

Abstract
This study presents the results of a meta-analysis of the association between substance use and risky sexual behavior among adolescents. 87 studies fit the inclusion criteria, containing a total of 104 independent effect sizes that incorporated more than 120,000 participants. The overall effect size for the relationship between substance use and risky sexual behavior was in the small to moderate range (r = .22, CI = .18, .26). Further analyses indicated that the effect sizes did not substantially vary across the type of substance use, but did substantially vary across the type of risky sexual behavior being assessed. Specifically, mean effect sizes were smallest for studies examining unprotected sex (r = .15, CI = .10, .20), followed by studies examining number of sexual partners (r = .25, CI = .21, .30), those examining composite measures of risky sexual behavior (r = .38, CI = .27, .48), and those examining sex with an intravenous drug user (r = .53, CI = .45, .60). Furthermore, our results revealed that the relationship between drug use and risky sexual behavior is moderated by several variables, including sex, ethnicity, sexuality, age, sample type, and level of measurement. Implications and future directions are discussed.
Keywords: risky sex, substance use, meta-analysis, study design, youth
1. Introduction
Sexually transmitted infections (STIs) represent one of the most critical public health challenges facing our nation, as there are approximately 19 million new infections within the United States each year, resulting in a yearly cost to our healthcare system of approximately $17 billion (Centers for Disease Control and Prevention [CDC], 2011). Globally, over a million people each day are infected with a STI (World Health Organization [WHO], 2013). The study of adolescents’ sexual behavior has been a mainstay in the infectious diseases literature for over three decades (Martinez, Copen, & Abma, 2011; Sawyer et al., 2012), as adolescents in the United States comprise approximately 50% of all new STI cases (Weinstock, Berman, & Cates, 2004) and 60% of youth worldwide are currently infected with a STI (Da Ros & Schmitt, 2008). Growth in the rates of STIs and associated costs of infection has created a sense of urgency in the need to understand the individual and situational factors that increase one’s risk for infection. One such factor, substance use prior to sexual activity, has been commonly shown to increase the likelihood of unsafe sexual intercourse (e.g., Yan et al., 2007). Though many studies have examined the relationship between risky sexual behavior (RSB) and substance use (SU) within a number of adolescent populations and within a variety of settings, the results of study findings have been mixed (e.g., Bryan, Ray, & Cooper, 2007; Siahann, 2007; Voisin et al., 2007). Therefore, the purpose of the current study is to use meta-analytic techniques to determine the conditions under which the relationship between these two variables is strongest. Specifically, we seek to estimate the average relationship between SU and RSB in adolescents, as well as to understand how the strength of this relationship varies with type of substance use, type of RSB being considered, and sample characteristics.
1.1 Substance use and risky sexual behavior
There is evidence that as many as 22.1% of adolescents engaged in SU during their most recent sexual encounter (e.g., Eaton et al., 2012). Research has shown that, relative to their non-substance using peers, adolescents who regularly abuse substances are more likely to be become sexually active at an earlier age (e.g., Madkour, Farhat, Halpern, Godeau, & Gabhainn, 2010), have more sexual partners (e.g., Connell, Gilreath, & Hansen, 2009), and are more likely to have unprotected sex (e.g., Tucker et al., 2012). Furthermore, SU has been associated with increased risk of STI (e.g., Swartzendruber, Sales, Brown, DiClemente, & Rose, 2013), particularly among juvenile detainees (e.g., Valera, Epperson, Daniels, Ramaswamy, & Freudenberg, 2009).
Although many studies have provided evidence for a relationship between SU and RSB, the findings from studies investigating this relationship have been mixed. Some researchers have found that the two variables are positively related (e.g., Baskin-Sommers & Sommers, 2006; Bryan, Ray, & Cooper, 2007), while others have found no relationship between SU and RSB (e.g., Leigh et al., 2008; Voisin et al., 2007). Several studies have important methodological variations that could have influenced their results, making generalizations difficult (e.g., Ellickson, Collins, Bogart, Klein, & Taylor, 2005). For the purposes of this study, RSB is defined as any behavior that increases one’s likelihood of STI, including having unprotected intercourse, having multiple sexual partners, and having intercourse with an intravenous drug user (IVDU). Substance use, on the other hand, includes the global or frequency of alcohol use and prescription drug abuse, as well as the use of illicit substances such as marijuana, cocaine, opiates, and ecstasy.
