

Abstract
Background and Objectives:
The most caries-susceptible period of a permanent first molar tooth is the eruption phase, during which the enamel is not fully matured and it is usually difficult for the child to clean the erupting tooth surfaces. Sealing occlusal pits and fissures with resin-based pit and fissure sealants is a proven method to prevent occlusal caries. The difference in the viscosity of the sealants differs in the penetration into pit and fissures and abrasive wear resistance property due to the addition of filler particles. The present study was conducted to evaluate and compare the retention of the resin-based filled (Helioseal F, Ivoclar Vivadent) and unfilled (Clinpro, 3M ESPE) pit and fissure sealants, which is important for their effectiveness.
Materials and Methods:
Fifty-six children between the age group of 6 and 9 years, with all four newly erupted permanent first molars were selected. Sealants were applied randomly using split mouth design technique on permanent first molars. Evaluation of sealant retention was performed at regular intervals over 12 months, using Simonsen's criteria at 2nd, 4th, 6th, 8th, 10th and 12th month. The results were subjected to statistical analysis.
Results:
At the end of our study period (12th month), 53.57% showed complete retention, 37.50% showed partial retention, and 8.83% showed complete missing of resin-based filled (Helioseal F) pit and fissure sealant. And, 64.29% showed complete retention, 32.14% showed partial retention, and 3.57% showed complete missing of resin-based unfilled (Clinpro) pit and fissure sealant. This difference in retention rates between filled and unfilled pit and fissure sealants was not statistically significant.
Conclusion:
The difference in retention rates between Helioseal F and Clinpro was not statistically significant, but Clinpro (unfilled) sealant showed slightly higher retention rates and clinically better performance than Helioseal F (filled).
Keywords: Filled, pit and fissure, retention, sealant, unfilled
Introduction
Pits and fissures are generally considered as faults or imperfections in cuspal odontogenesis. They have been considered as the single most important feature leading to the development of occlusal caries. The complex morphology of occlusal pits and fissures makes them an ideal site for retention of bacteria and food remnants, rendering the performance of proper hygiene difficult or even impossible.[1] The most caries-susceptible period of the first permanent molar is the long eruption phase as the enamel is immature during this period. Preventive measures such as control of bacterial plaque and topical application of fluoride solutions have little effect on such surfaces. More effective measures are, therefore, necessary, such as application of occlusal sealants.[2]
Since 1920's several attempts have been made to protect pits and fissures, such as physical blocking of fissures with zinc phosphate cement, prophylactic odontotomy and fissures eradication were all tried, but with little success. Nevertheless, these efforts to prevent pit and fissure decay succeeded only after 1955, when Buonocore published his classic study documenting a pioneer method for mechanical bonding of acrylic resin to the dental enamel previously etched with phosphoric acid. The first clinical benefit from Buonocore's work was the introduction of the first dental pit and fissure sealant, Nuva-Seal (L.D Caulk) in February 1971 along with its curing initiator and ultraviolet light source, the Caulk Nuva Lite.[3]
The properties required of an ideal fissure sealant include biocompatibility, anticariogenicity, adequate bond strength, good marginal integrity, resistance to abrasion and wear, and cost effectiveness. The clinical efficiency of fissure sealants is directly related to their retention.[4] Retention depends on morphology of pits and fissures, adequate isolation, conditioning of enamel, application techniques, particular material characteristics like viscosity, surface tension, and adequate adhesion (that is, penetration of the material into the previously etched system of fissures).[5,6]
In recent years resin-based filled and unfilled fluoridated sealants have been introduced, and fluoride has been added as a caries-preventive ingredient.[7] The effectiveness and success of the sealant depend on its retention by penetrating into the pits and fissures and into the micropores of the etched enamel surface.[4] Hence the present study was conducted to evaluate and compare the retention of the Resin-based filled (Helioseal F, Ivoclar Vivadent) and unfilled (Clinpro, 3M ESPE) pit and fissure sealants, which is important for their effectiveness.
Materials and Methods
The present study was carried out in the Department of Pedodontics and Preventive Dentistry, Sri Siddhartha Dental College and Hospital, Tumkur, Karnataka.
