

Abstract
Objective
We reviewed the feasibility, safety and efficacy as well as the clinical outcome and long-term angiographic results of endovascular treatment (EVT) of the anterior communicating artery (ACoA) aneurysms.
Methods
A total of 429 ACoA aneurysms in 426 patients were treated using coil embolization between March 1996 and October 2010 in a single institution. Pretreatment aneurysmal features were checked using angiogram. We had usually used tailored steam shaped microcatheter according to individual angiographic architectures. Immediate postembolization outcomes were evaluated using an angiographic outcome scale and clinical evaluation was performed using the Glasgow Outcome Scale (GOS).
Results
Postembolization angiograms demonstrated total occlusion of aneurysm in 290 of 429 (67.6%) aneurysms, neck remnant in 80 (18.6%) and body filling in 59 (13.8%). Dome direction and aneurysm angle was not associated with initial angiographic outcomes. The procedure-related morbidity rate was 0.9% (4 of 429). Clinical and imaging follow-up more than 6 months were available in 382 (89.0%) patients with a mean of 26.2 months. Overall rate of major recanalization was 7.9% (30 of 382) and all of them were retreated without complications. At the last follow-up, 233 (99.2%) of 235 patients had GOS of 5 in unruptured group, and 152 (79.5%) of 191 patients showed good clinical outcomes (GOS of 4 or 5) in ruptured group.
Conclusion
Tailored steam shaping of the microcatheter is vital to achieve good angiographic outcomes regardless of aneurysmal direction. EVT is feasible and safe for most ACoA aneurysms with acceptable immediate and long-term outcomes.
Keywords: Aneurysm, Anterior communicating artery, Endovascular treatment
INTRODUCTION
The anterior communicating artery (ACoA) aneurysm is the most common location of intracranial aneurysms in most series4,16). ACoA aneurysms were traditionally treated using microsurgical clipping. However, introduction and advance of endovascular technique and development of new devices have made it possible to treat ACoA aneurysms using coil embolization. In addition, some studies had revealed that coil embolization of ACoA aneurysm is feasible and effective and there is a tendency to increase coil embolization for treatment of ACoA aneurysms3,7,10,13,14,31,32). However, there are controversies to choice of treatment method for ACoA aneurysms between endovascular treatment and microsurgical clipping due to limitations of each method as ever3,13,32).
Despite these controversies, we have had a tendency to treat ACoA aneurysms using endovascular treatment as a primary treatment tool. We report our experience with the endovascular management of unruptured and ruptured ACoA aneurysms during the past 14 years.
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board at our institution and informed consent was waived. Patient and aneurysm data, clinical record and follow-up data have been prospectively recorded in a database continuously, and were retrospectively analyzed by our neurointervention team.
Patient and aneurysm characteristics
Between March 1997 and November 2011, 2273 aneurysms were occluded using detachable coils in our institution. Among them, 499 (21.9%) were located at the ACoA. Most of the aneurysms were treated in our institution for the first time, and 16 aneurysms had been coiled first at other hospitals and 7 clipped prior to the endovascular treatment. Excluding 47 aneurysms treated using bioactive coils (34 of polyglycolic acid/lactide copolymer-coated coil, 12 of HydroSoft coil and 1 of HydroCoil), 429 aneurysms in 426 patients were considered subjects of the present study. There were 228 (53.5%) male and 198 (46.5%) female patients with mean age 57.2 years (range, 12-83 years). 189 (44.3%) of 426 patients were presented with subarachnoid hemorrhage; 141 of good-grade subarachnoid hemorrhage (SAH) (HH Gr. I-III) and 48 of poor-grade SAH (HH Gr. IV, V). In agreement with our neurosurgery team, the endovascular treatment (EVT) was the primary treatment method for most of ACoA aneurysms in our institute.
Aneurysm analysis
An analysis of aneurysm size was performed with 3-dimensional digital subtraction angiography (3D-DSA) at the time of embolization. 3D-DSA was unavailable in 41 (9.6%) of 426 patients at the earlier period until January 2002. In these cases, linear measurements were obtained using the working projection and geometric comparison with reference vessel or 10 mm-size, round metal marker9). Dome direction of aneurysms was classified as anterior, posterior, superior or inferior42). We measured the aneurysm angle, which was defined as an angle between the main axis of an aneurysm and the parent artery on a working projection at each session of the treatment. The aneurysm angle was classified as ≤90°, 90-135°, and >135°. Variations of parent artery related to the ACoA aneurysm were classified as follows : unilateral A1 aplasia (non-opacification of one A1, filling of both A2 segment from one side) and A1 hypoplasia (1 mm or less of A1 diameter).
Endovascular procedure
Endovascular coil embolization was performed following a standardized protocol with systemic heparinization with or without antiplatelet premedication prior to the procedure in the neuroangiography suite, as describe previously19,21). In the present study, 193 (45.3%) of 426 patients received clopidogrel before the procedure. In most cases, antiplatelet agent was discontinued immediately after the procedure. On the other hand, no antiplatelet premedication was administered to 43 (10.1%) patients with unruptured aneurysm at the earlier period of March 2006 and 190 (44.6%) patients harboring a ruptured aneurysm.