1.2 Explanations of the relationship between substance use and risky sex
The perception that SU has a disinhibiting effect on one’s decision to engage in sexual behavior is widely accepted (Yan et al., 2007). Research on neurocognition suggests that these effects may be particularly strong for adolescents. The areas of the brain responsible for the experience of pleasure, emotion, reward, and novelty seeking reach maturity prior to areas of the brain that are associated with behavior regulation and higher-order processing (Riggs & Greenberg, 2009). Researchers have found that the limbic system, which is responsible for emotion control, develops significantly earlier than the frontal cortex, which controls executive functioning, such as decision making (Casey, Getz, & Galvan, 2008). Since the frontal cortex is still developing during adolescence, youth commonly make decisions that are disproportionately influenced by emotion rather than reasoning, increasing the likelihood of engaging in risky behaviors (e.g., Steinberg, 2008). Furthermore, previous research has suggested that type of SU may be differentially associated with certain types of RSB. One study, for example, found that marijuana use, and not alcohol use, was associated with RSB (Kingree & Betz, 2003).
Other theories suggest that the relationship between SU and RSB may not be entirely based in biology. Steele and Josephs (1990) proposed the alcohol myopia theory, suggesting that the disinhibition of behavior is the result of a reduction in the ability to correctly extract meaning from situational cues. Similarly, Hull & Bond (1986) proposed expectancy theory, which suggests that if adolescents expect SU to have a disinhibiting impact on their sexual behavior, they are more likely to engage in risky behaviors that have been attributed to SU, such as unprotected sex.
Some researchers believe that instead of SU leading to RSB, the practice of RSB leads to SU (Cooper, 2006). According to Cooper (2006), when the opportunity for intercourse arises, an individual’s motivations to engage in RSB lead him or her to use substances. Adolescents might also engage in SU because they believe that it has the potential to enhance their sexual experiences (Matthews et al., 2013). Individuals may sometimes attempt to excuse (to oneself and others) their behavior, such as RSB, by attributing it to the effects of SU (Cooper, 2006). Regardless of the individual motivations, reverse causal explanations assume that people strategically use substances because they believe that SU has the potential to facilitate the desired behaviors that lead to the sought after sexual outcome (Hendershot, Magnan, & Bryan, 2010).
Aside from explanations that focus on biological development or influences and individual expectations, research has shown that other factors may further influence the relationship between SU and RSB. Third-variable interpretations, for example, often focus on the characteristics of individuals or contexts that might increase the likelihood of both SU and RSB. Some individual characteristics that might be associated with both SU and RSB would be sensation seeking and impulsivity (Charnigo et al., 2013), and depression (e.g., Shrier et al., 2009). Some contextual factors that might be associated with SU and RSB would be abuse, neglect, parental SU, and peer influences (Cooper, 2006). All third-variable interpretations assume that the covariation between SU and RSB is due to a mediating variable, or the impact of a shared underlying cause.
1.3 Categorical differences between studies
There are several study characteristics that may moderate strength of the relationship between SU and RSB. We divided these into three categories: sample characteristics, measurement factors, and publication characteristics.
1.3.1 Sample characteristics
There is reason to believe that the relationship between SU and RSB may vary by demographic factors, such as sex (Schuster, Mermelstein, & Wakschlag, 2013) and ethnicity (Khan, Berger, Wells, & Cleland, 2012). Sex and ethnic differences often have cultural components that could lead to a significant amount of variability in concurrent participation in SU and RSB (Schwartz et al., 2012). Sex differences in the relationship between SU and RSB may depend on age (SAMSA, 2009). Male and female adolescents (12–17 years old) reported similar rates of alcohol use (14.2% and 15%, respectively), while emerging adult males (18–24 years old) reported significantly more alcohol use (64.3%) than their female peers (58%). We would expect that, as youth get older, sex differences in the relationship between SU and RSB will be more pronounced, with males reporting stronger associations than their female peers. Furthermore, it is possible that there are ethnic differences in the degree of substance use or substance of choice (Substance Abuse and Mental Health Services [SAMSA], 2009). According to data from the 2008 National Household Survey on Drug Abuse (NHSDA), Caucasian, Hispanic, and multiracial adolescents reported the highest rates of current alcohol use (16.3%, 14.8%, and 13.6%, respectively) (SAMSA, 2009). We propose that youth reporting the highest rates of SU may also be more likely to pair SU with RSB.
The setting from which participants are selected is an important factor as well. Voisin et al. (2007) found strong and significant relations between SU and RSB among juvenile detainees. Brown and Vanable (2007), on the other hand, did not find a significant relationship between SU and RSB among youth in community settings. It is possible that juvenile detainees differ significantly from their same-age peers who are not detained with regard to their desire to participate in risky behaviors and the degree to which they would pair illicit SU with RSB. Nationality of the sample could also be a source of variation in the reported relationship between SU and RSB (e.g., Cavazos-Rehg et al., 2011; Kebede et al., 2005). The customs and behavioral expectations of citizens of some countries might make concurrent SU and RSB more or less likely.