Consent was obtained from the school authorities for screening of school children from Sri Siddaganga Mutt, Tumkur. One hundred and fifty children aged between 6 and 9 years, 1st, 2nd and 3rd standard children, were examined in the Department of Pedodontics and Preventive Dentistry using a mouth mirror and dental explorer. The inclusion criteria specified that the healthy co-operative children of age 6–9 years with all four newly erupted permanent first molars, which were caries-free, nonrestored and unsealed, occlusal surface fully visible and free of mucosal tissue and deep pits and fissures indicated for pit and fissure sealant have been selected. The children with carious, restored and developmental anomalies of permanent first molars were excluded from the study.
Out of 150 children examined, 56 children had fulfilled the inclusion criteria. Ethical clearance to conduct the study was obtained from the Institutional Ethical Committee. Written consent from the legal guardian of children from Sri Siddaganga Mutt was taken.
A single operator carried out scaling procedures for each child, followed by prophylaxis using slurry of pumice and a rotating brush to ensure removal of debris from the fissures. The occlusal surfaces of all four first permanent molars were then thoroughly flushed with water to remove all traces of pumice slurry. An explorer tine was used to remove as much residual plaque as possible from the occlusal surfaces of pits and fissures. Isolation of permanent first molars was obtained using cotton rolls, and saliva ejector was held by an assistant.[4]
The occlusal surface of permanent first molars was dried and 37% phosphoric acid etchant (3M ESPE) was applied with a disposable nylon brush into the pits and fissures, and extended up to the cuspal inclines. Each tooth was etched for 45 s, and then rinsed thoroughly for 30 s using an oil-free air-water syringe. The cotton rolls were substituted taking care not to contaminate the etched surfaces which were then thoroughly blow dried. Etching was confirmed by a dull frosty-white appearance of the enamel. If salivary contamination occurred, the surface was again cleaned, dried and re-etched.[4]
The light-cure resin-based sealant, Helioseal F (Ivoclar Vivadent) and Clinpro (3M ESPE) was applied randomly using split mouth design technique on permanent first molars and light-cured using light-cure unit (3M ESPE). High points were checked using articulating paper and corrected. Polishing was done using composite polishing burs (SHOFU) in a single visit. All the children were recalled for assessment of sealant retention at intervals of 2nd, 4th, 6th, 8th, 10th and 12th month by a single blind examiner throughout the study period. Retention of the sealants at the specified time intervals was evaluated using Simonsen's criteria.[8] Data collected were entered in Microsoft Excel 2007 and analyzed using SPSS, 16 software (IBM Corporation). Descriptive statistics like percentage and proportion was carried, and the test of significance was done using Z-test (difference between two proportions).
Results
Comparison of the retention of resin-based filled (Helioseal F) and resin-based unfilled (Clinpro) sealant
At 2nd month evaluation of resin-based filled pit and fissure sealant, 77.68% (87 teeth) showed complete retention, 17.86% (20 teeth) showed partial retention, and 4.46% (5 teeth) showed complete missing of sealant. Whereas, 83.04% (93 teeth) showed complete retention, 16.07% (18 teeth) showed partial retention, and 0.89% (1 tooth) showed complete missing of resin-based unfilled pit and fissure sealant. During 4th month evaluation of resin-based filled pit and fissure sealant, 75.89% (85 teeth) showed complete retention, 19.64% (22 teeth) showed partial retention, and 4.46% (5 teeth) showed complete missing of sealant. Whereas, 83.04% (93 teeth) showed complete retention, 16.07% (18 teeth) showed partial retention, and 0.89% (1 tooth) showed complete missing of resin-based unfilled pit and fissure sealant. The difference in the degree of retention rate between two sealants was not statistically significant during 2nd and 4th month evaluation.
At 6th month evaluation of resin-based filled pit and fissure sealant, 71.43% (80 teeth) showed complete retention, 22.32% (25 teeth) showed partial retention, and 6.25% (7 teeth) showed complete missing of sealant. Whereas, 80.36% (90 teeth) showed complete retention, 18.75% (21 teeth) showed partial retention, and 0.89% (1 tooth) showed complete missing of resin-based unfilled pit and fissure sealant. The difference in complete retention and partial retention of two sealants was not statistically significant, but the complete missing of sealant was more in resin-based filled pit and fissure sealant, which was statistically significant (P < 0.05) when compared with resin-based unfilled pit and fissure sealant.
