

Abstract
The skin punch or surgical punch is an instrument which is used almost exclusively by dermatologists. It is a circular hollow blade attached to a pencil-like handle ranging in size from 0.5 to 10 mm. It is available as a disposable, reusable, and automated instrument. The punch can be used as a diagnostic, therapeutic, and cosmetic tool in dermatology. We have used punch as a diagnostic, therapeutic, and cosmetic tool in our dermatosurgery practice in our hospital. Various original research articles, text book publications, and review articles were studied and compiled. Techniques used by various authors and our own experiences with punch have been described. This article aims at providing the novel usefulness of skin biopsy punch in dermatology as the basic punch surgery is quick and easy to learn. Complications such as bleeding and infection are minimal.
Keywords: Biopsy, nail biopsy, punch excision, skin biopsy
What was known?
Punch instrument is a circular hollow blade attached to a pencil-like handle ranging in size from 0.5 mm to 10 mm available as a disposable, reusable, and automated instrument. Punch biopsy is an apparently simple procedure include the relative easiness to perform, minimal complications, and provision of a full-thickness sample.
Introduction
The skin punch is an instrument which is used almost exclusively by dermatologists. It was EL Keyes in 1887, who first established the importance of punch instrument in dermatology.[1] The skin biopsy is a relatively simple, but essential procedure in the management of skin disorders. Properly performed, it may confirm a diagnosis, remove cosmetically unacceptable lesions, and provide definitive treatment for a number of skin conditions. Techniques used by various authors and our own experiences with punch have been described below.
There are two types of punch instruments
Hand held punches
Power punches
Hand held punches
Variants
Metallic punches with tapering or cylindrical tip; metallic handle with attachable tips; disposable, plastic handle punches; available in sizes from 0.5 to 10 mm in diameter.
The Keye's punch has rounded sharp cutting end and thick handle which make it very much appropriate for small skin biopsies. Because of the thick walls with angled sides above the cutting edge, tissue tends to be pushed away as the punch is made, causing less dermis to be cut through than overlying epidermis. To overcome this disadvantage, loo trephine which has thin walls and newer disposable punches have been developed.[2]
Power punches
Here the shaft of the punch is mounted onto a hand machine with adjustable rotational speed varying from 2000 to 10,000 rpm. It is available in various sizes of 0.5-1.3 mm.
Uses of punches can be classified into three categories: [Table 1]
Table 1.
Different uses of skin biopsy punches in dermatology
Diagnostic purposes.
Therapeutic purposes.
Cosmetic purposes.
Diagnostic uses
Skin biopsy for diagnosis of dermatological diseases
Punch biopsies are simple to perform, have few complications, and if small, can heal without suturing. For non-facial lesions, a 4-mm punch is sufficient; however, in granulomatous conditions or conditions with atypical features, biopsies of 5 mm or more are preferable.
Modified diagnostic punch surgery
Split-punch biopsy technique
This technique is used to obtain two tissue samples for different studies from one punch biopsy. It is done by advancing the punch just into the papillary dermis followed by using a no. 11 blade held nearly perpendicular to the skin surface; the specimen is bisected to the subcutis. Then the punch is reintroduced and advanced to the subcutis and thus the bisected tissue split is obtained.[3]
Double-trephine punch biopsy
This technique is used to obtain tissue samples for diagnosis of dermatoses that affect the subcutaneous tissue. A 6 to 8 mm punch is inserted to obtain the initial sample. Once the superficial core is removed, a 4 mm punch is subsequently used within the center of the 8 mm defect to obtain the subcutaneous tissue.[4]
String-of-beads biopsy technique
This is done by performing smaller, adjacent 4 mm punch biopsies in a row, and the individual biopsy defects may be closed in a linear or multiple O-to-Z/W design with nonabsorbable sutures placed using the simple interrupted suture technique. This method obviates the need for dissection of tissue in pieces.[5]
The pendulum or scoop biopsy
The potential disadvantage of shaving a flat lesion or plaque is the inability to achieve a sufficiently deep or representative sample. The scoop ensures that adequate tissue sampling is achieved, thus making a histopathologic diagnosis readily available. The scoop also results in a smooth biopsy edge which results in less trauma and more rapid healing without scar. The scoop has the additional benefit of providing enough depth so as to make prognostication more accurate in cases of suspected malignancy. Observing standard surgical techniques, the lesion is cleansed and locally anesthetized. Counter traction is applied with the nondominant hand, and the biopsy-pen is inserted into the skin in a pendulous manner. The punch tool scoops the skin like a pendulum. Once the tissue is removed, the subcutaneous tissue is visualized and a procoagulant, such as Monsel's solution or Drysol may be applied for hemostasis.[6]
-
2.
