

Abstract
Moyamoya disease can be associated with autoimmune disease such as thyrotoxicosis, but there has been only one report of association with neuromyelitis optica (NMO). We report another case of this combination with the presence of anti-SSA antibody in addition to the NMO-immunoglobulin G. The patient presented limb weakness along with unsteady gait and numbness. A magnetic resonance imaging (MRI) of the spine showed extensive intramedullary hyperintense signals at C2 to T3 levels. On the other hand, no lesions were found on the MRI of the brain. The patient tested positive for anti-aquaporin-4 antibody and anti-SSA antibody which confirms the diagnosis of NMO. A magnetic resonance angiography scan of the brain revealed a bilateral distal occlusion of the internal carotid arteries (ICAs) as well as occlusions of the middle cerebral arteries (MCAs) with fine collaterals in the region which confirms the diagnosis of moyamoya disease. This report suggests that autoimmunity may be an important factor in the pathogenesis of moyamoya disease in some patients.
INTRODUCTION
Moyamoya disease is a cerebrovascular disease that increases risk of stroke in affected patients, and it is particularly common in East Asia. This disease is caused by severe stenosis on the internal carotid arteries and their proximal branches. As a compensatory mechanism to the reduced blood flow, small collateral vessels are formed, but these vessels are weak and prone to hemorrhage, aneurysm and thrombosis. This network of collateral vessels have an appearance of a ‘puff of smoke’, which translates to moyamoya in Japanese. The collateral vessels are thus known as ‘moyamoya vessels’ [1]. The exact etiology of the disease remains uncertain, but there have been suggestions that in some cases, moyamoya disease may be associated with autoimmune diseases [2].
Neuromyelitis optica (NMO) is an autoimmune, inflammatory disorder in which the optic nerves and spinal cord are damaged by inflammation. The disease is often presented as weakness in the limbs of varying degrees or loss in vision in one or both eyes. The diagnosis of NMO is usually confirmed with the presence of anti-aquaporin-4 antibody also known as NMO-immunoglobulin G [3].
Because of the known association of moyamoya disease with autoimmune disease, it may be possible to encounter patients who were affected by both illnesses. However, the report of patients with both diseases is rare. We describe here a patient who suffers from both moyamoya disease and NMO simultaneously, suggesting that there may be a relationship between the two diseases in the form of autoimmunity.
CASE REPORT
A 62-year-old woman with good past health with no previous neurological symptom was admitted to the Prince of Wales Hospital in Hong Kong after a sudden onset of left upper limb and lower limb weakness along with unsteady gait and numbness. Examination upon admission revealed brisk reflexes over both lower limbs, reduced pinprick sensation with a sensory level at T3 over left side. Her blood pressure was 141/74 mmHg with no history of smoking, hypertension, diabetes or dyslipidemia. An MRI scan of the whole spine showed extensive intramedullary hyperintense signals at C2 to T3 levels; most discrete at the T2 level. On the other hand, no lesions were found on the MRI of the brain. The severity of the spinal lesions and lack of brain lesions prompted an immunological investigation. The patient tested positive for anti-aquaporin-4 antibody and anti-SSA antibody using immunofluorescent test which confirms the diagnosis of NMO. In addition, her rheumatoid factor and antinuclear antibody were both negative; and there were no clinical features of keratoconjunctivitis sicca or dry month suggestive of Sjogren's syndrome.
A magnetic resonance angiography (MRA) scan of the brain revealed a bilateral distal occlusion of the internal carotid arteries. Occlusions of the MCA were noted with fine collaterals in the region—reminiscent of moyamoya vessels. The ICAs and ACA were preserved; and the CCAs were normal without atherosclerotic changes. She was diagnosed with moyamoya disease as well (Fig. 1).
Figure 1:
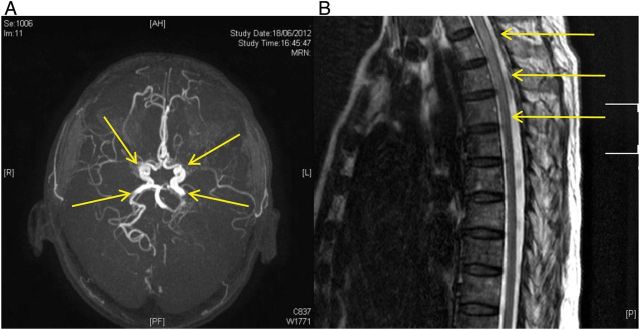
(A) An MRA of the head revealing occlusions of bilateral distal ICAs and presence of moyamoya vessels. (B) Axial MRI image of the spine showing intramedullary T2-hyperintense signals.
Despite treatment, leg weakness showed no significant improvement and further deterioration of leg power was witnessed with the left leg deteriorating more than the right. Intravenous methylprednisolone 1 g daily was given for 3 days. Afterwards, she was transferred to rehabilitation after 19 days in hospital with oral prescription of 30 mg of prednisolone daily together with azathioprine 50 mg daily. On follow-up 1 month later, she had suboptimal recovery with lower limb power remained Medical Research Council (MRC) Grade 3+/5 with spasticity and walk with frame for short distance. Blood test also revealed elevated alanine aminotransferase (ALT) 161 U/L while on azathioprine 50 mg daily. Therefore, azathioprine was stopped. Then, she received six courses of monthly cyclophosphamide (750 mg every month). She had gradual improvement in her neurological status with lower limb power MRC Grade 5/5 with reduced spasticity and able to walk with stick. Interval MRI brain and whole spine with contrast showed resolution of spine lesion and one new small non-contrast enhancing lesion over right cerebral peduncle. Clinically she remained well and she was re-challenged with low-dose azathioprine 25 mg daily since September 2013. Prednisolone was currently kept at a low dose 10 mg daily and planned to further taper down if she could tolerate higher dose of azathioprine.