1.3.2 Measurement factors
One of the most significant differences between studies of the relationship between these two variables is the variability in the operationalization of both substance use and risky sexual behavior, making comparisons between single studies difficult. The relationship between SU and RSB is often measured in one of three ways: globally, at the situational, or at the event level. In global measurements, researchers assess the overall rates of either SU or RSB. The measure of SU is not restricted to sexual situations. In this case, an individual’s global SU across all situations is considered (see Morrison-Beedy, Carey, Feng, & Tu, 2008). Situational measures, on the other hand, specifically assess the extent to which SU and RSB have occurred during a specific range of time or set of sexual encounters. These studies often relate the proportion of occasions in which SU occurs during/prior to sexual behavior to the proportion of occasions in which the individuals engaged in RSB (see Crosby et al., 2008). Situational measurements are taken at the participant level rather than at the event level. Event-level measures examine the specific pairing of SU and RSBs in individual sexual events to determine if SU and RSB were simultaneous. Event-level measures are distinguishable from situational measures in that event-level measurements of SU and RSB ask participants to identify a particular sexual event (e.g., last time you had intercourse) and ask questions about SU and RSB during that event (see Bryan et al., 2007). We would expect that differences in study design would significantly moderate the relationship between these two variables. Global measures may produce stronger effect sizes, as they tend to be less specific and may have the tendency to overestimate the connection between SU and RSB. Event-level measurements, on the other hand, may produce weaker effects given their specificity, as it is possible the such studies miss key sexual events during which SU was paired with RSB especially if the time frame does not match up with the event. For example, if a youth report did not use substances at their last intercourse, but did a week prior to the most recent sexual event.
1.3.3 Publication characteristics
Publication characteristics include the year of publication and whether the article was published in a peer-reviewed journal. The year of publication is important because study quality might vary with time. For example, newer studies can take advantage of previous research and often make use of empirically-supported methods of assessing the relationship between SU and RSB. It would be important to determine if the improvement of methods over time leads to higher or lower effect size estimates. Similarly, whether the article is published in a peer-reviewed journal might be an important source of variation, as studies with smaller effect sizes are less likely to be published. This could lead to the misperception that the relationship between SU and RSB is stronger than it really is due to publication bias.
1.4 Purpose of this study
There have been several recent reviews (e.g., Griffin, Umstattd, & Usdan, 2010; Sales, Brown, Vissman, & DiClemente, 2012; Shuper et al., 2010) and meta-analyses (e.g., Baliunas et al., 2010) that have examined the relationship between specific substances (i.e., alcohol consumption) and RSB. Despite the prevalence of reviews examining the SU to RSB relationship for specific substances, to our knowledge, no reviews have explored how the SU to RSB relationship among adolescents and young adults might vary across different substances. Moreover, no studies have meta-analyzed the relationship between more than one of type of SU on RSB. Furthermore, there is a lack of agreement among researchers regarding the nature of the relationship between SU and RSB, as variations in methodological decisions made by researchers have complicated our ability to interpret the results of studies investigating this association. Understanding the proposed association is crucial, as it has the potential to greatly impact the focus of intervention and prevention programs. To address these key concerns, the present study examines both the overall relationship between SU and RSB among adolescents, as well has how this relationship varies across different types of SU, different types of RSB, and the levels of relevant study characteristics.
2. METHOD
2.1 Sample of studies
The purpose of the literature search was to identify studies that investigated the bivariate relationship between SU and RSB. The following review used reporting standards consistent those of Lipsey and Wilson (2001) and PRISMA guidelines, which is a 27-item checklist for the conduct and reporting of systematic reviews and meta-analyses (Moher, Liberati, Tetzlaff, Altman, & The PRISMA Group, 2009). Several electronic databases were searched, including: PsycINFO, Health Source, PubMed, CINAHL, OVID, Sociological Abstracts, PsycARTICLES, PsychiatryOnline.com, and Academic Search Premier. While the lower limit of the date range was not specified, the upper limit end date was August 2008, which is when the meta-analysis was completed. This search strategy identified articles whose titles or abstracts paired terms related to RSB with terms related to SU. Wild card terms, or terms ending in special characters, were used to obtain articles that included variations of the search terms. The search terms (where “*” indicates the use of a wild card) for adolescents were youth*, teen*, adolescen*, young*, and juvenile. For RSB, the terms were AIDS, HIV, STD, risk*, unprotected, protect*, unsafe, safe, condom, sex*, and intercourse. Lastly, SU search terms were drug, substance, alcohol, cocaine, marijuana, heroin, and meth*. In addition to the search terms, a separate set of terms, called exclusion or “not” terms, were included to reduce the number of unrelated articles generated. Exclusion terms included: mouse, mice, rat*, cell*, serum*, elder*, and tissue*.