At 8th month evaluation of resin-based filled pit and fissure sealant, 63.39% (71 teeth) showed complete retention, 28.57% (32 teeth) showed partial retention, and 8.04% (9 teeth) showed complete missing of sealant. Whereas, 80.36% (90 teeth) showed complete retention, 18.75% (21 teeth) showed partial retention, and 0.89% (1 tooth) showed complete missing of resin-based unfilled pit and fissure sealant. The difference in complete retention and partial retention of two sealants was not statistically significant, but the complete missing of sealant was more in resin-based filled pit and fissure sealant which was statistically significant (P < 0.05) when compared with resin-based unfilled pit and fissure sealant, as seen in 6th month follow-up.
At 10th month evaluation of resin-based filled pit and fissure sealant, 57.14% (64 teeth) showed complete retention, 34.82% (39 teeth) showed partial retention, and 8.04% (9 teeth) showed complete missing of sealant. Whereas, 69.64% (78 teeth) showed complete retention, 27.68% (31 teeth) showed partial retention, and 2.68% (3 teeth) showed complete missing of resin-based unfilled pit and fissure sealant. The complete retention of the sealant was less in resin-based filled pit and fissure sealant which was statistically significant (P < 0.05) when compared with resin-based unfilled pit and fissure sealant.
During 12th month and final evaluation of resin-based filled pit and fissure sealant, 53.57% (60 teeth) showed complete retention, 37.5% (42 teeth) showed partial retention, and 8.93% (10 teeth) showed complete missing of sealant. Whereas, 64.29% (72 teeth) showed complete retention, 32.14% (36 teeth) showed partial retention, and 3.57% (4 teeth) showed complete missing of resin-based unfilled pit and fissure sealant. There was no statistically significant difference in the retention rate of resin-based filled (Helioseal F) pit and fissure sealant when compared with resin-based unfilled (Clinpro) pit and fissure sealants [Table 1 and Figure 1].
Table 1.
Comparison of the retention of resin-based filled (Helioseal F) and resin-based unfilled (Clinpro) sealant
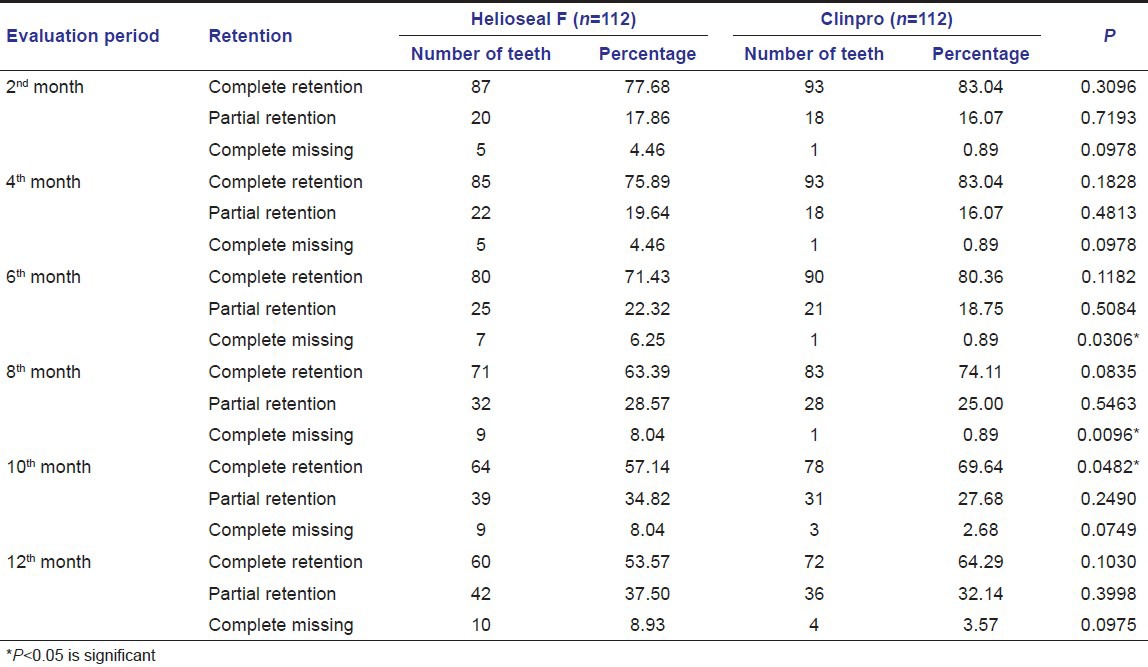
Figure 1.