We preferred steam shaping of a microcatheter to employing a preshaped one, depending on the relationship of the aneurysm and the parent artery. Steam shaping provided both a 'pigtail' or 'S' shape which had three subtypes of simple, right and left, as described previously26). Usually, a microcatheter was positioned at an aneurysm through the parent artery to introduce coils into an aneurysm. With an adequate shape of the microcatheter, its tip could be positioned into the aneurysm without a guidance of a wire by simple antegrade shift. If superselection of an aneurysm using a shaped-tip microcatheter was not satisfactory, we modified the shape until a proper selection could be achieved (Fig. 1).
Fig. 1. 52 year-old male patient presents with unruptured ACoA aneurysm. The lesion is posteriorly directed, and the aneurysm angle was 98.2°. A : Working projection of the aneurysm. B : The microcatheter is steam-shaped in the left 'S' shape, and introduced into the aneurysm without guidance of a wire. The first frame coil is inserted through the microcatheter. C : Lateral view of fluoroscopy shows a subsequent coil was stably inserted into the aneurysm. D : Completion angiogram showed that the aneurysm is completely occluded preserving the ACoA. This lesion has been followed up for 3 years, and there is no evidence of recanalization. ACoA : anterior communicating artery.

The aim of coiling was to pack the aneurysm as densely as possible without compromising the parent artery. Intracranial self-expandable stent was deployed in 33 (7.7%) of 429 aneurysms; 28 of Enterprise stent (Cordis, Miami Lakes, FL, USA) and 5 of NeuroForm stent (Boston Scientific, Natick, MA, USA).
Angiographic, clinical outcomes and follow-up protocol
Initial angiographic results were classified as total occlusion, neck remnant and body filling35). Imaging follow-up was done using plan radiography, magnetic resonance angiography (MRA) or DSA according to our pre-specified follow-up protocol. When unruptured aneurysms were successfully embolized, MRA was recommended at 6, 12, 24, and 36 months postembolization. For ruptured aneurysms, plane radiographs were obtained at 1 and 3 months postembolization with the procedural working projection, in addition to the scheduled MRA follow-up. When significant coil compaction or recanalization was suspected in noninvasive studies, conventional angiography was performed to assess the state of the aneurysm exactly, and to determine the need for further treatment. In patients undergoing repeat embolization, the same MRA follow-up protocol was applied following the interventional procedure. If the aneurysm occlusion was found stable 36 months after the initial or repeat treatment, follow-up was either discontinued or continued on a case-by-case basis, e.g., to check other untreated aneurysms. Recanalization was defined as coil loosening or compaction and progressive contrast filling within the aneurysmal sac with or without the aneurysmal growth, requiring additional treatment. All image studies were retrospectively reviewed by our neurointervention team.
Clinical outcome evaluations were performed using a Glasgow Outcome Scale (GOS)18). The patient's follow-up was performed by two neurointerventionists via their own outpatient department.
Statistical analysis
Patient data, aneurysm characteristics, angiographic outcome and risk factors for recanalization were tested as qualitative or continuous variables, as appropriate. Patients were divided into unruptured and ruptured aneurysm groups to evaluate their clinical outcomes. Aneurysms were also classified as either ruptured or unruptured to evaluate aneurysmal characteristics, angiographic outcomes and procedural-related complications. Differences between patient and aneurysm groups were tested using the chi-square or Student t-test.
Univariate analysis to assess the associations between potential risk factors of incomplete occlusion of aneurysm and initial angiographic outcomes was done with the chi-square test and the univariate logistic regression analysis. Then, subsequent stepwise multivariate logistic regression analysis was performed to control potential confounders.
Survival analysis was performed to examine time-to-recanalization. For this analysis, observations were censored when a patient was lost to follow-up or a major recanalization occurred. Kaplan-Meier analysis with the log-rank test was used to plot and compare recanalization-free survival distribution between the unruptured and ruptured groups. Suspected risk factors for major recanalization were evaluated by univariate Cox proportional hazard model. All variables significantly associated with major recanalization (p<0.20) were included in a multivariate model. Because the angiographic outcome is a well-known risk factor for recanalization, it was also included in a multivariate model. A probability value of <0.05 was considered significant. All descriptive and statistical analyses were performed with the SPSS 17.0 software for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Aneurysm characteristics and angiographic outcomes
In terms of aneurysmal characteristics there were no differences between unruptured and ruptured groups, except for the dome-to-neck ratio. The proportion of dome to neck ratio more than 1.5 was significantly higher among unruptured (Table 1).
Table 1. Aneurysm characteristics.