Articles included peer-reviewed publications, theses, dissertations, and government reports. The Social Science Citation Index was used to locate articles that had cited Leigh and Stall (1993), which was a seminal study in SU and RSB. We examined the references from Pritchard and Cox (2007), Richter, Valois, McKeown, and Vincent (1993), Donenberg, Emerson, Bryant, and King (2006), Donovan and McEwan (1995), Darling, Palmer, and Kipke (2005), Robbins and Bryan (2004), Hallfors et al. (2002), Ramrakha, Caspi, Dickson, Moffitt, and Paul (2000), and Naff Johnson (1996), which were randomly selected from the sample. Finally, we wrote the corresponding authors of the articles identified by these methods to obtain additional work in the area of SU and RSB that may have been missed by our search. The initial search generated 17,223 abstracts, which included duplicates and incomplete references. After the removal of the duplicates and incomplete references, there were 7,996 abstracts.
2.2 Inclusion and exclusion criteria
The next step involved the determination of whether a particular study met the criteria for inclusion in the meta-analysis. The first criterion was that participants were younger than 25 years of age. Many researchers have classified individuals aged 12 thru 24 to be adolescents; however, the range varies significantly. The condition of adolescence is often associated with advanced education, efforts to obtain employment, and find a marriage partner (Dehne & Riedner, 2001). Since the average age of marriage in much of the western world is close to 25 years of age, many researchers have selected this age as the cut-off for adolescence (Dehne & Riedner, 2001).
Additional criteria were as follows:
The study included measures of SU and RSB on the same participants.
There was sufficient information to compute an effect size for the relationship between SU and RSB.
Due to limitations of the research team, the article must have been written in English.
As we were interested in typical adolescents, studies focused on participants classified as prostitutes or sex workers were excluded.
The authors had written a document, manuscript, or report describing the study.
Sexual risk was not the result of a rape or sexual assault.
The titles and abstracts of identified articles were examined by two of the coauthors to create a reduced candidate list of 638 articles. This list removed articles that clearly did not contain data relevant to the meta-analysis, but retained any that might possibly be relevant. The full text of the 638 articles was examined, finally locating 87 that fit the inclusion criteria and which reported enough data to compute an effect size for the relationship between SU and RSB. These studies included 104 independent effect sizes, incorporating more than 120,000 participants.
2.3 Coding of moderators
Studies were coded based on the following moderator variables: Sample characteristics included type of sample (e.g., clinical, community, or juvenile), nationality, mean age, racial composition, and sex composition. Measurement factors included type of SU (e.g., alcohol, marijuana, hard drugs), method of assessment (e.g., self-report, interview, other), operational definitions of RSB (e.g., unprotected sex, number of partners, etc.), SU (e.g., frequency/quantity, dichotomization of use, clinical diagnosis), and level of measurement for SU and RSB (i.e., global, situational, or event analyses). Finally, publication characteristics included publication year and publication type (e.g., peer-reviewed journal, dissertation, etc.).
2.4 Reliability
For each study, two different raters (selected from authors TDR, HF, and MS) independently coded the moderating variables and calculated the effect sizes. Inter-rater reliability was computed using Cohen’s kappa for categorical variables (Cohen, 1960) and intraclass correlations for continuous variables (ICC; Fleiss & Cohen, 1973). Cohen’s kappa is a measure of “true” agreement, representing the agreement between coders that is achieved beyond that which is expected based on chance when all disagreements between coders are treated equally. The ICC is a measure of the consistency of ratings between coders evaluating the same study. In other words, it is the proportion of variance that is associated with differences among studies and describes the degree to which codes from the same study resemble each other. A kappa or ICC of at least 0.80 was considered acceptable. Reliability estimates ranged from 0.85 to 1.00, with a median of 0.97. Discrepancies between coders were resolved through discussions with the research team.
2.5 Computation of effect sizes
We chose to use Pearson’s r as our effect size measure to due to its ability to account for variations in metrics used in measurement and because much of the research on this relationship utilizes correlation coefficients. We found that the majority of studies that examined this topic did not report enough information to compute Cohen’s d or Hedge’s g, as means and standard deviations are often omitted from studies in which the relationship between SU and RSB was not the primary focus of the investigation. Effect sizes were computed using Comprehensive Meta-Analysis (CMA) version 2.2 (Borenstein, Hedges, Higgins, & Rothstein, 2006) and DSTAT version 1.10 (Johnson, 1993). For studies that did not directly report correlations, we derived the effect size from other statistics such as means and standard deviations, regression coefficients, t, F, and p values. If such information was not provided, the study was excluded from the sample. When studies included multiple measures of SU or RSB, individual effect sizes were calculated for the different measures. For example, if a study reported the use of both alcohol and marijuana, separate effect sizes were calculated representing the relations of each of these measures with RSB. To control for dependence and reduce the number of effect sizes contributed to the calculation of the overall effect size, we averaged the effect sizes from studies reporting more than one effect size. The final sample consisted of 87 studies.