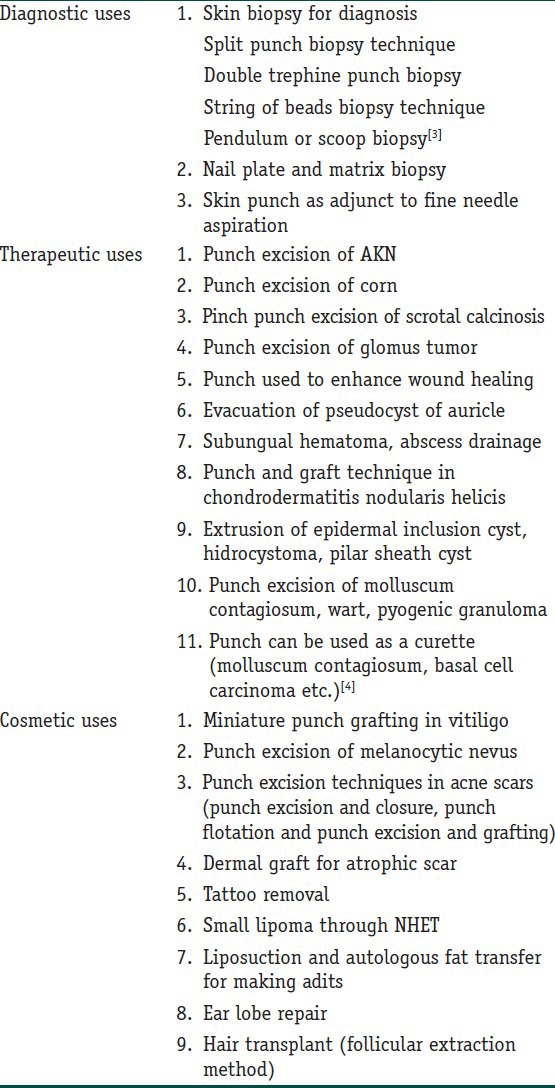
Nail biopsy: 2 to 3 mm punch biopsy is adequate for nail plate, nail bed, and nail matrix in most instances [Figure 1]. For a biopsy of the nail bed, a two-punch method may be used. In this technique, a larger size punch is used to remove the overlying nail plate and then a smaller punch is used to sample the bed.[7]
-
3.
Skin punch as an adjunct to fine-needle aspiration (FNA): Use of the punch is helpful in diagnosing solid organ tumors that are close to the skin surface, such as lymph nodes, the breast, and the thyroid, especially if the FNA yielded a non-diagnostic result.[8]
Figure 1.
