate WebTIPS. That is, there are a number of possible models such as WebTIPS that are maintained on a central server and hospitals will pay a licensing fee to the company that will operate the server based on the volume of children and parents that will view the program. Another possible model is for each hospital to purchase WebTIPS and implement it within its own servers or for professional societies like the Society for Pediatric Anesthesia or the American Society of Anesthesiology, who in turn might offer this program, at a greatly reduced price or even free to membership. As such, it is currently difficult to predict the exact cost of WebTIPS to a hospital or surgery center.
Finally, the current paradigm for behavioral preparation of children for outpatient surgery is based on generic interventions that are typically delivered on the morning of surgery. This very brief preparation (10-20 minutes) is generic, not evidence-based, and primarily addresses the issue of state anxiety and not pain and recovery after surgery. WebTIPS, which is Web-based, is a transformative alternative in that: 1) It is available 24-hours a day/7 days a week starting 5-days before surgery to 10 days after surgery; 2) It is tailored based on variables that have been shown to affect the response of the child and parent to pain and anxiety; 3) It is based on a well-established, rigorous development process; 4) It addresses the entire perioperative experience as a continuum including home before surgery, holding area before surgery, surgery, PACU, and home after surgery; 5) It has 2 distinct components directed to the parent and child; and 6) It provides nurses and anesthesiologists prior to the day of surgery with patient-specific information on children and parents that will allow for improved management of anxiety and pain on the day of surgery.
In the follow up article in this issue we detail data regarding formative evaluation and a preliminary randomized controlled trial.19
Acknowledgments
Funding: The National Institutes of Health funded this work with grant support (5R01HD056104-02, Zeev N. Kain)
Footnotes
Communication with Pew research center indicated that “These data were obtained from telephone interviews with a nationally representative sample of 1,006 adults living in the continental United States. Telephone interviews were conducted by landline (502) and cell phone (504, including 288 without a landline phone). The survey was conducted by Princeton Survey Research Associates International (PSRAI). Interviews were done in English and Spanish by Princeton Data Source from January 9 to 12, 2014. Statistical results are weighted to correct known demographic discrepancies. The margin of sampling error for the complete set of weighted data is ± 3.5 percentage points”.
Kain Z, MacLaren J, Wang S, Caldwell-Andrews A, Yaffa Zisk R, Mayes L. Facilitating perioperative research: Validity of short electronic measures for anxiety and temperament (abstract). American Society of Anesthesiology. Chicago, IL, 2006.
Disclosures:
Name: Zeev N. Kain, MD, MBA
Contribution: This author helped design the study and prepare the manuscript
Attestation: Zeev Kain approved the final manuscript. Zeev Kain attests to the integrity of the original data and analyses reported in this manuscript. Zeev Kain is the archival author.
Name: Michelle A. Fortier, PhD
Contribution: This author helped design the study and prepare the manuscript
Attestation: Michelle Fortier approved the final manuscript. Michelle Fortier attests to the integrity of the original data and analyses reported in this manuscript.
Name: Jill MacLaren Chorney, PhD
Contribution: This author helped design the study and prepare the manuscript
Attestation: Jill MacLaren Chorney approved the final manuscript.
Name: Linda Mayes, MD
Contribution: This author help design the study
Attestation: Linda Mayes approved the final manuscript.
The authors declare no conflicts of interest.
Contributor Information
Zeev N. Kain, Department of Anesthesiology and Perioperative Care, University of California, Irvine, Orange, California; UCI Center on Stress & Health, University of California, Irvine, Orange, California; Child Study Center, Yale University, New Haven, Connecticut.
Michelle A. Fortier, Department of Anesthesiology and Perioperative Care, University of California, Irvine, Orange, California; UCI Center on Stress & Health, University of California, Irvine, Orange, California.
Jill MacLaren Chorney, Departments of Anesthesiology, Pain Management and Perioperative Medicine, and Psychology, Dalhousie University and IWK Health Centre, Halifax, Nova Scotia.
Linda Mayes, Child Study Center, Yale University, New Haven, Connecticut; Departments of Pediatrics and Psychology, Yale University, New Haven, Connecticut.
References
- 1.Federation of State Medical Boards. [Accessed April 30, 2014];Report of the Special Committee on Outpatient (Office-Based) Surgery. 2002 Available at: http://www.fsmb.org/pdf/2002_grpol_Outpatient_Surgery.pdf.