2.6 Analytic procedures
When performing a meta-analysis, researchers can choose to use fixed-effects or random-effects analyses (Lipsey & Wilson, 2001). Compared to random-effects procedures, fixed-effects procedures assign greater weight to larger studies and have greater power to detect significant overall effects and moderators (Hedges & Olkin, 1985). Random-effects procedures, on the other hand, tend to increase the generalizability of results. Inferences based on fixed-effects procedures are limited to the specific sample of studies that are included in the meta-analysis (Hedges & Vevea, 1998). Inferences based on random-effects procedures, however, can be applied to the broader population of studies from which the meta-analytic sample is drawn (Hedges & Vevea, 1998). This study uses random-effects models because we wanted to have greater generalizability, and we believed that our large sample would allow us to overcome its power limitations.
We report the number of effects, point estimates, confidence intervals, and tests of significance for the entire sample and subgroups defined by our moderator variables. Prior to aggregation, each r was transformed to Zr using Fisher’s r-to-Z transformation. Afterwards, Zr was transformed back to r for interpretation purposes. Positive effect sizes indicated higher levels of RSB were associated with greater SU. Generally speaking, an effect size of r = ± .10 is considered to be a small effect, r = ± .30 is considered to be a medium effect, and an effect size of r = ± .50 is considered to be a large effect (Cohen, 1992).
To determine if moderator analyses were necessary, we tested for the presence of a significant amount of heterogeneity among the effect sizes. Categorical moderators (i.e., type of sample, nationality, race, type of SU, SU severity, method of assessment, type of RSB, SU, level of measurement, and type of document) were examined by testing whether the between-groups heterogeneity Qb is significantly different from zero. Qb follows a chi-square distribution and represents the variability in the effect sizes that can be explained by group differences. Continuous moderators (i.e., mean participant age, percent female, percent Caucasian, percent African descent, percent Hispanic, percent Asian, percent other, percent heterosexual, percent bisexual, percent homosexual, percent Lesbian, Gay, Bisexual, Transgender (LGBT)) were examined using meta-regression, which determines whether the slope between the moderator and effect size is significantly different from zero (see DeCoster, 2009).
3. RESULTS
3.1 Descriptive Analyses
Appendix A reports the mean age, sample type, drug being examined, RSB being examined, sample size, and effect size for each subsample analyzed in the meta-analysis. A complete table of all moderator variables is available from the first author upon request.
3.2 Overall relationship between substance use and risky sexual behavior
Table 1 contains statistics describing the overall distribution of effect sizes for SU and RSB. The weighted mean effect size was .22 for the random effects model, which would be classified as a small to medium effect according to Cohen’s (1992) guidelines. This positive effect size is significantly greater than zero, indicating that reports of SU are associated with engagement in RSB. There was a significant amount of heterogeneity among the effect sizes, indicating that there was more variability in the effect sizes than would expected due to chance alone, suggesting that study characteristics influenced the strength of this relationship.
Table 1.