Nail matrix biopsy by using punch
Therapeutic uses
Punch excision of acne keloidalis nuchae: The punch should extend deep into the subcutaneous tissue so that the entire hair follicle is excised [Figure 2]. After excision is performed, the wound edges can be injected with 10-40 mg/mL of triamcinolone acetonide to reduce inflammation. Silk sutures may be used to re-approximate the skin.[9]
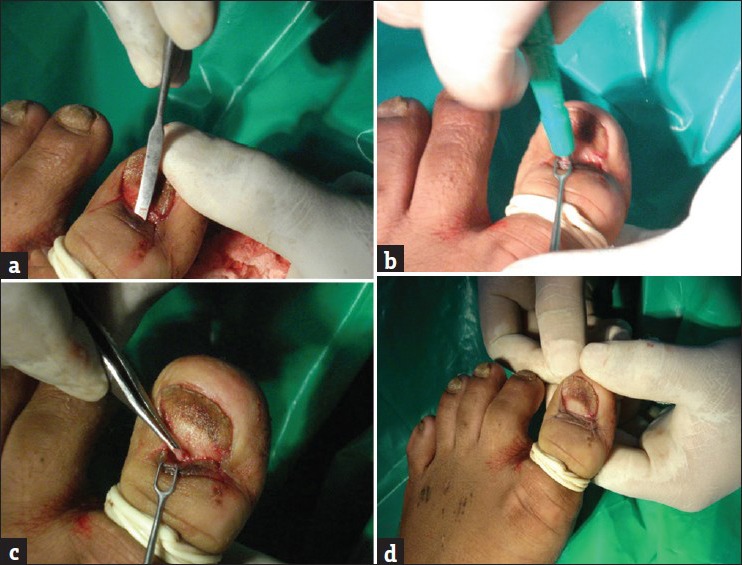
Punch excision of corn: The hyperkeratotic tissue surrounding and over the corn area is pared using no. 20-24 sterile surgical blade which makes the central core or kernel clearly visible. According to the size of the kernel punch with slow gradual rotatory half circular motion is pushed into the tissue. The punched out tissue is gradually pulled without cutting and pressure bandage is applied[10] [Figure 3].
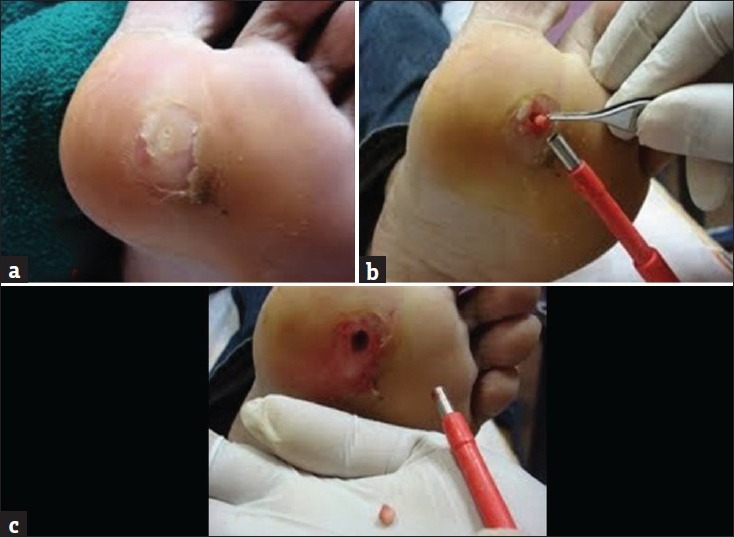
Pinch punch excision of scrotal calcinosis: Scrotal skin is pinched to highlight the subcutaneous nodules and using appropriate size of punch, nodules/cysts are excised[11] [Figure 4].