- 2.O'Byrne K, Peterson L, Saldana L. Survey of pediatric hospitals' preparation programs: Evidence of the impact of health psychology research. Health Psychol. 1997;16:147–54. doi: 10.1037//0278-6133.16.2.147. [DOI] [PubMed] [Google Scholar]
- 3.Kain ZN, Wang SM, Caldwell-Andrews AA, Smith G, Saadat H. Pre-Surgical Preparation Programs for Children Undergoing Outpatient Surgery: Current Status. Anesthesiology. 2006;105:A955. [Google Scholar]
- 4.Kain ZN, Caramico LA, Mayes LC, Genevro JL, Bornstein MH, Hofstadter MB. Preoperative preparation programs in children: a comparative examination. Anesth Analg. 1998;87:1249–55. doi: 10.1097/00000539-199812000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Kain ZN, Caldwell-Andrews AA. Preoperative psychological preparation of the child for surgery: an update. Anesthesiol Clin North America. 2005;23:597–614. doi: 10.1016/j.atc.2005.07.003. [DOI] [PubMed] [Google Scholar]
- 6.Wright KD, Stewart SH, Finley GA, Buffett-Jerrott SE. Prevention and Intervention Strategies to Alleviate Preoperative Anxiety in Children: A Critical Review. Behav Modif. 2007;31:52–79. doi: 10.1177/0145445506295055. [DOI] [PubMed] [Google Scholar]
- 7.Eysenck MW, Derakshan N, Santos R, Calvo MG. Anxiety and cognitive performance: attentional control theory. Emotion. 2007;7:336–53. doi: 10.1037/1528-3542.7.2.336. [DOI] [PubMed] [Google Scholar]
- 8.Kain ZN, MacLaren JE, Hammell C, Novoa C, Fortier MA, Huszti H, Mayes L. Healthcare provider-child-parent communication in the preoperative surgical setting. Paediatr Anaesth. 2009;19:376–84. doi: 10.1111/j.1460-9592.2008.02921.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rimer BK, Conaway M, Lyna P, Glassman B, Yarnall KS, Lipkus I, Barber LT. The impact of tailored interventions on a community health center population. Patient Educ Couns. 1999;37:125–40. doi: 10.1016/s0738-3991(98)00122-0. [DOI] [PubMed] [Google Scholar]
- 10.Oenema A, Brug J, Lechner L. Web-based tailored nutrition education: results of a randomized controlled trial. Health Educ Res. 2001;16:647–60. doi: 10.1093/her/16.6.647. [DOI] [PubMed] [Google Scholar]
- 11.Brug J, Steenhuis I, Van Assema P, De Vries H. The impact of a computer-tailored nutrition intervention. Prev Med. 1996;25:236–42. doi: 10.1006/pmed.1996.0052. [DOI] [PubMed] [Google Scholar]
- 12.Brug J, Campbell M, van Assema P. The application and impact of computer-generated personalized nutrition education: a review of the literature. Patient Educ Couns. 1999;36:145–56. doi: 10.1016/s0738-3991(98)00131-1. [DOI] [PubMed] [Google Scholar]
- 13.Kreuter MW, Wray RJ. Tailored and targeted health communication: strategies for enhancing information relevance. Am J Health Behav. 2003;27:s227–3. doi: 10.5993/ajhb.27.1.s3.6. [DOI] [PubMed] [Google Scholar]
- 14.Kreuter MW, Skinner CS. Tailoring: what's in a name? Health Educ Res. 2000;15:1–4. doi: 10.1093/her/15.1.1. [DOI] [PubMed] [Google Scholar]
- 15.Dijkstra A, De Vries H. The development of computer-generated tailored interventions. Patient Educ and Couns. 1999;36:193–203. doi: 10.1016/s0738-3991(98)00135-9. [DOI] [PubMed] [Google Scholar]
- 16.Rakowski W, Ehrich B, Goldstein M, Rimer B, Pearlman D, Clark M, Velicer W, Woolverton H. Increasing mammography among women aged 40–74 by use of a stage-matched tailored intervention. Prev Med. 1998;27:748–56. doi: 10.1006/pmed.1998.0354. [DOI] [PubMed] [Google Scholar]
- 17.Brug J, Oenema A, Campbell M. Past, present, and future of computer-tailored nutrition education. Am J Clin Nutr. 2003;77:S1028–S34. doi: 10.1093/ajcn/77.4.1028S. [DOI] [PubMed] [Google Scholar]
- 18.Brug J, Oenema A, Kroeze W, Raat H. The internet and nutrition education: challenges and opportunities. Eur J Clin Nutr. 2005;59:S130–9. doi: 10.1038/sj.ejcn.1602186. [DOI] [PubMed] [Google Scholar]
- 19.Fortier MA, Bunzli E, Walthall J, Olshansky E, Saadat H, Santistevan R, Mayes L, Kain ZN. Web-based Tailored Intervention for Preparation of Parents and Children for Outpatient Surgery (WebTIPS): Formative Evaluation and Randomized Controlled Trial. Anesth Analg. 2015 doi: 10.1213/ANE.0000000000000632. IN THIS ISSUE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pew Internet & American Life Project. [Accessed April 30, 2014];Internet User Demographics. 2014 Available at: http://www.pewinternet.org/data-trend/internet-use/latest-stats/