Effects sizes by type of substance use and type of RSB
| Alcohol | Marijuana | Hard Drugs | Multiple Drugs | |
|---|---|---|---|---|
|
| ||||
| Unprotected Sex | ||||
| Number of Effects | 36 | 17 | 21 | 22 |
| Mean weighted r | .11 | .13 | .18 | .16 |
| Test comparing r to 0 | Z = 3.13, p = .002 | Z = 5.37, p < .001 | Z = 4.91, p < .001 | Z = 3.51, p < .001 |
| 95% CI | (.04, .18) | (.08, .17) | (.11, .25) | (.07, .25) |
| Range of r | (−.662, .58) | (−.20, .45) | (−.18, .41) | (−.26, .62) |
| Heterogeneity | Qw [35] = 1271.70 | Qw [16] = 70.57 | Qw [20] = 278.11 | Qw [21] = 846.74 |
| Number of partners | ||||
| Number of Effects | 18 | 11 | 16 | 9 |
| Mean weighted r | .25 | .33 | .25 | .29 |
| Test comparing r to 0 | Z = 5.38, p < .001 | Z = 4.61, p < .001 | Z = 5.71, p < .001 | Z = 5.10, p < .001 |
| 95% CI | (.16, .33) | (.19, .45) | (.16, .33) | (.18, .39) |
| Range of r | (−.27, .57) | (0, .75) | (.02, .61) | (.08, .87) |
| Heterogeneity | Qw [17] = 495.34 | Qw [10] = 936.91 | Qw [15] = 474.62 | Qw [8] = 119.24 |
| Sex with IVDU | ||||
| Number of Effects | 1 | 1 | 2 | No observations |
| Mean weighted r | .47 | .76 | .50 | |
| Test comparing r to 0 | Z = 8.5, p < .001 | Z = 13.96, p < .001 | Z = 10.11, p < .001 | |
| 95% CI | (.36, .58) | (.66, .88) | (.41, .57) | |
| Range of r | (.43, .5) | |||
| Heterogeneity | Qw [0] = 346.07 | Qw [0] = 41.41 | Qw [1] = 346.07 | |
| Multiple RSB | ||||
| Number of Effects | 12 | 4 | 12 | 12 |
| Mean weighted r | . 27 | .21 | .34 | .50 |
| Test comparing r to 0 | Z = 4.55, p < .001 | Z = 2.52, p = .012 | Z = 5.15, p < .001 | Z = 5.90, p < .001 |
| 95% CI | (.16, .38) | (.05, .36) | (.21, .45) | (.34, .62) |
| Range of r | (−.1, .51) | (.04, .32) | (.22, .40) | (.23, .79) |
| Heterogeneity | Qw [11] = 346.07 | Qw [3] = 41.41 | Qw [11] = 346.07 | Qw [11] = 346.07 |
Note: For all heterogeneity statistics, p < .001.
Although our literature search attempted to locate both published and unpublished research, we realize that publication biases may still have influenced the results of our meta-analysis. We therefore used the trim and fill method to evaluate the possible effects of publication bias on our estimate of the weighted mean effect size (Duval & Tweedie, 2000). This is a nonparametric method that measures publication bias by examining the symmetry of a funnel plot after methodically omitting studies until the plot is symmetrical. Missing studies are then imputed with the intent of preserving the symmetry of the funnel plot. The resulting adjusted mean effect size estimate, r = .04, indicates that the inclusion of missing studies would reduce the overall mean effect size. A 95% confidence interval around the adjusted mean effect size would be (−0.001, 0.091), suggesting that the observed relationship could have been caused by publication bias. The presence of a significant amount of heterogeneity among the effect sizes suggests the need to perform moderator analyses to determine if variability in the effect sizes can be explained by study characteristics.
3.3 Effect sizes by type of substance and type of risky sexual behavior
We examined the association between SU and RSB for each combination of substance type (i.e., alcohol, marijuana, hard drugs, and drugs and alcohol) and RSB type (i.e., unprotected sex, number of partners, sex with an IVDU, and multiple RSBs). As most of the studies included in this meta-analysis collapsed across substances such as narcotics, opiates, amphetamines, barbiturates, and stimulants, we created an aggregate category that incorporated all of these drugs referred to as hard drugs. We also created an additional category for drugs and alcohol, as many studies did not distinguish between the two. Table 2 presents the results of these analyses and shows that, with one exception, there was little variation in the relationship between SU and RSB across drugs. Specifically, effect sizes for condom use across all substances were within the small range (r = .11 to .18); effect sizes for number of partners across all substances were within the small to moderate range (r = .25 to .33); and three of four effect sizes for multiple RSBs were in the small to moderate range (r = .21 to .34).
Table 2.
Summary of effect size characteristics.
| Number of effects | 104 |
| Median r | .21 |
| Mean weighted r | .22 |
| Test comparing r to 0 | Z = 10.214, p < .001 |
| 95% confidence interval around mean weighted r | (.18, .26) |
| Range of r | (−.66, .77) |
| Heterogeneity | Qw = 3797.70, p < .001 |
There was one cell, the combination of multiple SU and multiple RSB, which diverged from this pattern. Whereas the effect size for multiple RSB was typically in the small to moderate range, the effect size in this cell was large (r = .50). There are several potential explanations for the observed finding. First, of the 12 studies represented in the referenced cell, 7 reported effect sizes in the small to moderate range (r = .23 to .46), and 5 reported large effect sizes (r = .59 to .79). The number of RSBs assessed in these 5 studies (averaging 3.8) was slightly larger than those assessed in the 7 studies reporting smaller effect sizes (averaging 3.1), which may have contributed to the difference. Moreover, all of the 5 studies reporting large effect sizes included a measure of intercourse with a high-risk sexual partner, which was absent from the 7 studies reporting smaller effect sizes and may have further contributed to the large effect sizes observed in these studies. Second, comparisons of effect sizes indicate that 4 of the 12 studies represented in this cell were based on data from clinical populations, which tended to report a higher overall effect size (r = .66) compared to community samples (r = .41).