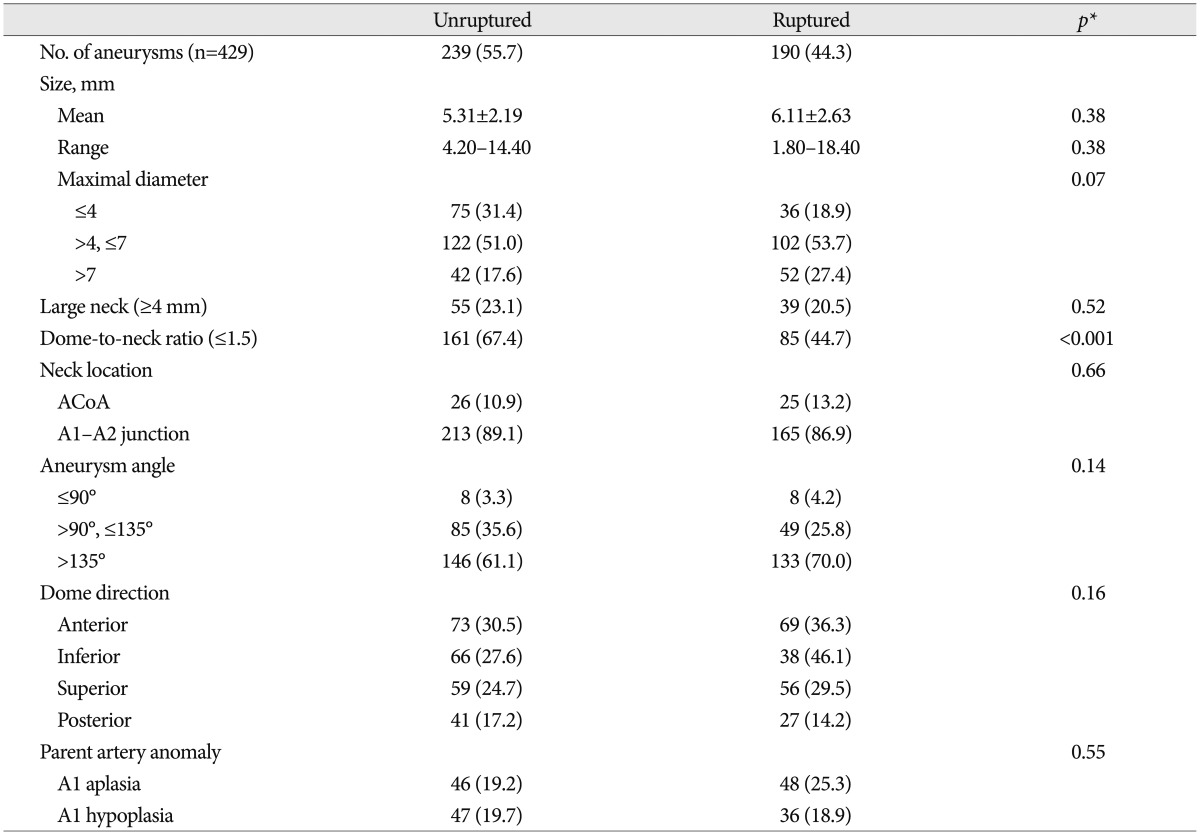
Numbers in parentheses are percentages. *p values derived from Fisher's exact test for dichotomous and categorical variables and the Student t-test for continuous variables. ACoA : anterior communicating artery
Total occlusion was achieved in 290 (67.6%) of 429 aneurysms, neck remnant in 80 (18.6%), and 59 (13.8%). In a patient, we failed to deflate a balloon (HyperForm; ev3, Irvine, CA, USA) during coil embolization, and the aneurysm was clipped after puncture and deflation of the balloon using a fine needle under the operative microscope.
Among all aneurysmal characteristics listed in Table 1, regarding immediate angiographic outcomes, neck size of more than 4 mm {odds ratio (OR), 2.01 [95% confidence interval (CI), 1.10 to 3.68]; p=0.02} and unruptured aneurysms [OR, 2.18 (95% CI, 1.19 to 3.98); p=0.01] were significant factors related to incomplete occlusion of aneurysms. The other aneurysm characteristics, including dome direction and aneurysm angle, were not associated with initial angiographic outcomes (Table 2).
Table 2. Initial angiographic outcomes according to dome direction and aneurysm angle.
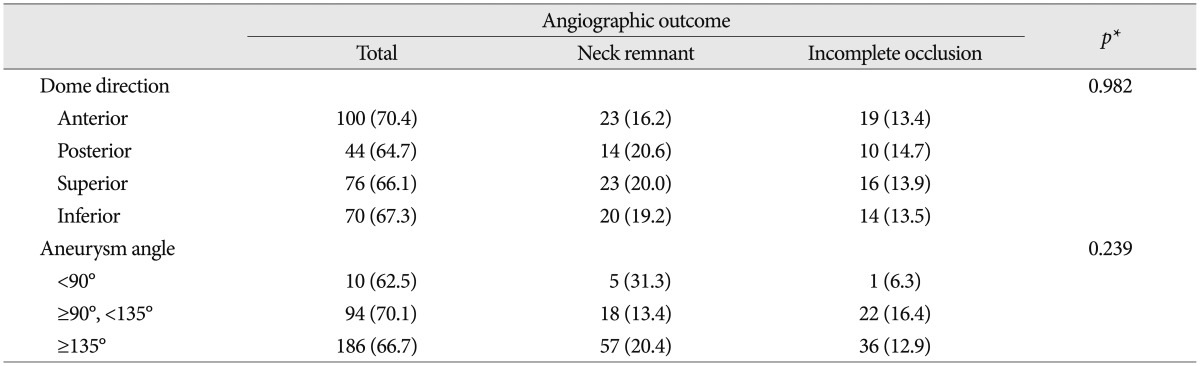
Numbers in parentheses are percentages. *p values derived from chi-square test
Periprocedural adverse events
Periprocedural adverse events occurred in 69 (16.1%) of 429 procedures. Those for unruptured and ruptured groups were 11.7% (28/239) and 21.6% (41/190), respectively, and there was no statistically significant difference.
Thromboembolic complications were more prevalent in ruptured group (8.3% vs. 14.8%, p=0.04). Of the 48 thromboembolic complications developed during procedures, the majority (n=42) were asymptomatic. Among 6 symptomatic patients, 2 (0.8%) belonged to unruptured group and 4 (2.1%) ruptured group, and 3 (0.7%) had delayed thromboembolic complications, all of whom had been treated with stent-assisted technique. Permanent neurologic deficits were remained in 3 (0.7%) patients related to the thromboembolic complications; 1 (0.4%) of the unruptured group and 2 (1.1%) of the ruptured group. Except for 3 cases of permanent neurologic deficits, the other patients were fully recovered with conservative management including antiplatelet medication. Patients with unruptured aneurysms showed a lower rate of thromboembolic complications when they were given antiplatelet premedication before procedures with no hemorrhagic complications (6.2% vs. 20.9%; p=0.02).
