

Abstract
The purpose of this study was to report variations of the cubital superficial vein patterns in the Korean subjects, which was investigated by using venous illuminator, AccuVein. The 200 Korean subjects were randomly chosen from the patients and staff of the Keimyung University Dongsan Medical Center in Daegu, Korea. After excluding the inappropriate cases for detecting venous pattern, we collected 174 cases of right upper limbs and 179 cases of left upper limbs. The superficial veins of the cubital fossa were detected and classified into four types according to the presence of the median cubital vein (MCV) or median antebrachial vein. The type II, presenting the both cephalic and basilic vein connected by the MCV, was most common (177 upper limbs, 50.1%). Although the most common type in male and female was different as type I (108 upper limbs, 49.3%) and type II (75 upper limbs, 56.0%), respectively, statistical significance was not detected (P=0.241). The frequency of the each types between right and left upper limbs was also not different (P=0.973). Among 154 subjects who were observed the venous pattern in the both upper limbs, 76 subjects (49.3%) had the same venous pattern. Using AccuVein to investigate the venous pattern has an advantage of lager scale examination compared to the cadaver study. Our results might be helpful for medical practitioner to be aware of the variation of the superficial cubital superficial vein.
Keywords: Cubital fossa, Vein illuminator, Anatomical variation, Cephalic vein, Basilic vein
Introduction
Venipuncture for obtaining a blood sample is one of the most common procedures in the emergency room. It is performed by various medical practitioners such as physician, nurse, emergency medical technician. For inexperienced health workers, it can be the most frustrating and most important task for building rapport with patients. Despite of the importance of the approaching superficial veins, however, students in the health care system usually have rare opportunities to observe actual human superficial vein, including anatomy cadavers. Furthermore, application of educated anatomical knowledge to the practical venipuncture procedure is difficult work because of variation of the anatomy of superficial vein [1, 2].
The one of most common site for venipuncture is the superficial veins in the cubital fossa of upper limbs which include the cephalic, basilic, median cubital, and antebrachial veins and their tributaries. Because of the wide variations of these superficial veins, it has been reported that adverse effects such as bruising, hematoma, and sensory change occurred by mispuncture in various health care system [3, 4]. For the accomplishment of venipuncture of these superficial veins without such accidents, it is important to understand the courses of the superficial veins.
Although there are numerous variations of the superficial venous system in the cubital fossa, it was classified into several types by investigators. Most of them classified the courses of the superficial veins into four or six types [5, 6, 7, 8, 9]. However, none of these have conducted large scale examinations using any specific equipment in alive human.
Recently, several devices using infrared reflection were developed to optimize peripheral venipuncture [10, 11]. It was reported that the first-attempt success rate was higher in the using device group than the control group [12]. Among those devices, one of the commercially available devices is the AccuVein AV300 (AccuVein LLC, Cold Spring Harbor, NY, USA). Here, we examined the different type courses of superficial veins in the cubital fossa in a large scale Korean population performed by AccuVein AV300 device (AV300).
Materials and Methods
In this study 120 males and 80 females were randomly selected from among the patients and staff of the Keimyung University Dongsan Medical Center in Daegu, Korea. All subjects were Koreans aged between 21 and 87 years (mean, 52.6 years). Excluded were those with thick subcutaneous tissue layers which was not observed by AV300 or wound within the cubital region. As a result, we collected 174 cases of right upper limbs and 179 cases of left upper limbs. After taking the subject's consent, the superficial veins of the cubital fossa were made prominent by using AV300 about 10 cm proximal to crease at the elbow and by active movements of the forearm. The veins were marked on the skin and the pattern of veins in each case was accurately drawn on a sheet of paper which was identified with the name, sex and age of the subject; venous patterns on the right and left sides were noted separately. Small veins were ignored. All the drawings obtained were carefully studied and analyzed.
Types of superficial venous arrangement
The cubital veins are classified into four main groups based on previous study [8] with following criteria (Fig. 1).
Fig. 1. Running patterns of superficial veins in right cubital fossa. The patterns were classified into four types (See Materials and Methods). CV, cephalic vein; BV, basilic vein; MCV, median cubital vein; MABV, median antebrachial vein.