Given the relative independence of the effects of SU type and RSB type, we believe that we were justified in performing individual moderator analyses for these two variables, which are presented in Table 3. We did not observe a significant influence of SU type on the relationship between SU and RSB. There was, however, a significant influence of RSB type. The strongest effect was found in studies that defined RSB as intercourse with an IVDU. The magnitude of this effect was followed by studies that used an aggregate measure of RSB. The smaller effects were among studies that measured RSB by reports of number of sexual partners and unprotected intercourse, respectively.
Table 3.
Results of moderator analyses for SU predicting type of RSB.
| Type of Drug | ||
| Alcohol | Number of effects | 66 |
| Weighted mean r | .173 | |
| 95% CI | .121 to .225 | |
| Marijuana | Number of effects | 29 |
| Weighted mean r | .193 | |
| 95% CI | .145 to .239 | |
| Hard drugs | Number of effects | 33 |
| Weighted mean r | .217 | |
| 95% CI | .169 to .263 | |
| Multiple drugs | Number of effects | 37 |
| Weighted mean r | .276 | |
| 95% CI | .197 to .348 | |
| Test | Qb [3] = 5.06, p = .18 | |
| Type of RSB | ||
| Unprotected sex | Number of effects | 71 |
| Weighted mean r | .153 | |
| 95% CI | .104 to .202 | |
| Number of sexual partners | Number of effects | 45 |
| Weighted mean r | .252 | |
| 95% CI | .206 to .297 | |
| Intercourse with IVDU | Number of effects | 2 |
| Weighted mean r | .530 | |
| 95% CI | .450 to .602 | |
| Multiple risky sexual behaviors | Number of effects | 28 |
| Weighted mean r | .382 | |
| 95% CI | .272 to .483 | |
| Test | Qb [3] = 59.72, p < .001 |
3.4 Other moderators
The results of the categorical moderator analyses are presented in Table 4 and the results of the continuous moderator analyses are presented in Table 5.
Table 4.
Results of other categorical moderator analyses for SU predicting RSB.
| Document type | ||
| Peer review Journal | Number of effects | 97 |
| Weighted mean r | .219 | |
| 95% CI | .177 to .259 | |
| Dissertation/Non-peer reviewed | Number of effects | 7 |
| Weighted mean r | .196 | |
| 95% CI | .035 to .337 | |
| Test | Qb [1] = .082, p = .77 | |
| Nationality | ||
| United States & Canada | Number of effects | 76 |
| Weighted mean r | .205 | |
| 95% CI | .164 to .244 | |
| Europe | Number of effects | 7 |
| Weighted mean r | .248 | |
| 95% CI | .119 to .368 | |
| Latin America | Number of effects | 2 |
| Weighted mean r | .273 | |
| 95% CI | .042 to .476 | |
| Asia | Number of effects | 4 |
| Weighted mean r | .196 | |
| 95% CI | −.023 to .398 | |
| Africa | Number of effects | 10 |
| Weighted mean r | .131 | |
| 95% CI | .021 to .238 | |
| Australia/New Zealand | Number of effects | 4 |
| Weighted mean r | .421 | |
| 95% CI | .257 to .561 | |
| Number studies with multiple effects | 68 | |
| Test of moderator including all effects | Qb [5] = 8.99, p =.11 | |
| Sample Type | ||
| Community | Number of effects | 87 |
| Weighted mean r | .215 | |
| 95% CI | .169 to .260 | |
| Clinical | Number of effects | 8 |
| Weighted mean r | .418 | |
| 95% CI | .269 to .547 | |
| Forensic | Number of effects | 8 |
| Weighted mean r | .110 | |
| 95% CI | −.046 to .261 | |
| Number studies with multiple effects | 67 | |
| Test of moderator including all effects | Qb [2] = 8.65, p = .01 | |
| Drug Use Assessment | ||
| Self-report/Self-administered | Number of effects | 58 |
| Weighted mean r | .237 | |
| 95% CI | .180 to .293 | |
| Interview | Number of effects | 45 |
| Weighted mean r | .210 | |
| 95% CI | .140 to .280 | |
| Test of moderator including all effects | Qb [1] = .337, p = .56 | |
| Sexual Behavior Assessment | ||
| Self-report/Self-administered | Number of effects | 62 |
| Weighted mean r | .237 | |
| 95% CI | .182 to .291 | |
| Interview | Number of effects | 41 |
| Weighted mean r | .196 | |
| 95% CI | .128 to .262 | |
| Test | Qb [1] = .899, p = .34 | |
| SU Definition | ||
| Frequency & Quantity of use | Number of effects | 41 |