Punch excision of glomus tumor of nail: A window is created in nail plate by using 5-6 mm punch and tumor in nail bed is excised by taking a smaller punch incision (3-4 mm) and sutured.[12]
Use of the punch to enhance wound healing: The full thickness punch grafts (3 mm punch) are harvested from the buttocks or thigh. Punch holes (2 or 2.5 mm) are made in the floor of the granulating ulcer 5 mm from each other, and grafts are pushed into these recipient holes.[13]
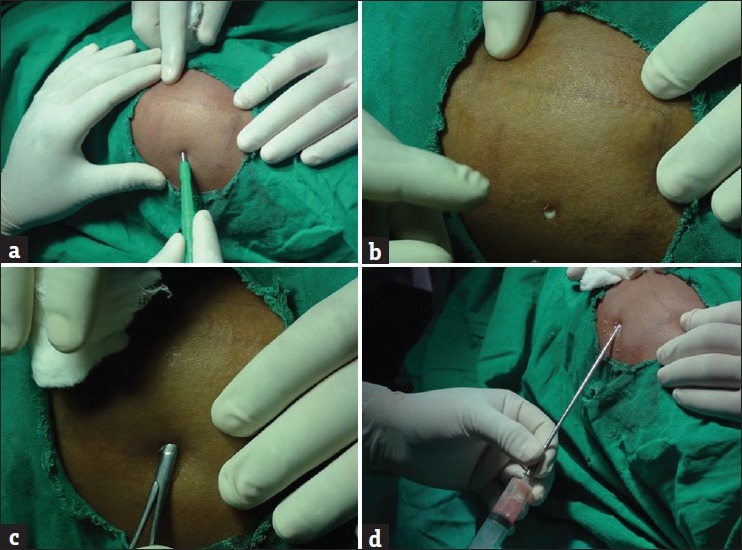
Punch can be used for extrusion of epidermal inclusion cyst, hidrocystomas, pilar sheath cyst, and pseudocyst of auricle[14] with a punch hole technique and the contents of cyst are drained and pressure bandage is applied [Figure 5].
The punch and graft technique in chondrodermatitis nodularis helicis: A punch biopsy is applied perpendicular to the skin surface and advanced until a deep punch of underlying cartilage is cut. Then the same-sized punch of a full-thickness skin graft from the postauricular area donor site is harvested and fixed in place with 6-0 interrupted sutures.[15]
Subungal haematoma[16]: Hematoma is drained by making an opening through the nail plate with either No. 11 blade, electrocautery or punch of size 1.5 or 2 mm or larger (up to 4 mm). Punch is preferred as it remains patent after decompression and allows further drainage without the opening getting sealed.
Punch is used to remove molluscum contagiosum, wart, pyogenic granulomas, etc.
Punch can be held like a pencil or a pen which can mimic the cutting angle of a standard curette. With alternating flexion and extension of the wrist one can use the punch as a curette when curette is not available.[17]
Figure 2.

Punch excision of acne keloidalis nuchae
Figure 3.
Punch excision of corn
Figure 4.
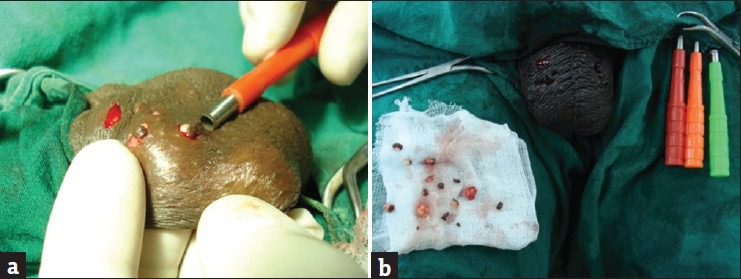
Punch excision of scrotal calcinosis
Figure 5.

Epidermal inclusion cyst extrusion
Cosmetic uses
Miniature punch grafting in vitiligo: This method consists of taking miniature punch grafts of sizes varying from 1 to 3 mm in diameter from donor site, grafting them in appropriate punched out areas spaced 2 to 5 mm apart at the recipient site and further securing them by firm pressure [Figure 6].
Punch excision of melanocytic nevus: Round excision may be a better alternative to conventional fusiform or shave excision of benign papular or dome-shape nevus (<5 mm) of the face because it leaves an almost imperceptible scar[18] [Figure 7].
-
Punch excision techniques in acne scars:[19]
- Punch excision and closure: If the scar is >3.5 mm in size, it is excised and sutured after undermining.