Comparison of the retention of resin-based filled (Helioseal F) and resin-based unfilled (Clinpro) sealant
Comparison of the retention of resin-based filled (Helioseal F) and resin-based unfilled (Clinpro) sealant between upper and lower teeth
At the final month evaluation of the retention of resin-based filled (Helioseal F) and resin-based unfilled (Clinpro) sealant between the upper and lower teeth, 42.86% (24 teeth) showed complete retention on upper teeth and 64.29% (36 teeth) on lower teeth. About 44.64% (25 teeth) showed partial retention on upper teeth and 30.36% (17 teeth) on lower teeth. About 12.50% (7 teeth) showed complete missing on upper teeth and 5.36% (3 teeth) on lower teeth in filled resin-based sealant and 58.93% (33 teeth) showed complete retention on upper teeth and 69.64% (39 teeth) on lower teeth. About 37.5% (21 teeth) showed partial retention on upper teeth and 26.79% (15 teeth) on lower teeth. About 3.57% (2 teeth) showed complete missing on upper teeth and 3.57% (2 teeth) on lower teeth in unfilled resin-based sealant. There was no statistically significant difference.
Discussion
Caries occurrence in the pits and fissures of the occlusal surface of molars is responsible for about 67–90% of caries in children from 5 to 17 years of age. Caries frequently occurs on these surfaces, and progression of the lesion can occur quite rapidly because the pits and fissures predispose occlusal surfaces to decay.[9]
Sealants have been developed to protect the pits and fissures from caries by preventing the impaction of food and bacteria, which produce acidic conditions that result in caries initiation. These pit and fissure sealants are largely accepted as effective noninvasive treatment to prevent or arrest occlusal caries. The efficacy of sealants in preventing caries has been associated with the duration and degree of sealant retention.[5,10] The retention rate becomes a major point of concern when a study tests the clinical performance of a fissure sealant material.
Mechanical retention of sealants is the direct result of resin penetration into pits and fissures and porous etched enamel surface forming micromechanical tags,[10] where the viscosity of the sealant plays an important role in penetrating and forming micromechanical tags for their retention on the etched surface.[11] Resin sealants that possess both low viscosity and excellent wetting properties have been recommended for dental use.[12] Over a period sealants undergo abrasive wear and hence filler particles have been added to sealants to increase their wear and abrasion resistance. Addition of filler particles lowers the sealant's ability to penetrate into fissures and microporosities of etched enamel.[11] As there were less clinical studies comparing the retention rate of resin-based filled and unfilled fluoride releasing pit and fissure sealants, the present study was conducted to evaluate and compare the retention ability of commercially available Helioseal F (filled) and Clinpro (unfilled) resin-based pit and fissure sealants.
Following the split-mouth design, this study used Helioseal F (filled) and Clinpro (unfilled) resin-based pit and fissure sealants. This design was undertaken in which both sealant materials were to be applied in the same mouth on contralateral teeth to directly compare the material performance under similar environmental conditions. Also, before application of sealants all the teeth were pretreated by prophylaxis with pumice slurry using bristle-brush in a slow speed hand piece.
The successful bonding of resin sealant to enamel is dependent on adequate and proper conditioning of enamel. In the present study, 37% phosphoric acid gel (3M ESPE) was used with an etching time of 45 s. Etching roughens the tooth surface and produces a honeycomb-like structure so that tags of sealant can penetrate deeply into the enamel and form an effective mechanical bond, thus retaining the sealant.[4]
During the application procedure according to the manufacturer's instructions, both materials were able to place easily using syringe and needle tips. Comparatively clinpro sealant had very less air bubbles inclusion during application, and the pink color of the sealant made the visualization better to apply the sealant on all the pits and fissures easily when compared to Helioseal F. All the air bubbles were removed using sharp explorer by manipulating the material in pits and fissures and ensured that all the air bubbles were removed and light-cured for 20 s.