Intra-procedural bleeding of aneurysms occurred in 18 (4.2%) of 429 procedures; 8 (3.3%) of unruptured group, and 10 (5.2%) of ruptured group. One patient had thromboembolic complication and aneurysmal rupture simultaneously. This patient was initially presented with SAH (HH Gr. I). Even though we achieved total occlusion of the lesion, the ipsilateral anterior cerebral artery (ACA) was occluded at the end of the procedure. Because of the ACA territorial infarction, the patient showed poor clinical outcome (GOS=3). Another patient, having suffered from non-leakage perforation, stayed bedridden (GOS=2) at the last follow-up. The patient had initially presented with SAH and massive intraventricular hemorrhage (HH Gr. IV). Except these 2 cases, 16 (88.9%) of 18 procedural rupture cases showed excellent clinical outcomes (GOS=5) at the last follow-up.
Three (1.6%) of ruptured group experienced rebleeding after coil embolization. Two of 3 cases accompanied an adjacent intracerebral hemorrhage (ICH). In two of 3 cases, completion control angiogram showed thrombus formation around the deployed coil, and an intra-arterial infusion of tirofiban was performed to resolve the clot22). One of these 2 patients died (GOS=1) and the other became vegetative status (GOS=2). The other one presented with a 2-mm sized ruptured aneurysm. We achieved total occlusion without any procedural-related complications. The patient complained severe, bursting headache at the fifteenth day of the procedure. CT scan revealed rebleeding, and the follow-up angiography showed enlargement of the aneurysmal sac (maximal diameter of 7.2 mm). Immediate repeat coil embolization was performed and the patient showed favorable clinical outcome (GOS=4) at 6-month follow-up.
Recanalization
Three hundred eighty two (89.0%) of the 429 aneurysms were examined by plain radiograph and/or MRA and/or DSA for more than 6 months after coil embolization. Any degree of recanalization was revealed in 45 (11.7%) of 382 followed-up aneurysms via non-invasive study, i.e. plain radiography and MRA. Among them, DSA was performed to confirm the recanalization in all of 45 aneurysms, and retreatment was required in 30 (7.9%) of 45 aneurysms. Kaplan-Meire analysis revealed that the overall cumulative risk of recanalization was 5% at 12 months, 7% at 24 months, 8% at 36 months and 11% at 48 months. The cumulative risk of recanalization at 12, 24, 36, and 48 months was 3%, 5%, 5%, and 5% in unruptured group, and 8%, 12%, 13%, and 16% in ruptured group. The cumulative risk of major recanalization required retreatment was significantly higher in the ruptured group (Fig. 2). All the recanalized aneurysms (n=30) were retreated by endovascular treatment without any procedure-related complications. Multivariate Cox proportional hazard model revealed that significant factors related to recanalization were neck size of more than 4 mm [hazard ratio (HR), 5.66 (95% CI, 2.74 to 60.8); p<0.001], ruptured aneurysm [HR, 2.31 (95% CI, 1.10 to 4.90); p=0.03] and A1 segment aplasia [OR, 2.81 (95% CI, 1.21 to 6.49); p=0.02]. Body filling of immediate angiographic outcome showed borderline significance for major recanalization [OR, 2.06 (95% CI, 0.99 to 5.35); p=0.056]. The other aneurysmal characteristics, including dome direction and aneurysm angle were not associated with major recanalization.
Fig. 2. Kaplan-Meire analysis demonstrates the proportion of patients without major recanalization during follow-up.

Clinical outcome
At the last follow-up there were more patients of poor clinical outcomes (GOS, 1 to 3) in ruptured group (20.5% vs. 0.4%; p<0.001, Fisher's exact test), and significantly associated with the patient's clinical grade at admission (p<0.001, chi-square test) (Table 3). Fourteen (3.2%) of 426 patients died and there was no mortality in unruptured group. Except for 3 cases (1 case of procedural rupture accompanied by thromboembolism and 2 cases of thromboembolic complications), all neurologic deficits of 61 patients were associated with SAH itself in ruptured group. Eventually, procedure-related morbidity and mortality rates were 1.6% and 0% in ruptured group, respectively.
Table 3. Clinical outcomes at the last follow-up.

Numbers in parentheses are percentages. UIA : unruptured intracranial aneurysm, GOS : Glasgow Outcome Scale
In unruptured group, 235 (99.1%) of 237 patients showed excellent clinical outcomes (GOS of 5). One of 2 complicated cases was showed poor clinical outcome due to symptomatic thromboembolic complications (GOS of 3). After all, procedure-related morbidity in unruptured group was one (0.4%) case resulting in both ACA territorial infarctions (GOS of 3).