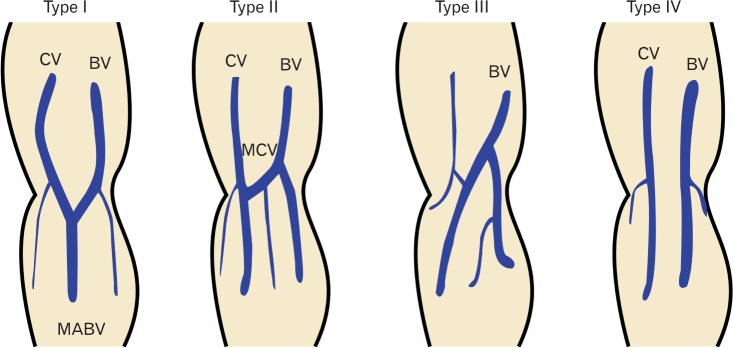
Type I: The median antebrachial vein was dominant and joined both cephalic vein (CV) and basilic vein (BV) in the cubital region.
Type II: In the cubital region, the median cubital vein connected the two veins in the cubital region.
Type III: In the cubital region, development of the brachial CV was poor or missing.
Type IV: No communicating branch between the CV and BV.
Statistical analysis
Statistical analysis was done using the SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). For comparisons, chi-square Fisher exact test was used to determine significance at P<0.05.
Results
We visualized the morphology of the superficial vein in the cubital region using AV300 (Fig. 2), and classified them into four types (See Materials and Methods). In agreement with previous study [8], type II was the most common type (177 upper limbs, 50.1%) (Table 1), while type I, III, and IV was found in 165 (46.7%), 7 (2.0%), and 4 upper limbs (1.1%), respectively. Comparison in sexual difference, the most common type in male and female was different as type I (108 upper limbs, 49.3%) and type II (75 upper limbs, 56.0%), respectively. However, different frequency of the type of a superficial vein between men and women was not significant (P=0.241, Fisher exact test). Furthermore, frequency of the type between right and left upper limbs was not different (P=0.973, Fisher exact test) (Table 2).
Fig. 2. Image of veins captured and projected on the skin of cubital region by AV300.
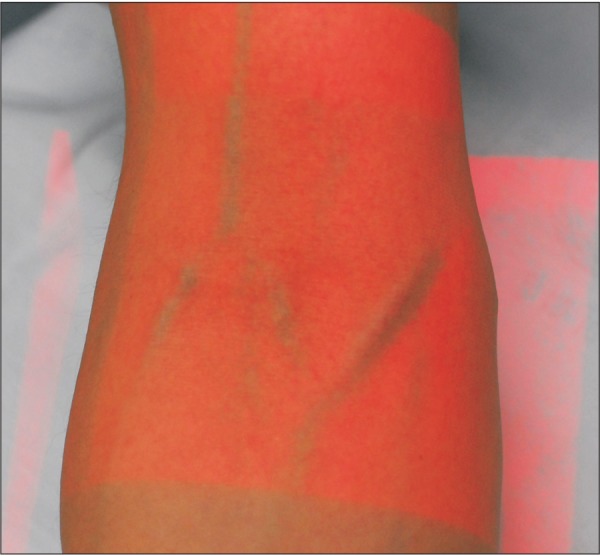
Table 1. Number and frequency of the type of the superficial vein in the cubital region of both gender.
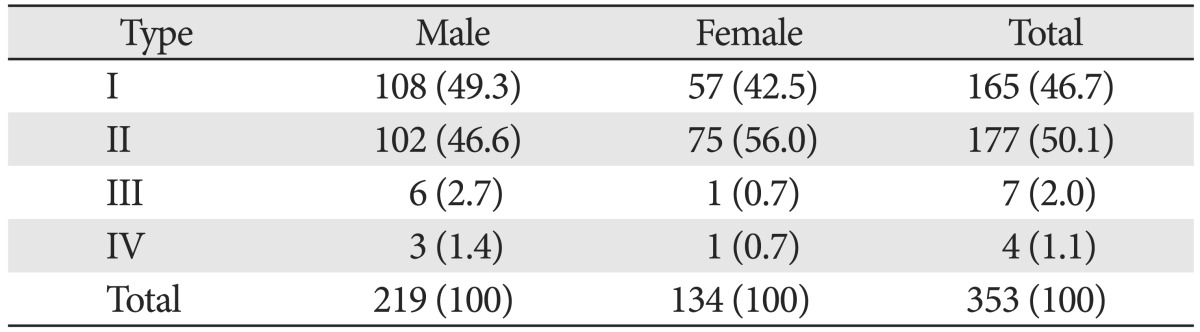
Values are presented as number (%).
