

Abstract
A 65-year-old male suffering from acute spinal cord injury leading to incomplete tetraplegia presented with severe recurrent Clostridium difficile (C. difficile) infection subsequent to antibiotic treatment for pneumonia. After a history of ineffective antimicrobial therapies, including metronidazole, vancomycin, fidaxomicin, rifaximin and tigecycline, leading to several relapses, the patient underwent colonoscopic fecal microbiota transplantation from his healthy son. Four days subsequent to the procedure, the patient showed a systemic inflammation response syndrome. Without detecting an infectious cause, the patient received antimicrobial treatment, including tigecycline, metronidazole, vancomycin via polyethylene glycol and an additional enema for a period of seven days, leading to a prompt recovery and no reported C. difficile infection relapse during a 12 wk follow up.
Keywords: Clostridium difficile infection, Spinal cord injury, Fecal microbiota transplantation, Systemic inflammatory response syndrome
Core tip: A 65-year-old male suffering from incomplete tetraplegia presented with severe recurrent Clostridium difficile (C. difficile) infection subsequent to antibiotic treatment of pneumonia. After several antimicrobial therapies with subsequent relapses, the patient underwent colonoscopic fecal microbiota transplantation from his healthy son. Four days later, the patient showed a systemic inflammation response syndrome. Without detecting an infectious cause, the patient received antimicrobial treatment, including tigecycline, metronidazole, vancomycin via polyethylene glycol and an additional enema, for a period of seven days, leading to prompt recovery and no reported C. difficile infection relapse during a 12 wk follow up.
INTRODUCTION
The recurrence rate of Clostridium difficile (C. difficile) infections (CDI) after adequate antibiotic treatment remains high and is even more frequent in patients who once relapsed[1]. Data analysis of CDI in spinal cord injured (SCI) patients is insufficient but recurrence rates seem to be equivalent to the non-SCI population[2]. A recent systematic review provides evidence that fecal microbiota transfer (FMT) seems to be a useful adjunct in the treatment of CDI relapses[3]. Out of 536 patients enrolled and treated with FMT, 467 (87%) succeeded in showing no further symptoms. However, success rates vary depending on the site of administration: 81% (stomach); 86% (duodenum and jejunum); 93% (cecum and ascending colon); and 84% for the distal colon. No severe adverse events occurred due to the procedure.
Patients with SCI present with special characteristics in the course of gastrointestinal diseases[4-6] and therefore the management and treatment is challenging[7,8]. For example, impaired colonic motility leads to decreased large bowel transport, frequently leading to constipation or megacolon[9,10]. Furthermore, high level tetraplegic patients (C4 or higher), with more frequent administration of antibiotics due to permanent or intermittent dependency on assisted ventilation following ventilator associated pneumonia, are more susceptible to colonization with multi resistant bacteria or C. difficile infections[11].
Yet, no special protocols for the treatment of CDI in tetraplegic patients have been published, so general regimens are applied. Until now, no FMT procedure in SCI patients has been described in the available literature.
CASE REPORT
A 65-year-old male was admitted to our hospital after ventral spondylodesis of C3 to C5 due to traumatic fracture. However, high level incomplete tetraplegia (American Spinal Injury Association impairment scale C) persisted so that intermittent mechanical ventilation via tracheostoma and enteral feeding via gastric tube [polyethylene glycol (PEG)] became necessary. After several weeks of intensive care treatment, transfer to a general ward was possible. The patient received antibiotic treatment (co-trimoxazole and imipenem) because of a ventilator-associated pneumonia. As a consequence of this, 10 wk post trauma, he presented with watery diarrhea. An Elisa immunoassay detected C. difficile toxin A and B and polymerase chain reaction as a nucleic acid amplification method distinguished C. difficile ribotype 027.
Several therapeutic protocols including metronidazole, vancomycin, fidaxomicin, rifaximin and tigecycline in different forms of applications and combinations were administered (Table 1). Treatment was initiated with vancomycin via PEG 250 mg 4 times a day and via clyster. Metronidazole was added via PEG 400 mg 3 times a day. No vancomycin tapering was done. Fidaxomicin was given using 200 mg via PEG two times a day for 10 d. Due to the next relapse, the patient was treated with rifaximin 400 mg three times a day via PEG for 2 wk. After the next relapse, he was treated with tigecycline intravenously for 10 d combined with vancomycin 2 g via clyster.