DISCUSSION
Their deep location, complex arterial relationship and frequent association with anomalies of the ACoA make microsurgical clipping of ACoA aneurysms difficult1,16,37). Recently endovascular techniques for treatment of ACoA aneurysm has become popular, and the efficacy and outcomes of endovascular treatment of ACoA aneurysms have been reported31). However, there are concerns about morphological limitations including dome direction in the endovascular approach to the ACoA aneurysm3,13,14,32). In the present study, dome direction of aneurysm and aneurysm angle were not associated with immediate angiographic outcomes (Table 2). We could surmount these anatomical limitations with the appropriate shaping of a microcatheter. We tailored the shape of a microcatheter tip according to the individual anatomy and geometry of the aneurysm and parent arteries. The introduction of rotational 3D-DSA makes a decision of shape more delicate. An application of the appropriately shaped microcatheter provided intra-aneurysmal stability of the microcatheter during coil embolization. Intra-aneurysmal positioning of the microcatheter harboring an inappropriately shaped tip would be prone to result in premature kickback of the microcatheter, and would interfere dense coil packing. Considering the intricacy of the ACoA complex, optimal shaping of a microcatheter tip is prerequisite in coil embolization of an ACoA aneurysm. We believe tailored microcatheter steam shape resulted in good immediate and long-term angiographic outcomes with low rate of periprocedural complications compared with other serieses (Table 4).
Table 4. Results of a literature review of outcomes of ACoA aneurysms treated by coil embolization.
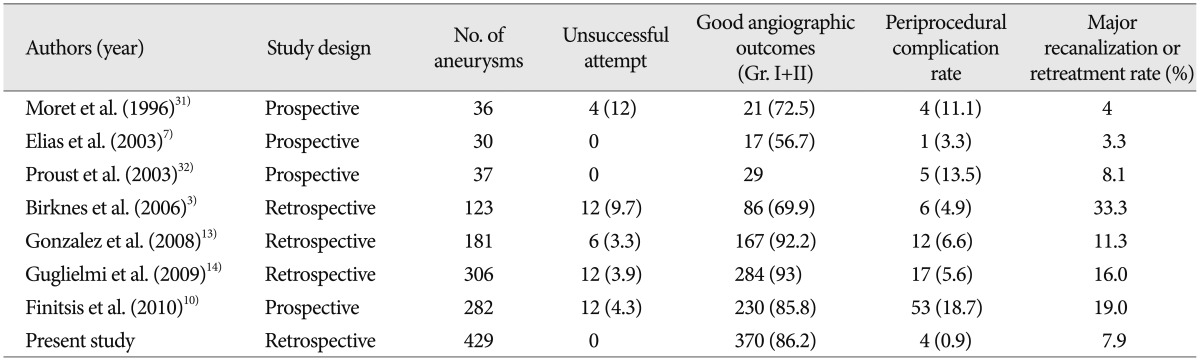
Numbers in parenthesis are percentages. ACoA : anterior communicating artery
In our series of ACoA aneurysms, initial incomplete occlusion tended to lead to aneurysmal recanalization. Even though incomplete occlusion was prominent in the group of unruptured aneurysm in the present study, however, recanlization of coiled aneurysms was more prevalent in the group of ruptured aneurysm. Systemic heparinization with or without antiplatelet medication for coil embolization of the unruptured aneurysm might lead to these results. Moreover, SAH produces a hypercoagulable state and there is a higher tendency for thrombus formation in those patients12). Consequently, even with less compact coil mesh, we could achieve total occlusion more easily in ruptured aneurysms compared with unruptured lesions. These phenomena would interrupt the strong association between an initial angiographic outcome and a tendency to recanalization.
In our series the procedural aneurysmal rupture rate was 4.2%, and the clinical outcomes were favorable with only 0.5% of morbidity rate and no mortality. This is comparable to the published data of intraprocedural rupture which is more frequent during microsurgical clipping than coil embolization8). Overall premature intraoperative rupture rates with microsurgery occurred up to 40% of the patients during microsurgical clipping, and the morbidity and mortality rates for them have been reported to be up to 35%8,36). Due to tortuosity and small diameter of A1 segment, however, ACoA aneurysms are known to be more vulnerable to procedural perforation than aneurysms arising at other sites during the coil embolization25). Even though rapid counter-measures against intraprocedural rupture could reduce morbidity and mortality, we need to be more cautious during coil embolization for ACoA aneurysms due to its high prevalence in ACoA aneurysms and its potentially catastrophic clinical outcomes.
The results from the International Study of Unruptured Intracranial Aneurysms (ISUIA) revealed that the unruptured aneurysms have a minimal rupture risk, and suggested that preventive treatments of unruptured aneurysm could be rarely justified40,41). In the group of unruptured aneurysms of the present study, procedure-related morbidity rate (0.4%) was very low and there was no mortality. Compared with annual rupture rate of unruptured aneurysms observed ISUIA studies, the present study showed that lower procedure-related morbidity and mortality rate than the rupture rate of unruptured intracranial aneurysms. In addition, a meta-analysis and several other studies have demonstrated that ACoA aneurysms have a higher rupture risk than those at other locations17,23,27,39). According to them, the annual risks of rupture for unruptured ACoA aneurysm ranged from 1.6% to 5.8%. The present study also showed that thromboembolic complications could be significantly reduced with antiplatelet premedication in cases of unruptured ACoA aneurysms19). As a result, regarding the treatment of unruptured ACoA aneurysm, endovascular treatment would be a beneficial and safe therapeutic tool.