Table 2. Number and frequency of the type of the superficial vein in the cubital region of both upper limbs.
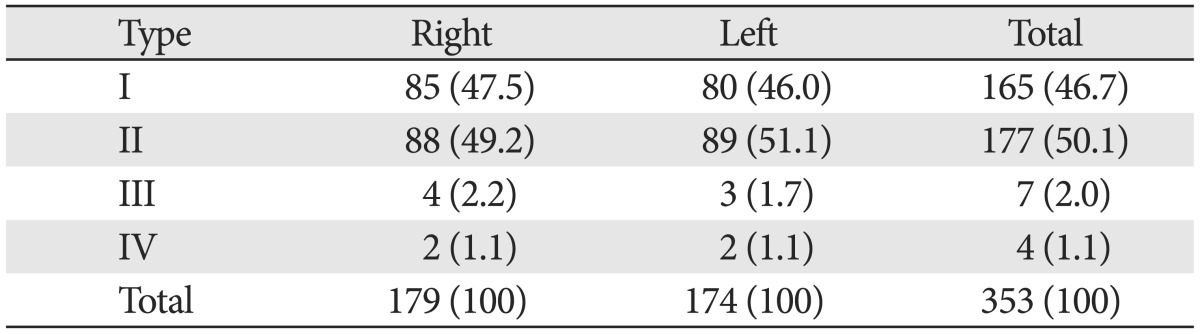
Values are presented as number (%).
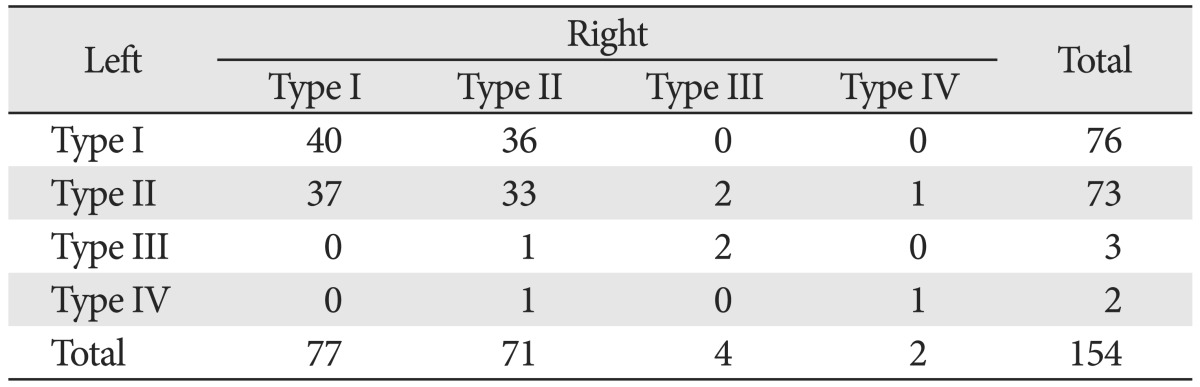
We were able to distinct the venous pattern in the both sides of 154 subjects among examined 200 subjects. Seventy six subjects (49.3%) had the same venous pattern in both upper limbs. The association of the type frequency between right and left upper limbs seems to be significant (P<0.001, Fisher exact test) (Table 3), which means laterality of the superficial vein type.
Table 3. The contingency table of the type of the superficial vein in the cubital region between both upper limbs.
Discussion
The results from this study show that gender influence was not significant on the venous pattern of the cubital region of the upper limbs. The right and left side difference in both sexes was also not significant. The frequency of the venous pattern was comparable to the previous cadaver study in Asian [8] in which the frequencies of types I, II, III, and IV described as 41.7%, 56.7%, 1.7%, and 0%, respectively.
Most medical practitioners are aware of two patterns of venous returns in the cubital fossa. Standard textbooks of anatomy state that the median cubital vein passes diagonally across the roof of the cubital fossa and connects the CV on the lateral side with the basilic vein on the medial side [2]. So called N-type or type II in our study was the most common pattern which was present 56.0% of females and 46.6% of males. Another textbook states that a single median antebrachial vein divides into median cephalic and basilic veins which drain into the cephalic and basilic veins respectively. We found this pattern, so called M-type or type I in 42.5% of females and in 49.3% of males.