Table 1.
Antibiotic treatment prior to fecal microbiota transfer procedure
| Episode | Antibiotic regimen | Dose | Administration route | Length |
| 1 | Vancomycin | 4 times/250 mg | PEG | 10 d |
| Vancomycin | 2 times/2 g | Enema | 10 d | |
| Metronidazole | 3 times/400 mg | PEG | 10 d | |
| 2 | Fidaxomicin | 2 times/200 mg | PEG | 10 d |
| 3 | Rifaximin | 3 times/400 mg | PEG | 10 d |
| 4 | Tigecycline | 1 time/50 mg | iv | 10 d |
| 5 | Rifaximin | 3 times/400 mg | PEG | 14 d |
| 6 | Tigecycline | 1 time/50 mg | iv | 7 d |
| Vancomycin | 2 times/2 g | Enema | 7 d | |
| Rifaximin | 3 times/400 mg | PEG | 10 d | |
| 7 | FMT-procedure | |||
PEG: Polyethylene glycol; FMT: Fecal microbiota transfer.
None of the above succeeded in resolving the symptoms. A total of six relapses occurred, four of which were confirmed by toxin testing in a stool sample. Two episodes without microbiological proof were highly probable by clinical evaluation. Two of the recurrences matched the criteria of severe CDI.
After the sixth treatment failure and renewed cultural proof of CDI, we decided to transfer fecal microbiota. The son, as a healthy first degree relative, gave informed consent for FMT. He reported no antibiotic treatment in the last three months prior to the procedure. Additional testing for infectious diseases (anti-hepatitis A virus, anti-hepatitis B core, hepatitis B surface antigen, anti-hepatitis C virus, human immunodeficiency virus, cytomegalovirus, Epstein-Barr virus, Treponema pallidum) in the serum and C. difficile toxins A and B, campylobacter spp., Shigella, salmonella, Yersinia, pathogenic Escherichia coli, Adeno-, Rota- and Norovirus, parasites, Cryptosporidium/Microsporidium in three independent fecal samples were negative.
In order to prepare the patient for the FMT procedure, we omitted antibiotic treatment over a period of one week and bowel lavage and enema was performed on the 7th day. Fresh donor stool was immediately transferred to the laboratory in an airtight container. A portion of 160 g was weighed and homogenized with isotonic sodium chloride in a sterile flask. Afterwards, the homogenate was filtered repeatedly through a sterile gauze pad to remove as much particulate matter as possible[12]. The finished stool slurry was immediately transferred to the endoscopy unit and administered into the terminal ileum and colon during colonoscopy. The endoscopic findings showed severe pseudomembranous colitis with destruction of large areas of the colonic surface (see Figure 1).
Figure 1.
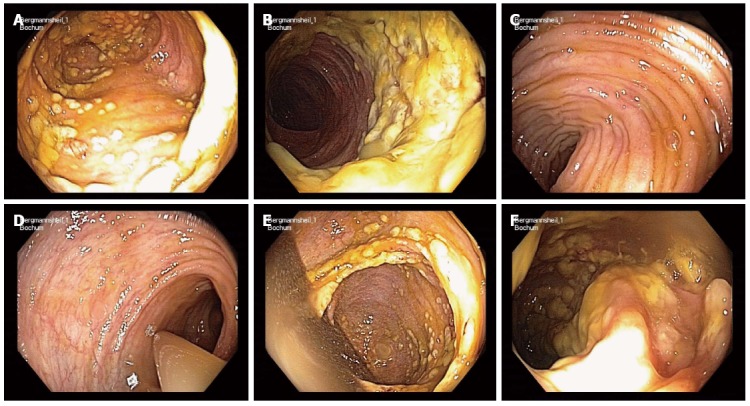
Endoscopic appearance during colonoscopic fecal microbiota transfer procedure. A, B: Severe pseudomembranous colitis in the colon after antibiotic treatment and bowel lavage; C: Terminal ileum without endoscopic changes; D: Instillation of fecal transplant; E, F: Fecal transplant in pseudomembranous colitis areas.