Some microsurgical series for ACoA aneurysms, which included ruptured and unruptured lesions, showed that the proportion of excellent clinical outcome reached as high as 65% and the mortality rate ranged between 3.5% and 10.4%6,24,32). In the present study, the proportion of excellent clinical outcome (GOS=5) and mortality rate were 67.3%, and 7.4% in the group of ruptured aneurysm. Considering that surgical series included unruptured aneurysms, the results of our endovascularly treated ruptured group was comparable with previously reported surgical groups. In addition, the International Subarachnoid Aneurysm Trial studies presented the endovascular procedure as an alternative with better immediate and long-term outcomes28,29,30). Moreover, the microsurgical treatment of ACoA aneurysm has a higher tendency to develop variable neurophysiologic deficit, including memory, executive or cognitive function, and brain injury, which is more prevalent among patients with SAH, than endovascular treatment2,5,11,33). Consequently, endovascular technique might be preferable to treat most of ruptured ACoA aneurysms.
One concern about the coil embolization of ruptured ACoA aneurysm is early rebleeding after the procedure. The 1.6% incidence of early rebleeding after coil embolization of ruptured group is in concordance with previously reported studies28,38). In a report, adjacent ICH, ACoA localization and small size of aneurysm were strong risk factors for early rebleeding after coil embolization of ruptured aneurysms38). All three rebleeding cases of the present study presented with SAH accompanied by adjacent ICH. In such cases, short-term imaging follow-up and close observation should be performed for detection reopening of the aneurysms after coil embolization, or else microsurgical clipping could be considered as the first-line treatment. Another major concern about coiling of ACoA aneurysm is long-term durability of coiled aneurysms. Aneurysm recanalization occurs more frequently with EVT than with microsurgical clipping30,34). Thus, radiologic follow-up is mandatory for optimal management in order to identify recanalization of coiled aneurysm and prevent rebleeding. In our series, all major recanalization was treated by using EVT without procedural related complications. As reported in the literature, retreatment by using EVT of recanalized aneurysms is less likely to increase the risk of procedure-related complications15,20). Neck size more than 4 mm, ruptured aneurysms, A1 aplasia and incomplete occlusion of aneurysm were significant predictor of recanalization, as identified previously13,14,32). Usually, posteriorly directed ACoA aneurysm is difficult to achieve complete occlusion that is associated with higher tendency of recanalization13,14). However, this study revealed that dome direction was not associated with recanalization. An application of tailored steam shaped microcatheter would indirectly result in no differences of recanalization rate between differently directed aneurysms.
Aside from the general limitations of the retrospective, single-center study, there are other limitations in this study. Comparison with the neurosurgical series was not feasible, and represents a minor limitation of our study. Data presenting the outcome of microsurgical treatment of the specific ACoA aneurysm topography are extremely poor, and it is not appropriate to compare our results with microsurgical series dealing with various locations. Thus, treatment of ACoA aneurysms either by using EVT or microsurgical approach needs further confirmation in a large multicenter study.
CONCLUSION
The endovascular treatment for ACoA aneurysms seems to be applicable to most of ACoA aneurysms, either runruptured or ruptured, with an acceptable procedure-related complications rate and favorable long-term angiographic and clinical outcomes. We believe the tailored steam shaping of the microcatheter tip exerts favorable influence on achieving good angiographic results and a long-term durability regardless of aneurysmal direction.
Acknowledgements
We thank Mi-Sun Ko, BA for assistance with data retrieval vital for the conduct of this study.
This study was supported by a grant of the Korean health technology R&D Project, Ministry of Health & Welfare, Republic of Korea (No. A110506).
References
- 1.Agrawal A, Kato Y, Chen L, Karagiozov K, Yoneda M, Imizu S, et al. Anterior communicating artery aneurysms : an overview. Minim Invasive Neurosurg. 2008;51:131–135. doi: 10.1055/s-2008-1073169. [DOI] [PubMed] [Google Scholar]
- 2.Akyuz M, Erylmaz M, Ozdemir C, Goksu E, Ucar T, Tuncer R. Effect of temporary clipping on frontal lobe functions in patients with ruptured aneurysm of the anterior communicating artery. Acta Neurol Scand. 2005;112:293–297. doi: 10.1111/j.1600-0404.2005.00483.x. [DOI] [PubMed] [Google Scholar]