Various authors have used different criteria to assess sealant retention. The use of varying criteria with lack of clear definitions led us to select Simonsen's criteria for evaluation of sealant retention, which are relatively simple to follow.[8] In most of the studies, evaluation of the sealant was done at 3rd, 6th, 9th and 12th month[13] or at 3rd, 6th, and 12th month,[9] or at 6th and 12th month[14] or at 12th month[7,15] during 1-year follow-up period. In this study, sealants were evaluated for retention at 2nd, 4th, 6th, 8th, 10th and 12th month to ensure the complete retention of the sealant at short regular intervals and provide the necessary treatment if required.
At the final month evaluation, the results showed that there was no statistically significant difference in complete retention, partial retention, or complete missing (P > 0.05) between resin-based filled and unfilled pit and fissure sealants. This result was in accordance with other similar studies done.[7,14] The resin-based unfilled pit and fissure sealant (Clinpro) clinically performed better when compared to resin-based filled pit and fissure sealant (Helioseal F). And partial retention of sealants was 37.50% (42 teeth) and 32.14% (36 teeth) in resin-based filled and unfilled pit and fissure sealants respectively, which is better when compared to other studies.[7,15] Wendt-LK and Koch G, had an opinion that if some part of the sealant is missing in the fissures there is still enough material in the deeper part to prevent caries.[16] Complete missing of the sealant was only 8.93% and 3.57% in resin-based filled and unfilled pit and fissure sealants respectively, these results were similar to the other studies.[9]
The study done by McCourt found that sealants without filler provided greater penetration into enamel, especially into fissures than sealants incorporating a microfiller.[17] Rock et al. were of the same opinion in the evaluation of retention capacities of sealants with and without filler, the sealants without filler showed significantly better results after 3 years.[18] However, other authors have not found significant differences in either retention or bond strength between sealants with and without filler and have reported that both penetrate into fissures equally well.[19] A previous study showed that even if acid etching gels or solutions were scraped into the fissures with an explorer tine, the gels, solutions or sealants did not penetrate beyond the region of fissure constriction.[20] This may explain the reason why there was no statistically significant difference in retention rates between resin-based filled and unfilled pit and fissure sealant, which shows that neither fissure sealant showed complete penetration into constricted fissures.
In the present study, the resin-based filled pit and fissure sealant (Helioseal F) showed 53.57% complete retention, 37.50% partial retention and 8.93% complete missing of sealant at 12th month evaluation. The results were slightly better than in a study conducted by Ganss et al.,[15] where only 42.3% of sealant was completely retained by 1-year and in another study done by Bargale and Raj showed only 36.9% of complete retention of sealant after 1-year.[21]
In our study, resin based unfilled pit and fissure sealant (Clinpro) showed 64.29% complete retention, 32.14% of partial retention and 3.57% of complete missing sealant at 12th month follow-up, which showed very good results than in the study done by Dharand Chen[22] where only 24% of the sealant was completely retained by 1-year.
In the previous studies, various other resin based filled sealants (55–98.5%) and unfilled sealants (70–100%) had shown good results with complete retention of sealant by the end of 1-year.[7,14,15] The criteria for patient/tooth selection, the isolation technique used, the operative technique, the choice of materials and the clinical performance evaluation methods used have possibly been associated with the variation in results found among studies.
The retention rate in this study is low when compared to other studies,[7,23] where rubber dam isolation was used. In our study, we did not use rubber dam isolation as we wanted to assess the retention of the sealants using the techniques that would be adopted in community programs.