Four days subsequent to the FMT, the patient experienced fever as part of a severe systemic inflammatory response syndrome with shock. Stool consistency was pulpy but not watery as seen before. Due to respiratory failure and vasoplegia which required immediate mechanical ventilation and high-dose vasopressor therapy, the patient was transferred from the intermediate care to the intensive care unit. Extensive work-up did not reveal any infectious cause. Whole body CT scan did not show a focus despite the persistent colitis, especially no signs of pneumonia, empyema or soft tissue infection. Microbiological testing did not detect C. difficile in the stool sample and blood and urine cultures did not detect any bacteria or mycosis. There was no sign of catheter-associated blood stream infection. Echocardiographic examination did not show endocarditis.
We initiated calculated intravenous antibiotic therapy, including tigecycline and metronidazole as well as vancomycin via PEG and an enema, for a period of seven days. The respiratory and cardiovascular situation improved shortly after initiation of the treatment. In the following weeks, the patient did not receive any further antibiotic therapy. Weaning from ventilation was successful within the next weeks, enabling transfer of the patient to a specialized rehabilitation clinic. No recurrence of watery diarrhea or CDI-like symptoms occurred in the following twelve weeks subsequent to the FMT procedure.
DISCUSSION
Only very few adverse events associated with FMT have been described in the available literature so far, focussing on general population[13]. In more than 200 fecal transplantation procedures at the Academic Medical Centre of Amsterdam, The Netherlands, and more than 3000 at the Centre for Digestive Diseases in Sydney, Australia, no serious adverse event have been reported. Most patients treated with FMT experienced diarrhea on the day of the procedure and only a minority of the patients reported belching, abdominal cramping or constipation. These observations coincide with published case reports and series of FMT for CDI[14,15]; adverse events were reported for only 3 of 317 patients (upper gastrointestinal tract bleeding, peritonitis or enteritis). In another case report, nasoduodenal FMT for Crohn’s disease resulted in transient adverse effects, such as fever and abdominal tenderness in three out of four patients. However, the symptoms were temporary and ceased spontaneously in the following two days post FMT[16]. A case report by Borody et al[17], in which FMT was administered during colonoscopy, does not describe any side effects due to the procedure. Substantially, long-term follow up studies state FMT as a safe and feasible procedure without major adverse events[18].
Due to impaired bowel function, among other characteristics, patients with spinal cord injury are a challenging population. In particular, CDI in SCI-patients seems to take a more severe clinical course[19]. Furthermore, bowel preparation as the initial step of FMT is less effective[8], which may lead to deterioration of the FMT outcome.
This case emphasizes that FMT is feasible and effective in the treatment of CDI in tetraplegic patients; however, possible adverse and even severe adverse events have to be taken into consideration. In a population of ninety-nine immunosuppressed patients, severe adverse events occurred in 15% of the patients, including one procedure-associated and one non procedure-associated death[20]. Astonishingly, infection has not been the leading problem. Although our patient showed symptoms of systemic inflammation response syndrome, an infectious cause was not identified during the extensive diagnostic work-up. We hypothesize that some bacteria, possibly C. difficile, might have passed the severely destroyed mucosal layer during colonoscopy of the insufficiently prepared large bowel. The assumed transient bacteremia may be avoidable by performing FMT using a nasojejunal tube.
Although the cause remained uncertain, the treatment for septic CDI using metronidazole, vancomycin and tigecycline was initiated. With the absence of diarrhea 12 wk after the FMT procedure, the enterocolitis is considered to be in remission, emphasizing that antibiotic treatment after FMT did not lead to a relapse of CDI in the sense of the international definition[21,22].
To our knowledge, this is the first case reporting successful fecal microbiota transfer in a SCI-patient with recurrent CDI. Severe adverse events, although rarely described in literature, have to be considered subsequent to FMT, especially in patients with further impairments of bowel function. In cases of tetraplegic patients, oral administration of the stool suspension might be more feasible than through a colonoscope due to the impaired bowel cleansing prior to the procedure and therefore a higher microbial load. However, antibiotic treatment after FMT does not necessarily deteriorate the outcome of fecal microbiota transplantation.
COMMENTS
Case characteristics
A patient with acute spinal cord injury leading to incomplete tetraplegia developed recurrent diarrhea after antibiotic treatment of ventilator associated pneumonia.
Clinical diagnosis
Relapsing Clostridium difficile (C. difficile) infection (CDI) was likely.
Differential diagnosis
After several regimens to treat CDI, fecal microbiota transplantation (FMT) was planned and undertaken.