DISCUSSION
Neuromyelitis optica is an autoimmune, inflammatory disease with strong associations with certain immunologic factors such as anti-aquaporin-4 antibody, anti-SSA and anti-SSB antibodies. Among these immunologic factors, anti-SSA can be considered a relatively rare one; occurring in only 15.7% of patients with NMO [4].
As far as we know, there has only been one previous report of a patient with NMO and concurrent moyamoya disease. The previous report detailed a similar profile with both patients being female and of East Asian descent. Most notably though is that both patients share a positive response for anti-SSA antibody and anti-aquaporin-4 antibody [5]. This suggests that there may be a connection between the two diseases and these autoimmune antibodies. However, our patient did not fulfill the diagnostic criteria for Sjogern's syndrome [6], which is in contrast with the previous reported case. Anti-aquaporin-4 antibody mainly affects the cell membrane so is unlikely to be connected to moyamoya disease [3]. Hence, our patient, together with previous case report [5], suggested that moyamoya disease may be associated with anti-SSA antibody. Considering the low percentage of patients with NMO and anti-SSA antibody, the presence of anti-SSA antibodies for both patients can suggest that it may be more than a coincidence. If there indeed is a connection between moyamoya disease and anti-SSA, then the etiology of moyamoya disease may be more suggestive of autoimmune in nature.
After searching through literature, there have been reports of moyamoya disease being associated with other autoimmune diseases such as Sjogern's syndrome [7], Graves' disease [8] and systemic lupus erythematosus [9]. There have also been reports of collateralization resembling moyamoya disease associated with autoimmune antibodies [2]. More recently, a case series of 94 primarily white patients with moyamoya disease was reported and the patients had significantly higher prevalence of autoimmune diseases (22.3%) [10]. However, none of these patients was anti-SSA antibody positive.
However, there is still insufficient data to provide a concrete association between moyamoya disease and autoimmune antibodies. More research will be needed to confirm that moyamoya disease is caused by autoimmunity.
ACKNOWLEDGEMENTS
We thank Chinese University of Hong Kong (Focused Investment Scheme B) and the Institute of Innovative Medicine, Chinese University of Hong Kong.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1.Scott RM, Smith ER. Moyamoya disease and moyamoya syndrome. N Engl J Med. 2009;360:1226–37. doi: 10.1056/NEJMra0804622. [DOI] [PubMed] [Google Scholar]
- 2.Provost TT, Moses H, Morris EL, Altman J, Harley JB, Alexander E, et al. Cerebral vasculopathy associated with collaterization resembling moyamoya phenomenon and with anti-Ro/SSA and anti-LA/SSB antibodies. Arthritis Rheum. 1991;34:1052–5. doi: 10.1002/art.1780340816. [DOI] [PubMed] [Google Scholar]
- 3.Downer JJ, Leite MI, Carter R, Palace J, Kuker W, Quaghebeur G. Diagnosis of neruomyelitis optica (NMO) spectrum disorders: is MRI obsolete? Neuroradiology. 2012;54:279–85. doi: 10.1007/s00234-011-0875-x. [DOI] [PubMed] [Google Scholar]
- 4.Pittock SJ, Lennon VA, de Seze J, Vermersch P, Homburger HA, Wingerchuk DM, et al. Neuromyelitis optica and non-organ-specific autoimmunity. Arch Neurol. 2008;65:78–83. doi: 10.1001/archneurol.2007.17. [DOI] [PubMed] [Google Scholar]
- 5.Asai Y, Nakayasu H, Fusayasu E, Nakashima K. Moyamoya disease presenting as thalamic hemorrhage in a patient with neuromyelitis optica and Sjogren's syndrome. J Stroke Cerebrovasc Dis. 2012;21:619.e7–9. doi: 10.1016/j.jstrokecerebrovasdis.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 6.Goldblatt F, O'Neill SG. Clinical aspects of autoimmue rheumatic disease. Lancet. 2013;382:797–808. doi: 10.1016/S0140-6736(13)61499-3. [DOI] [PubMed] [Google Scholar]
- 7.Matsuki Y, Kawakami M, Ishizuka T, Kawaguchi Y, Hidaka T, Suzuki K, et al. SLE and Sjögren's syndrome associated with unilateral moyamoya vessels in cerebral arteries. Scand J Rheumatol. 1997;26:392–4. doi: 10.3109/03009749709065707. [DOI] [PubMed] [Google Scholar]
- 8.Malik S, Russman AN, Katramados AM, Silver B, Mitsias PD. Moyamoya syndrome associated with Graves’ disease: a case report and review of the literature. J Stroke Cerebrovasc Dis. 2011;20:528–36. doi: 10.1016/j.jstrokecerebrovasdis.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 9.Jeong HC, Kim YJ, Yoon W, Joo SP, Lee SS, Park YW. Moyamoya Syndrome associated with systemic lupus erythematosus. Lupus. 2008;17:679–82. doi: 10.1177/0961203307087375. [DOI] [PubMed] [Google Scholar]
- 10.Bower RS, Mallory GW, Nwojo M, Kudva YC, Flemming KD, Meyer FB. Moyamoya disease in a primarily white, Midwestern US population. Stroke. 2013;44:1997–9. doi: 10.1161/STROKEAHA.111.000307. [DOI] [PubMed] [Google Scholar]