- 3.Birknes JK, Hwang SK, Pandey AS, Cockroft K, Dyer AM, Benitez RP, et al. Feasibility and limitations of endovascular coil embolization of anterior communicating artery aneurysms : morphological considerations. Neurosurgery. 2006;59:43–52. doi: 10.1227/01.NEU.0000219220.25721.B9. discussion 43-52. [DOI] [PubMed] [Google Scholar]
- 4.Brisman JL, Song JK, Newell DW. Cerebral aneurysms. N Engl J Med. 2006;355:928–939. doi: 10.1056/NEJMra052760. [DOI] [PubMed] [Google Scholar]
- 5.Chan A, Ho S, Poon WS. Neuropsychological sequelae of patients treated with microsurgical clipping or endovascular embolization for anterior communicating artery aneurysm. Eur Neurol. 2002;47:37–44. doi: 10.1159/000047945. [DOI] [PubMed] [Google Scholar]
- 6.Diraz A, Kobayashi S, Toriyama T, Ohsawa M, Hokama M, Kitazama K. Surgical approaches to the anterior communicating artery aneurysm and their results. Neurol Res. 1993;15:273–280. doi: 10.1080/01616412.1993.11740148. [DOI] [PubMed] [Google Scholar]
- 7.Elias T, Ogungbo B, Connolly D, Gregson B, Mendelow AD, Gholkar A. Endovascular treatment of anterior communicating artery aneurysms : results of clinical and radiological outcome in Newcastle. Br J Neurosurg. 2003;17:278–286. doi: 10.1080/0268869031000153251. [DOI] [PubMed] [Google Scholar]
- 8.Elijovich L, Higashida RT, Lawton MT, Duckwiler G, Giannotta S, Johnston SC, et al. Predictors and outcomes of intraprocedural rupture in patients treated for ruptured intracranial aneurysms : the CARAT study. Stroke. 2008;39:1501–1506. doi: 10.1161/STROKEAHA.107.504670. [DOI] [PubMed] [Google Scholar]
- 9.Fernandez Zubillaga A, Guglielmi G, Viñuela F, Duckwiler GR. Endovascular occlusion of intracranial aneurysms with electrically detachable coils : correlation of aneurysm neck size and treatment results. AJNR Am J Neuroradiol. 1994;15:815–820. [PMC free article] [PubMed] [Google Scholar]
- 10.Finitsis S, Anxionnat R, Lebedinsky A, Albuquerque PC, Clayton MF, Picard L, et al. Endovascular treatment of ACom intracranial aneurysms. Report on series of 280 patients. Interv Neuroradiol. 2010;16:7–16. doi: 10.1177/159101991001600101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fontanella M, Perozzo P, Ursone R, Garbossa D, Bergui M. Neuropsychological assessment after microsurgical clipping or endovascular treatment for anterior communicating artery aneurysm. Acta Neurochir (Wien) 2003;145:867–872. doi: 10.1007/s00701-003-0111-5. discussion 872. [DOI] [PubMed] [Google Scholar]
- 12.Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Koike T, Tanaka R. Serial changes of hemostasis in aneurysmal subarachnoid hemorrhage with special reference to delayed ischemic neurological deficits. J Neurosurg. 1997;86:594–602. doi: 10.3171/jns.1997.86.4.0594. [DOI] [PubMed] [Google Scholar]
- 13.Gonzalez N, Sedrak M, Martin N, Vinuela F. Impact of anatomic features in the endovascular embolization of 181 anterior communicating artery aneurysms. Stroke. 2008;39:2776–2782. doi: 10.1161/STROKEAHA.107.505222. [DOI] [PubMed] [Google Scholar]
- 14.Guglielmi G, Viñuela F, Duckwiler G, Jahan R, Cotroneo E, Gigli R. Endovascular treatment of 306 anterior communicating artery aneurysms : overall, perioperative results. J Neurosurg. 2009;110:874–879. doi: 10.3171/2008.10.JNS081005. [DOI] [PubMed] [Google Scholar]
- 15.Henkes H, Fischer S, Liebig T, Weber W, Reinartz J, Miloslavski E, et al. Repeated endovascular coil occlusion in 350 of 2759 intracranial aneurysms : safety and effectiveness aspects. Neurosurgery. 2006;58:224–232. doi: 10.1227/01.NEU.0000194831.54183.3F. discussion 224-232. [DOI] [PubMed] [Google Scholar]
- 16.Hernesniemi J, Dashti R, Lehecka M, Niemelä M, Rinne J, Lehto H, et al. Microneurosurgical management of anterior communicating artery aneurysms. Surg Neurol. 2008;70:8–28. doi: 10.1016/j.surneu.2008.01.056. discussion 29. [DOI] [PubMed] [Google Scholar]
- 17.Inagawa T. Multiple intracranial aneurysms in elderly patients. Acta Neurochir (Wien) 1990;106:119–126. doi: 10.1007/BF01809453. [DOI] [PubMed] [Google Scholar]
- 18.Jennett B, Snoek J, Bond MR, Brooks N. Disability after severe head injury : observations on the use of the Glasgow Outcome Scale. J Neurol Neurosurg Psychiatry. 1981;44:285–293. doi: 10.1136/jnnp.44.4.285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kang HS, Han MH, Kwon BJ, Jung C, Kim JE, Kwon OK, et al. Is clopidogrel premedication useful to reduce thromboembolic events during coil embolization for unruptured intracranial aneurysms? Neurosurgery. 2010;67:1371–1376. doi: 10.1227/NEU.0b013e3181efe3ef. discussion 1376. [DOI] [PubMed] [Google Scholar]
- 20.Kang HS, Han MH, Kwon BJ, Kwon OK, Kim SH. Repeat endovascular treatment in post-embolization recurrent intracranial aneurysms. Neurosurgery. 2006;58:60–70. doi: 10.1227/01.neu.0000194188.51731.13. discussion 60-70. [DOI] [PubMed] [Google Scholar]
- 21.Kang HS, Kwon BJ, Kim JE, Han MH. Preinterventional clopidogrel response variability for coil embolization of intracranial aneurysms : clinical implications. AJNR Am J Neuroradiol. 2010;31:1206–1210. doi: 10.3174/ajnr.A2051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kang HS, Kwon BJ, Roh HG, Yoon SW, Chang HW, Kim JE, et al. Intra-arterial tirofiban infusion for thromboembolism during endovascular treatment of intracranial aneurysms. Neurosurgery. 2008;63:230–237. doi: 10.1227/01.NEU.0000320440.85178.CC. discussion 237-238. [DOI] [PubMed] [Google Scholar]