Laboratory diagnosis
An ELISA detected C. difficile toxins A and B, polymerase chain reaction proved C. difficile ribotype 027.
Imaging diagnosis
Colonoscopy during FMT showed pseudomembranous colitis, a computed tomography scan four days later revealed severe colitis; all other examinations did not show pathological signs.
Treatment
Relapsing CDI was treated by FMT, which four days later resulted in a systemic inflammatory response syndrome (SIRS); subsequent treatment with tigecycline, rifaximin and vancomycin led to prompt complete recovery.
Related reports
There is an increasing interest in the literature in FMT but descriptions of complications are scarce. Furthermore, several special groups of patients have been treated with FMT but no tetraplegic patient with functional abnormalities of the gastrointestinal and colonic tract has been described so far.
Experiences and lessons
The authors report the first case of FMT in a tetraplegic patient and describe a possible, procedure related serious adverse event.
Peer-review
This is an interesting case report of CDD treated with FMT in a patient with acute spinal cord injury who had been previously treated with antibiotics. The paper is well written and the case is interesting and potentially useful for readers.
Footnotes
Ethics approval: This retrospective case report has not been discussed with the institutional review board.
Informed consent: The manuscript has been prepared anonymously with informed consent of the patient and his son.
Conflict-of-interest: The authors declare they have no conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: August 25, 2014
First decision: October 29, 2014
Article in press: January 16, 2015
P- Reviewer: Burdette SD, Gea-Banacloche J, Rodriguez D S- Editor: Ma YJ L- Editor: Roemmele A E- Editor: Wang CH
References
- 1.McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol. 2002;97:1769–1775. doi: 10.1111/j.1572-0241.2002.05839.x. [DOI] [PubMed] [Google Scholar]
- 2.Ramanathan S, Johnson S, Burns SP, Kralovic SM, Goldstein B, Smith B, Gerding DN, Evans CT. Recurrence of Clostridium difficile infection among veterans with spinal cord injury and disorder. Am J Infect Control. 2014;42:168–173. doi: 10.1016/j.ajic.2013.08.009. [DOI] [PubMed] [Google Scholar]
- 3.Cammarota G, Ianiro G, Gasbarrini A. Fecal microbiota transplantation for the treatment of Clostridium difficile infection: a systematic review. J Clin Gastroenterol. 2014;48:693–702. doi: 10.1097/MCG.0000000000000046. [DOI] [PubMed] [Google Scholar]
- 4.Longo WE, Ballantyne GH, Modlin IM. Colorectal disease in spinal cord patients. An occult diagnosis. Dis Colon Rectum. 1990;33:131–134. doi: 10.1007/BF02055542. [DOI] [PubMed] [Google Scholar]
- 5.Glickman S, Kamm MA. Bowel dysfunction in spinal-cord-injury patients. Lancet. 1996;347:1651–1653. doi: 10.1016/s0140-6736(96)91487-7. [DOI] [PubMed] [Google Scholar]
- 6.Stone JM, Nino-Murcia M, Wolfe VA, Perkash I. Chronic gastrointestinal problems in spinal cord injury patients: a prospective analysis. Am J Gastroenterol. 1990;85:1114–1119. [PubMed] [Google Scholar]
- 7.Hayman AV, Guihan M, Fisher MJ, Murphy D, Anaya BC, Parachuri R, Rogers TJ, Bentrem DJ. Colonoscopy is high yield in spinal cord injury. J Spinal Cord Med. 2013;36:436–442. doi: 10.1179/2045772313Y.0000000091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ancha HR, Spungen AM, Bauman WA, Rosman AS, Shaw S, Hunt KK, Post JB, Galea M, Korsten MA. Clinical trial: the efficacy and safety of routine bowel cleansing agents for elective colonoscopy in persons with spinal cord injury - a randomized prospective single-blind study. Aliment Pharmacol Ther. 2009;30:1110–1117. doi: 10.1111/j.1365-2036.2009.04147.x. [DOI] [PubMed] [Google Scholar]