In our study, retention on the maxillary teeth with both resin-based filled and unfilled pit and fissure sealants was less when compared to mandibular teeth as reported in other studies. The superior retention in mandibular teeth could be because of direct vision, gravity-aided flow of the sealant and well-defined pits and fissures.[24,25] Also, the effect of occlusal stress on the sealant of the maxillary molar appeared at an earlier stage of eruption compared with that of the mandibular molar. The decrease in retention rates found in 8–9-year-old children may be related to the occlusal stress that occurs during eruption. In the earlier stages of mandibular eruption, the maxillary teeth contact only mandibular cusps, not yet reaching the sealant.[13]
After 1-year evaluation, the teeth sealed with resin-based filled and unfilled pit and fissure sealants were found to be completely caries-free in our study. This could be due to the fluoride releasing properties of both the sealants. The fluoride is known to have antibacterial activity by means of inhibition of the biosynthetic metabolism of bacteria. The addition of fluoride to pit and fissure sealant has been applied widely in commercial materials and in research. Fluoride released from dental restorative materials affects caries formation by reducing the demineralization, enhancing remineralization, interfering with plaque formation and inhibiting microbial metabolism.[26]
Dental sealants are a proven tool in caries prevention.[4] Whether the prevention of caries is due to obturation of the fissures, or to the local presence of fluoride, or to both modes of action, it would appear that long-term retention of sealants is a prerequisite for caries prevention. A satisfactory goal might be to seal the pits and fissures of the teeth for the first few years after eruption when the risk of caries attack is highest.[13]
It is important to target sealants on the most susceptible surfaces of the most the susceptible teeth. A complication of this philosophy is that these teeth and surfaces are often the most difficult to successfully seal, leading to high rates of failure.[27] Sealant success is positively associated with eruption status of teeth because the more fully erupted a tooth is, the greater the ability to maintain a dry field. However, sealing of the teeth should be done as soon as it erupts into the oral cavity and reapplication of the sealant should be done as soon as the sealant is lost completely to prevent further treatment necessity.
Conclusion
The study concluded that there was no statistically significant difference in the retention rates between resin-based filled (Helioseal F, Ivoclar Vivadent) and unfilled (Clinpro, 3M ESPE) pit and fissure sealants, but the retention rates of resin-based unfilled (Clinpro) pit and fissure sealant was slightly higher and clinically shown better performance than resin-based filled (Helioseal F) pit and fissure sealant. The retention of sealant on mandibular teeth was seen to be superior to that on maxillary teeth in both resin-based filled pit and fissure sealant.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Taylor CL, Gwinnett AJ. A study of the penetration of sealants into pits and fissures. J Am Dent Assoc. 1973;87:1181–8. doi: 10.14219/jada.archive.1973.0601. [DOI] [PubMed] [Google Scholar]
- 2.Ripa LW. Occlusal sealants: Rationale and review of clinical trials. Int Dent J. 1980;30:127–39. [PubMed] [Google Scholar]
- 3.Simonsen RJ. Pit and fissure sealant: Review of the literature. Pediatr Dent. 2002;24:393–414. [PubMed] [Google Scholar]
- 4.Waggoner WF, Siegal M. Pit and fissure sealant application: Updating the technique. J Am Dent Assoc. 1996;127:351–61. doi: 10.14219/jada.archive.1996.0205. [DOI] [PubMed] [Google Scholar]
- 5.Droz D, Schiele MJ, Panighi MM. Penetration and microleakage of dental sealants in artificial fissures. J Dent Child (Chic) 2004;71:41–4. [PubMed] [Google Scholar]
- 6.Eliades A, Birpou E, Eliades T, Eliades G. Self-adhesive restoratives as pit and fissure sealants: A comparative laboratory study. Dent Mater. 2013;29:752–62. doi: 10.1016/j.dental.2013.04.005. [DOI] [PubMed] [Google Scholar]