Absence of the median cubital vein or communicating branch between the cephalic and basilic veins, type IV, was found in 1 upper limb in females and in 3 upper limbs in males. The type III, poor development of CV, was found in 1 upper limb of females and in 6 upper limbs of males. Although these two rare types of cubital vein pattern were found higher in males than in females, statistical significance of gender influence was not found. The association of these two patterns between right and left upper limbs was seemed to be significant. Cause of the low frequency of the venous patterns III and IV, however, it was not able to statistically interpret the results. Therefore, it needs to conduct further study including more subjects about gender influence or left-right symmetry of these two rare venous patterns in the cubital region.
Comparing with the cadaver dissection, our study has some limitations of missing the small vessels and being not able to examine the topological correlation with the cutaneous nerve in the cubital region. It also needs to conduct the cadaver dissection within the cubital region finding the topological pattern of the venous patterns and the cutaneous nerve. Nevertheless, our study has an advantage of larger scale examination compared to the cadaver study. Considering with the high success rate of venipuncture using intravenous illuminator [12], our study has an advantage of more accuracy in classifying the venous pattern compared to the vein engorgement study using tourniquet.
Acknowledgements
We thank all our colleagues in Keimyung University School of Medicine for helpful advice and discussions.
References
- 1.Moore KL, Dalley AF, Agur AM. Clinically oriented anatomy. Philadelphia: Lippincott Williams & Wilkins; 2013. [Google Scholar]
- 2.Warwick R, Williams PL. Gray's anatomy. Edinburgh: Longman; 1973. [Google Scholar]
- 3.Newman BH, Pichette S, Pichette D, Dzaka E. Adverse effects in blood donors after whole-blood donation: a study of 1000 blood donors interviewed 3 weeks after whole-blood donation. Transfusion. 2003;43:598–603. doi: 10.1046/j.1537-2995.2003.00368.x. [DOI] [PubMed] [Google Scholar]
- 4.Newman BH, Waxman DA. Blood donation-related neurologic needle injury: evaluation of 2 years' worth of data from a large blood center. Transfusion. 1996;36:213–215. doi: 10.1046/j.1537-2995.1996.36396182137.x. [DOI] [PubMed] [Google Scholar]
- 5.Dharap AS, Shaharuddin MY. Patterns of superficial veins of the cubital fossa in Malays. Med J Malaysia. 1994;49:239–241. [PubMed] [Google Scholar]
- 6.Mikuni Y, Chiba S, Tonosaki Y. Topographical anatomy of superficial veins, cutaneous nerves, and arteries at venipuncture sites in the cubital fossa. Anat Sci Int. 2013;88:46–57. doi: 10.1007/s12565-012-0160-z. [DOI] [PubMed] [Google Scholar]
- 7.Ukoha UU, Oranusi CK, Okafor JI, Ogugua PC, Obiaduo AO. Patterns of superficial venous arrangement in the cubital fossa of adult Nigerians. Niger J Clin Pract. 2013;16:104–109. doi: 10.4103/1119-3077.106777. [DOI] [PubMed] [Google Scholar]
- 8.Yamada K, Yamada K, Katsuda I, Hida T. Cubital fossa venipuncture sites based on anatomical variations and relationships of cutaneous veins and nerves. Clin Anat. 2008;21:307–313. doi: 10.1002/ca.20622. [DOI] [PubMed] [Google Scholar]
- 9.Wasfi FA, Dabbagh AW, AlAthari FM, Salman SS. Biostatistical study on the arrangement of the superficial veins of the cubital fossa in Iraqis. Acta Anat (Basel) 1986;126:183–186. doi: 10.1159/000146212. [DOI] [PubMed] [Google Scholar]
- 10.Hess HA. A biomedical device to improve pediatric vascular access success. Pediatr Nurs. 2010;36:259–263. [PubMed] [Google Scholar]
- 11.Kaddoum RN, Anghelescu DL, Parish ME, Wright BB, Trujillo L, Wu J, Wu Y, Burgoyne LL. A randomized controlled trial comparing the AccuVein AV300 device to standard insertion technique for intravenous cannulation of anesthetized children. Paediatr Anaesth. 2012;22:884–889. doi: 10.1111/j.1460-9592.2012.03896.x. [DOI] [PubMed] [Google Scholar]
- 12.Kim MJ, Park JM, Rhee N, Je SM, Hong SH, Lee YM, Chung SP, Kim SH. Efficacy of VeinViewer in pediatric peripheral intravenous access: a randomized controlled trial. Eur J Pediatr. 2012;171:1121–1125. doi: 10.1007/s00431-012-1713-9. [DOI] [PubMed] [Google Scholar]