- Punch incision and elevation: If the depressed scar has a normal surface texture, it is incised up to the subcutaneous tissue and elevated to the level of the surrounding skin [Figure 8].
- Punch excision and grafting: Depressed pitted ice pick scars up to 4 mm in diameter are excised and replaced with an autologous, full-thickness punch graft.
Dermal graft for atrophic scar: 3-5 mm punch biopsy up to deep dermis is done in covered parts of the body. The epidermis part is excised and only dermal part is preserved. Subcision of the scar is done 1 week prior to the dermal graft. Depending on the size of the atrophic scar, appropriate size of dermal graft is inserted to the atrophic scar after making the pockets below the scar with 18-G needle [Figure 9]. Seal the entry point with Steri-strip.
Tattoo removal: Very tiny tattoos, in particular remnant of post traumatic tattoos or first attempts at self-tattooing (traditional green tattoo on forehead), may be removed by a punch biopsy closed by a single suture.[20]
-
Small lipoma excision through narrow hole extrusion technique (NHET): In NHET, a small, circular punch defect is created in the skin and then the lipoma is extruded through the hole by applying lateral pressure. A curved hemostat can be inserted in the defect to separate the lipoma from the surrounding tissue.[21]
‘Pot-lid” technique for aesthetic removal of small lipoma on the face: A 5-mm punch inserted deep into the center of the lesion to create a circular hole. The punched-out piece of skin kept in normal saline. The lipoma is extruded with the help of a hemostat and by squeezing pressure. After achieving hemostasis, two absorbable buried subcutaneous sutures are placed to create support for the graft. The punched-out piece of skin is then positioned to cover the defect, like a “lid on a pot” and dressed.[22]
Liposuction: Punch is used to make holes to insert cannulas. A micro-adit used in tumescent liposuction is a small circular hole made by a tiny (1.5 mm or 2 mm) skin biopsy punch facilitate and promote the drainage of residual blood-tinged anesthetic solution associated with tumescent liposuction [Figure 10].
In earlobe repair: Using a punch biopsy instead of the scalpel blade to excise the partial cleft in an elliptical fashion. The opposing margins are sutured together in a straight line.[23]
-
Follicular unit extraction (FUE) method by using micropunches for:
- Androgenitic alopecia
- Eyebrow transplant, eye lash implantation
- Vitiligo surgeries for poliosis etc.
Figure 6.
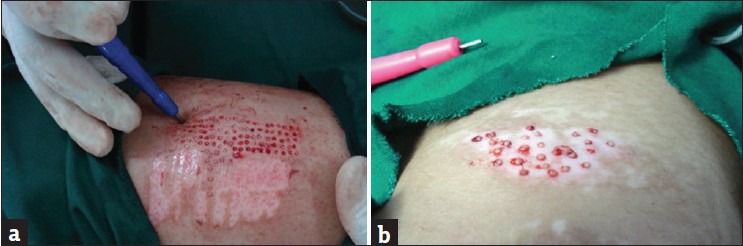
Miniature punch grafting. (a) The donor area and (b) the recipient area
Figure 7.

Melanocytic nevus punch excision and closure
Figure 8.

Punch excision and elevation of acne scar
Figure 9.

(a) Skin biopsy punch of donor area, (b) excision of the dermal graft by scissors, (c) the dermal graft, the epidermis is removed, (d) and (e) showing the subcision of the depressed scar and (f) the photo after dermal graft
Figure 10.
Autologous fat transfer: (A) and (B) the adit made through a punch, (C) the artery forceps inserted into the punch hole to access subcutaneous fat, (D) the extraction of fat
In FUE, the extraction of intact follicular unit is dependent on the principle that the area of attachment of arrector muscle to the follicular unit is the tightest zone. Once this is made loose and separated from the surrounding dermis, the inferior segment can be extracted easily. Because the follicular unit is narrowest at the surface, one needs to use special micropunches of size 0.6-1.0 mm and therefore the resulting scar is too small to be recognized[24] [Figure 11].