- 21.De Vries H, Brug J. Computer-tailored interventions motivating people to adopt health promoting behaviours: introduction to a new approach. Patient Educ Couns. 1999;36:99–105. doi: 10.1016/s0738-3991(98)00127-x. [DOI] [PubMed] [Google Scholar]
- 22.Lauver D, Ward S, Heidrich S, Keller ML, Bowers BJ, Brennan PF, Korchhoff TK, Wells TJ. Patient-centered interventions. Res Nurs Health. 2002;25:246–55. doi: 10.1002/nur.10044. [DOI] [PubMed] [Google Scholar]
- 23.Boothroyd RA, Banks SM, Evans ME, Greenbaum PE, Brown E. Untangling the web: an approach to analyzing the impacts of individually tailored, multicomponent treatment interventions. Mental Health Services Research. 2004 Sep;6(3):143–153. doi: 10.1023/b:mhsr.0000036488.12833.6e. [DOI] [PubMed] [Google Scholar]
- 24.Spielberger CD. Manual for the State-Trait Anxiety Inventory (STAI : Form Y) Palo Alto, CA: Consulting Psychologists Press; 1983. pp. 4–26. [Google Scholar]
- 25.Miller S. Monitoring and blunting: Validation of a questionnaire to assess styles of information seeking under threat. J Pers Soc Psychol. 1987;52:345–53. doi: 10.1037//0022-3514.52.2.345. [DOI] [PubMed] [Google Scholar]
- 26.Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, Wadsworth ME. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol Bull. 2001;127:87–127. [PubMed] [Google Scholar]
- 27.Miller SM. Monitoring versus blunting styles of coping with cancer influence the information patients want and need about their disease. Implications for cancer screening and management Cancer. 1995;76:167–77. doi: 10.1002/1097-0142(19950715)76:2<167::aid-cncr2820760203>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 28.Miller SM, Rodoletz M, Mangan CE, Schroeder CM, Sedlacek TV. Applications of the monitoring process model to coping with severe long- term medical threats. Health Psychol. 1996;15:216–25. doi: 10.1037//0278-6133.15.3.216. [DOI] [PubMed] [Google Scholar]
- 29.Williams-Piehota P, Pizarro J, Schneider TR, Mowad L, Salovey P. Matching health messages to monitor-blunter coping styles to motivate screening mammography. Health Psychol. 2005;24:58–67. doi: 10.1037/0278-6133.24.1.58. [DOI] [PubMed] [Google Scholar]
- 30.Forward S, Brown T, McGrath P. Mothers' attitudes and behavior toward medicating children's pain. Pain. 1996;67:469–74. doi: 10.1016/0304-3959(96)03149-1. [DOI] [PubMed] [Google Scholar]
- 31.Yaffa Zisk R, Grey M, MacLaren J, Kain Z. Exploring Socio-Demographic and Personality Characteristic Predictors of Parental Pain Perceptions. Anesth Analg. 2007;106:65–74. doi: 10.1213/01.ane.0000257927.35206.c1. [DOI] [PubMed] [Google Scholar]
- 32.Zisk Rony RY, Fortier MA, Chorney JM, Perret D, Kain ZN. Parental postoperative pain management: attitudes, assessment, and management. Pediatrics. 2010;125:e1372–8. doi: 10.1542/peds.2009-2632. [DOI] [PubMed] [Google Scholar]
- 33.Zisk RY, Grey M, Medoff-Cooper B, MacLaren JE, Kain ZN. The squeaky wheel gets the grease: parental pain management of children treated for bone fractures. Pediatr Emerg Care. 2008;24:89–96. doi: 10.1097/PEC.0b013e318163db77. [DOI] [PubMed] [Google Scholar]
- 34.Kain ZN, Caldwell-Andrews AA, Krivutza D, Weinberg ME, Wang SM, Gaal D. Trends in the practice of parental presence during induction of anesthesia and the use of preoperative sedative premedication in the United States, 1995-2002: Results of a follow-up national survey. Anesth Analg. 2004;98:1252–9. doi: 10.1213/01.ane.0000111183.38618.d8. [DOI] [PubMed] [Google Scholar]
- 35.Putnam SP, Rothbart MK, Putnam SP, Rothbart MK. Development of short and very short forms of the Children's Behavior Questionnaire. J Pers Assess. 2006;87:102–12. doi: 10.1207/s15327752jpa8701_09. [DOI] [PubMed] [Google Scholar]
- 36.Fortier MA, Blount RL, Wang SM, Mayes LC, Kain ZN. Analysing a family-centred preoperative intervention programme: a dismantling approach. Br J Anaesth. 2011;106:713–8. doi: 10.1093/bja/aer010. [DOI] [PMC free article] [PubMed] [Google Scholar]