- 9.Fajardo NR, Pasiliao RV, Modeste-Duncan R, Creasey G, Bauman WA, Korsten MA. Decreased colonic motility in persons with chronic spinal cord injury. Am J Gastroenterol. 2003;98:128–134. doi: 10.1111/j.1572-0241.2003.07157.x. [DOI] [PubMed] [Google Scholar]
- 10.Vallès M, Vidal J, Clavé P, Mearin F. Bowel dysfunction in patients with motor complete spinal cord injury: clinical, neurological, and pathophysiological associations. Am J Gastroenterol. 2006;101:2290–2299. doi: 10.1111/j.1572-0241.2006.00729.x. [DOI] [PubMed] [Google Scholar]
- 11.Dumford DM, Nerandzic M, Chang S, Richmond MA, Donskey C. Epidemiology of clostridium difficile and vancomycin-resistant Enterococcus colonization in patients on a spinal cord injury unit. J Spinal Cord Med. 2011;34:22–27. doi: 10.1179/107902610x12883422813822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kleger A, Schnell J, Essig A, Wagner M, Bommer M, Seufferlein T, Härter G. Fecal transplant in refractory Clostridium difficile colitis. Dtsch Arztebl Int. 2013;110:108–115. doi: 10.3238/arztebl.2013.0108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Smits LP, Bouter KE, de Vos WM, Borody TJ, Nieuwdorp M. Therapeutic potential of fecal microbiota transplantation. Gastroenterology. 2013;145:946–953. doi: 10.1053/j.gastro.2013.08.058. [DOI] [PubMed] [Google Scholar]
- 14.Gough E, Shaikh H, Manges AR. Systematic review of intestinal microbiota transplantation (fecal bacteriotherapy) for recurrent Clostridium difficile infection. Clin Infect Dis. 2011;53:994–1002. doi: 10.1093/cid/cir632. [DOI] [PubMed] [Google Scholar]
- 15.Kassam Z, Lee CH, Yuan Y, Hunt RH. Fecal microbiota transplantation for Clostridium difficile infection: systematic review and meta-analysis. Am J Gastroenterol. 2013;108:500–508. doi: 10.1038/ajg.2013.59. [DOI] [PubMed] [Google Scholar]
- 16.Vermeire S, Joossens M, Verbeke K, Hildebrand F, Machiels K, Van den Broeck K, Van Assche G, Rutgeerts PJ, Raes J. Pilot study on the safety and efficacy of faecal microbiota transplantation in refractory Crohn’s disease. Gastroenterology. 2012;142:S360. [Google Scholar]
- 17.Borody TJ, Wettstein AR, Leis S, Hills LA, Campbell J, Torres M. Clostridium difficile complicating inflammatory bowel disease: pre- and post-treatment findings. Gastroenterology. 2008;134:A361. [Google Scholar]
- 18.Brandt LJ, Aroniadis OC, Mellow M, Kanatzar A, Kelly C, Park T, Stollman N, Rohlke F, Surawicz C. Long-term follow-up of colonoscopic fecal microbiota transplant for recurrent Clostridium difficile infection. Am J Gastroenterol. 2012;107:1079–1087. doi: 10.1038/ajg.2012.60. [DOI] [PubMed] [Google Scholar]
- 19.Buchner AM, Sonnenberg A. Epidemiology of Clostridium difficile infection in a large population of hospitalized US military veterans. Dig Dis Sci. 2002;47:201–207. doi: 10.1023/a:1013252528691. [DOI] [PubMed] [Google Scholar]
- 20.Kelly CR, Ihunnah C, Fischer M, Khoruts A, Surawicz C, Afzali A, Aroniadis O, Barto A, Borody T, Giovanelli A, et al. Fecal microbiota transplant for treatment of Clostridium difficile infection in immunocompromised patients. Am J Gastroenterol. 2014;109:1065–1071. doi: 10.1038/ajg.2014.133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Debast SB, Bauer MP, Kuijper EJ. European Society of Clinical Microbiology and Infectious Diseases: update of the treatment guidance document for Clostridium difficile infection. Clin Microbiol Infect. 2014;20 Suppl 2:1–26. doi: 10.1111/1469-0691.12418. [DOI] [PubMed] [Google Scholar]
- 22.Surawicz CM, Brandt LJ, Binion DG, Ananthakrishnan AN, Curry SR, Gilligan PH, McFarland LV, Mellow M, Zuckerbraun BS. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478–98; quiz 499. doi: 10.1038/ajg.2013.4. [DOI] [PubMed] [Google Scholar]