Figure 11.
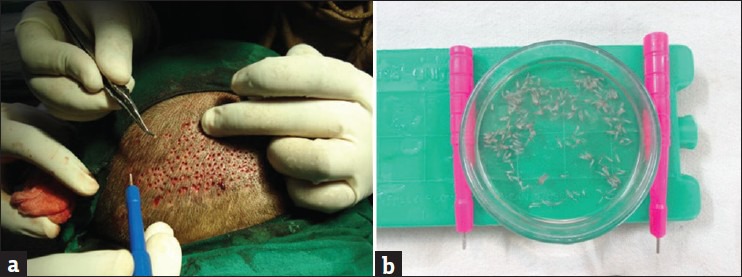
(a) Follicular unit extraction method, (b) the follicular grafts in petridish
Conclusion
Uses of the punch to diagnose and treat many medical and surgical conditions make it important to many other specialties beside dermatology. We propose a punch technique as a novel method for dermatosurgical treatment of various lesions with curative and good cosmetic results when compared with other existing surgical methods.
What is new?
A simple and an inexpensive skin biopsy punch have vast applications in dermatology. It is not only used to confirm a diagnosis, but used to remove cosmetically unacceptable lesions, and provide definitive treatment for a number of skin conditions. The use of skin biopsy punch is not only limited to the field of dermatology but also extended to the other specialties.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Keyes EL. The cutaneous punch. Arch Dermatol. 1982;118:940–2. doi: 10.1001/archderm.118.11.940. [DOI] [PubMed] [Google Scholar]
- 2.Stegman SJ. Commentary: The cutaneous punch. Arch Dermatol. 1982;118:943–4. [PubMed] [Google Scholar]
- 3.Inman VD, Pariser RJ. Biopsy technique pearl: Obtaining an optimal split punch-biopsy specimen. J Am Acad Dermatol. 2003;48:273–4. doi: 10.1067/mjd.2003.42. [DOI] [PubMed] [Google Scholar]
- 4.Nousari HC. Surgical pearl: Double-trephine punch biopsy technique for sampling subcutaneous tissue. J Am Acad Dermatol. 2003;48:609–10. doi: 10.1067/mjd.2003.88. [DOI] [PubMed] [Google Scholar]
- 5.Chavez-Frazier AE, Wanitphakdeedecha R, Nguyen TH, et al. Introducing the string-of-beads biopsy for solving diagnostic challenges of the skin with punch biopsies for multiple studies, simple closure. Dermatol Surg. 2008;34:1549–52. doi: 10.1111/j.1524-4725.2008.34320.x. doi: 10.1111/j. 1524-4725.2008.34320.x. [DOI] [PubMed] [Google Scholar]
- 6.Buka RL, Ness RC. Surgical Pearl: The Pendulum or “Scoop” Biopsy. Clin Med Res. 2008;6:86–7. doi: 10.3121/cmr.2008.804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grover C, Chaturvedi UK, Reddy BS. Role of nail biopsy as a diagnostic tool. Indian J Dermatol Venereol Leprol. 2012;78:290–8. doi: 10.4103/0378-6323.95443. [DOI] [PubMed] [Google Scholar]
- 8.Shin HJ, Sneige N, Staerkel GA. Utility of punch biopsy for lesions that are hard to aspirate by conventional fine-needle aspiration. Cancer. 1999;87:149–54. doi: 10.1002/(sici)1097-0142(19990625)87:3<149::aid-cncr8>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- 9.Dinehart SM, Herzberg AJ, Kerns BJ, Pollack SV. Acne keloidalis: A review. J Dermatol Surg Oncol. 1989;15:642–7. doi: 10.1111/j.1524-4725.1989.tb03603.x. [DOI] [PubMed] [Google Scholar]