- 7.Koch MJ, García-Godoy F, Mayer T, Staehle HJ. Clinical evaluation of Helioseal F fissure sealant. Clin Oral Investig. 1997;1:199–202. doi: 10.1007/s007840050034. [DOI] [PubMed] [Google Scholar]
- 8.Simonsen RJ. Retention and effectiveness of dental sealant after 15 years. J Am Dent Assoc. 1991;122:34–42. doi: 10.14219/jada.archive.1991.0289. [DOI] [PubMed] [Google Scholar]
- 9.Wendt LK, Koch G, Birkhed D. On the retention and effectiveness of fissure sealant in permanent molars after 15-20 years: A cohort study. Community Dent Oral Epidemiol. 2001;29:302–7. doi: 10.1034/j.1600-0528.2001.290410.x. [DOI] [PubMed] [Google Scholar]
- 10.Garcia-Godoy F, Gwinnett AJ. An SEM study of fissure surfaces conditioned with a scraping technique. Clin Prev Dent. 1987;9:9–13. [PubMed] [Google Scholar]
- 11.Subramaniam P, Babu KL, Naveen HK. Effect of tooth preparation on sealant success – An in vitro study. J Clin Pediatr Dent. 2009;33:325–31. [PubMed] [Google Scholar]
- 12.Irinoda Y, Matsumura Y, Kito H, Nakano T, Toyama T, Nakagaki H, et al. Effect of sealant viscosity on the penetration of resin into etched human enamel. Oper Dent. 2000;25:274–82. [PubMed] [Google Scholar]
- 13.Subramaniam P, Konde S, Mandanna DK. Retention of a resin-based sealant and a glass ionomer used as a fissure sealant: A comparative clinical study. J Indian Soc Pedod Prev Dent. 2008;26:114–20. doi: 10.4103/0970-4388.43192. [DOI] [PubMed] [Google Scholar]
- 14.Charbeneau GT, Dennison JB, Ryge G. A filled pit and fissure sealant: 18-month results. J Am Dent Assoc. 1977;95:299–306. doi: 10.14219/jada.archive.1977.0476. [DOI] [PubMed] [Google Scholar]
- 15.Ganss C, Klimek J, Gleim A. One year clinical evaluation of the retention and quality of two fluoride releasing sealants. Clin Oral Investig. 1999;3:188–93. doi: 10.1007/s007840050100. [DOI] [PubMed] [Google Scholar]
- 16.Wendt LK, Koch G. Fissure sealant in permanent first molars after 10 years. Swed Dent J. 1988;12:181–5. [PubMed] [Google Scholar]
- 17.McCourt JW, Eick JD. Penetration of fissure sealants into contraction gaps of bulk packed auto-cured composite resin. J Pedod. 1988;12:167–75. [PubMed] [Google Scholar]
- 18.Rock WP, Weatherill S, Anderson RJ. Retention of three fissure sealant resins. The effects of etching agent and curing method. Results over 3 years. Br Dent J. 1990;168:323–5. doi: 10.1038/sj.bdj.4807185. [DOI] [PubMed] [Google Scholar]
- 19.Sveen OB, Jensen OE. Two-year clinical evaluation of Delton and Prisma-Shield. Clin Prev Dent. 1986;8:9–11. [PubMed] [Google Scholar]
- 20.Garcia-Godoy F, Gwinnett AJ. Penetration of acid solution and gel in occlusal fissures. J Am Dent Assoc. 1987;114:809–10. doi: 10.14219/jada.archive.1987.0164. [DOI] [PubMed] [Google Scholar]
- 21.Bargale S, Raju OS. The retention of glass ionomer and light cure resin pit and fissure sealant using replica technique – An in vivo study. Internet J Dent Sci. 2011;9:37–41. [Google Scholar]
- 22.Dhar V, Chen H. Evaluation of resin based and glass ionomer based sealants placed with or without tooth preparation – A two year clinical trial. Pediatr Dent. 2012;34:46–50. [PubMed] [Google Scholar]
- 23.Simonsen RJ. The clinical effectiveness of a colored pit and fissure sealant at 36 months. J Am Dent Assoc. 1981;102:323–7. doi: 10.14219/jada.archive.1981.0051. [DOI] [PubMed] [Google Scholar]
- 24.Erdemir U, Sancakli HS, Yaman BC, Ozel S, Yucel T, Yildiz E. Clinical comparison of a flowable composite and fissure sealant: A 24-month split-mouth, randomized, and controlled study. J Dent. 2014;42:149–57. doi: 10.1016/j.jdent.2013.11.015. [DOI] [PubMed] [Google Scholar]
- 25.Ninawe N, Ullal NA, Khandelwal V. A 1-year clinical evaluation of fissure sealants on permanent first molars. Contemp Clin Dent. 2012;3:54–9. doi: 10.4103/0976-237X.94547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Li F, Li F, Wu D, Ma S, Gao J, Li Y, et al. The effect of an antibacterial monomer on the antibacterial activity and mechanical properties of a pit-and-fissure sealant. J Am Dent Assoc. 2011;142:184–93. doi: 10.14219/jada.archive.2011.0062. [DOI] [PubMed] [Google Scholar]
- 27.Feigal RJ. Sealants and preventive restorations: Review of effectiveness and clinical changes for improvement. Pediatr Dent. 1998;20:85–92. [PubMed] [Google Scholar]