- 23.Kappelle LJ, Eliasziw M, Fox AJ, Barnett HJ North American Symptomatic Carotid Endarterectomy Trial Group. Small, unruptured intracranial aneurysms and management of symptomatic carotid artery stenosis. Neurology. 2000;55:307–309. doi: 10.1212/wnl.55.2.307. [DOI] [PubMed] [Google Scholar]
- 24.Keogh AJ, Sharma RR, Vanner GK. The anterior interhemispheric trephine approach to anterior midline aneurysms : results of treatment in 72 consecutive patients. Br J Neurosurg. 1993;7:5–12. doi: 10.3109/02688699308995050. [DOI] [PubMed] [Google Scholar]
- 25.Kwon BJ, Chang HW, Youn SW, Kim JE, Han MH. Intracranial aneurysm perforation during endosaccular coiling : impact on clinical outcome, initial occlusion, and recanalization rates. Neurosurgery. 2008;63:676–672. doi: 10.1227/01.NEU.0000325500.73330.C2. discussion 682-683. [DOI] [PubMed] [Google Scholar]
- 26.Kwon BJ, Im SH, Park JC, Cho YD, Kang HS, Kim JE, et al. Shaping and navigating methods of microcatheters for endovascular treatment of paraclinoid aneurysms. Neurosurgery. 2010;67:34–40. doi: 10.1227/01.NEU.0000370891.67129.2F. discussion 40. [DOI] [PubMed] [Google Scholar]
- 27.Mira JM, Costa FA, Horta BL, Fabião OM. Risk of rupture in unruptured anterior communicating artery aneurysms : meta-analysis of natural history studies. Surg Neurol. 2006;66(Suppl 3):S12–S19. doi: 10.1016/j.surneu.2006.06.025. discussion S19. [DOI] [PubMed] [Google Scholar]
- 28.Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms : a randomised trial. Lancet. 2002;360:1267–1274. doi: 10.1016/s0140-6736(02)11314-6. [DOI] [PubMed] [Google Scholar]
- 29.Molyneux AJ, Kerr RS, Birks J, Ramzi N, Yarnold J, Sneade M, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT) : long-term follow-up. Lancet Neurol. 2009;8:427–433. doi: 10.1016/S1474-4422(09)70080-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms : a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809–817. doi: 10.1016/S0140-6736(05)67214-5. [DOI] [PubMed] [Google Scholar]
- 31.Moret J, Pierot L, Boulin A, Castaings L, Rey A. Endovascular treatment of anterior communicating artery aneurysms using Guglielmi detachable coils. Neuroradiology. 1996;38:800–805. doi: 10.1007/s002340050352. [DOI] [PubMed] [Google Scholar]
- 32.Proust F, Debono B, Hannequin D, Gerardin E, Clavier E, Langlois O, et al. Treatment of anterior communicating artery aneurysms : complementary aspects of microsurgical and endovascular procedures. J Neurosurg. 2003;99:3–14. doi: 10.3171/jns.2003.99.1.0003. [DOI] [PubMed] [Google Scholar]
- 33.Proust F, Martinaud O, Gérardin E, Derrey S, Levèque S, Bioux S, et al. Quality of life and brain damage after microsurgical clip occlusion or endovascular coil embolization for ruptured anterior communicating artery aneurysms : neuropsychological assessment. J Neurosurg. 2009;110:19–29. doi: 10.3171/2008.3.17432. [DOI] [PubMed] [Google Scholar]
- 34.Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003;34:1398–1403. doi: 10.1161/01.STR.0000073841.88563.E9. [DOI] [PubMed] [Google Scholar]
- 35.Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001;32:1998–2004. doi: 10.1161/hs0901.095600. [DOI] [PubMed] [Google Scholar]
- 36.Schramm J, Cedzich C. Outcome and management of intraoperative aneurysm rupture. Surg Neurol. 1993;40:26–30. doi: 10.1016/0090-3019(93)90165-w. [DOI] [PubMed] [Google Scholar]
- 37.Sekhar LN, Natarajan SK, Britz GW, Ghodke B. Microsurgical management of anterior communicating artery aneurysms. Neurosurgery. 2007;61(5) Suppl 2:273–290. doi: 10.1227/01.neu.0000303980.96504.d9. discussion 290-292. [DOI] [PubMed] [Google Scholar]
- 38.Sluzewski M, van Rooij WJ. Early rebleeding after coiling of ruptured cerebral aneurysms : incidence, morbidity, and risk factors. AJNR Am J Neuroradiol. 2005;26:1739–1743. [PMC free article] [PubMed] [Google Scholar]
- 39.Tsutsumi K, Ueki K, Morita A, Kirino T. Risk of rupture from incidental cerebral aneurysms. J Neurosurg. 2000;93:550–553. doi: 10.3171/jns.2000.93.4.0550. [DOI] [PubMed] [Google Scholar]
- 40.Wiebers DO. Unruptured intracranial aneurysms : natural history and clinical management. Update on the international study of unruptured intracranial aneurysms. Neuroimaging Clin N Am. 2006;16:383–390. vii. doi: 10.1016/j.nic.2006.04.005. [DOI] [PubMed] [Google Scholar]
- 41.Wiebers DO, Whisnant JP, Huston J, 3rd, Meissner I, Brown RD, Jr, Piepgras DG, et al. Unruptured intracranial aneurysms : natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–110. doi: 10.1016/s0140-6736(03)13860-3. [DOI] [PubMed] [Google Scholar]
- 42.Yaşargil MG. Anterior communicating artery aneurysm. In: Yaşargil MG, editor. Microneurosurgery. Vol II. New-York: Thieme-Verlag; 1984. pp. 169–223. [Google Scholar]