- 10.Sacchidanand S, Mallikarjuna M, Purohit V, Sujaya SN. Surgical enucleation of corn: A novel technique. J Cutan Aesthet Surg. 2012;5:52–3. doi: 10.4103/0974-2077.94329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chang CH, Yang CH, Hong HS. Surgical Pearl: Pinch-punch excisions for scrotal calcinosis. J Am Acad Dermatol. 2004;50:780–1. doi: 10.1016/j.jaad.2002.11.001. [DOI] [PubMed] [Google Scholar]
- 12.Savanth SS. Nail surgery. In: Savanth SS, editor. Textbook of dermatosurgery and cosmetology. 2nd ed. Mumbai, India: ASCAD; 2008. p. 250. [Google Scholar]
- 13.Thami GP, Singal A, Bhalla M. Surgical pearl: Full-thickness punch grafting in chronic nonhealing ulcers. J Am Acad Dermatol. 2004;50:99–100. doi: 10.1016/s0190-9622(03)02735-x. [DOI] [PubMed] [Google Scholar]
- 14.Paul AY, Pak HS, Welch ML, Toner CB, Yeager J. Pseudocyst of the auricle: Diagnosis and management with a punch biopsy. J Am Acad Dermatol. 2001;45:230–2. doi: 10.1067/mjd.2001.103991. [DOI] [PubMed] [Google Scholar]
- 15.Rajan N, Langtry JA. The punch and graft technique: A novel method of surgical treatment for chondrodermatitis nodularis helicis. Br J Dermatol. 2007;157:744–7. doi: 10.1111/j.1365-2133.2007.08099.x. [DOI] [PubMed] [Google Scholar]
- 16.Baran R, Haneke E. Skin surgery (Epstein E, Epstein E J reds) 6th edn. Philadelphia: WB Saunders Co; 1987. Surgery of the nail; pp. 534–547. [Google Scholar]
- 17.Quan LT, Orengo I. Surgical Pearl: Curetting with a punch. J Am Acad Dermatol. 2000;43:854–5. doi: 10.1067/mjd.2000.107250. [DOI] [PubMed] [Google Scholar]
- 18.Tursen U, Kaya TI, Ikizoglu G. Surgical approach to benign small papular and dome-shaped melanocytic naevi on the face. J Cosmet Dermatol. 2003;2:175–9. doi: 10.1111/j.1473-2130.2004.00074.x. [DOI] [PubMed] [Google Scholar]
- 19.Khunger N. Scar revision. Dermatologic surgery made easy. In: Sehgal VN, editor. 1st ed. New Delhi, India: Jaypee; 2006. pp. 172–8. [Google Scholar]
- 20.Wollina U, Köstler E. Tattoos: Surgical removal. Clin Dermatol. 2007;25:393–7. doi: 10.1016/j.clindermatol.2007.05.016. [DOI] [PubMed] [Google Scholar]
- 21.Christensen L, Patterson J, Davis D. Surgical pearl: Use of the cutaneous punch for the removal of lipomas. J Am Acad Dermatol. 2000;42:675–6. [PubMed] [Google Scholar]
- 22.Gupta S, Pandhi R, Kumar B. “Pot-lid” technique for aesthetic removal of small lipoma on the face. Int J Dermatol. 2001;40:420–4. doi: 10.1046/j.1365-4362.2001.01225.x. [DOI] [PubMed] [Google Scholar]
- 23.Tan EC. Punch technique--an alternative approach to the repair of pierced earlobe deformities. J Dermatol Surg Oncol. 1989;15:270–2. doi: 10.1111/j.1524-4725.1989.tb03159.x. [DOI] [PubMed] [Google Scholar]
- 24.Dua A, Dua K. Follicular unit extraction hair transplant. J Cutan Aesthet Surg. 2010;3:76–81. doi: 10.4103/0974-2077.69015. [DOI] [PMC free article] [PubMed] [Google Scholar]