| Weighted mean r | .282 | |
| 95% CI | .213 to .348 | |
| Dichotomous user/nonuser | Number of effects | 55 |
| Weighted mean r | .155 | |
| 95% CI | .104 to .206 | |
| Clinical Diagnosis | Number of effects | 9 |
| Weighted mean r | .304 | |
| 95% CI | .238 to .367 | |
| Test | Qb [2] = 15.47, p < .001 | |
| Level of SU Measurement | ||
| Global association | Number of effects | 83 |
| Weighted mean r | .234 | |
| 95% CI | .186 to .280 | |
| Situational | Number of effects | 19 |
| Weighted mean r | .307 | |
| 95% CI | .209 to .400 | |
| Event level | Number of effects | 16 |
| Weighted mean r | .071 | |
| 95% CI | −.001 to .142 | |
| Test | Qb [2] = 19.43, p < .001 | |
| Level of RSB Measurement | ||
| Global association | Number of effects | 83 |
| Weighted mean r | .260 | |
| 95% CI | .217 to .303 | |
| Situational | Number of effects | 9 |
| Weighted mean r | .124 | |
| 95% CI | .071 to .176 | |
| Event level | Number of effects | 22 |
| Weighted mean r | .064 | |
| 95% CI | .002 to .125 | |
| Test | Qb [2] = 30.71, p < .001 |
Table 5.
Results of continuous moderator analyses for SU predicting RSB.
| Publication Year | |
| Number of effects | 242 |
| Unstandardized slope | −.018 |
| Standard error of slope | .0005 |
| Test of slope ≠ 0 | Z = −39.96, p < .001 |
| Mean Age | |
| Number of effects | 236 |
| Unstandardized slope | .012 |
| Standard error of slope | .001 |
| Test of slope ≠ 0 | Z = 10.34, p < .001 |
| % African descent | |
| Number of effects | 203 |
| Unstandardized slope | −.003 |
| Standard error of slope | .00005 |
| Test of slope ≠ 0 | Z = −49.61, p < .001 |
| % Caucasian | |
| Number of effects | 188 |
| Unstandardized slope | .002 |
| Standard error of slope | .00007 |
| Test of slope ≠ 0 | Z = 35.35, p < .001 |
| % Hispanic | |
| Number of effects | 180 |
| Unstandardized slope | .0055 |
| Standard error of slope | .00014 |
| Test of slope ≠ 0 | Z = 38.09, p < .001 |
| % Asian | |
| Number of effects | 168 |
| Unstandardized slope | .004 |
| Standard error of slope | .0003 |
| Test of slope ≠ 0 | Z = 15.15, p < .001 |
| % Female | |
| Number of effects | 236 |
| Unstandardized slope | .0004 |
| Standard error of slope | .00007 |
| Test of slope ≠ 0 | Z = 6.289, p < .001 |
| % Heterosexual | |
| Number of effects | 14 |
| Unstandardized slope | −.004 |
| Standard error of slope | .0004 |
| Test of slope ≠ 0 | Z = −10.10, p < .001 |
| % Homosexual | |
| Number of effects | 18 |
| Unstandardized slope | .00004 |
| Standard error of slope | .0002 |
| Test of slope ≠ 0 | Z = .148, p = .88 |
| % Bisexual | |
| Number of effects | 10 |
| Unstandardized slope | −.028 |
| Standard error of slope | .003 |
| Test of slope ≠ 0 | Z = −8.76, p < .001 |
| % LGBT | |
| Number of effects | 14 |
| Unstandardized slope | .005 |
| Standard error of slope | .0009 |
| Test of slope ≠ 0 | Z = 5.27, p < .001 |
3.4.1 Document Type
There were two types of documents represented in our sample: published, peer-reviewed manuscripts and unpublished manuscripts, including theses and dissertations. Document type was not a significant moderator of the SU and RSB relationship, suggesting that variation in document type did not have a significant impact on effect sizes.
3.4.2 Nationality
We examined whether the nationality of the sample had a significant impact on effect sizes. This variable was divided into six geographic locations: the USA and Canada, Europe, Latin America/South America/Mexico, Asia, Africa, and Australia/New Zealand. Nationality was not a significant moderator of the SU and RSB relationship, suggesting that variations in effect sizes were not the result of differences across nationalities.
3.4.3 Sample Type
Studies within this meta-analysis used one of three sample types: clinical, community, or forensic. Our results indicated that the association between SU and RSB differed significantly in strength depending on the type of sample. The largest effect was observed in clinical samples, or among individuals receiving inpatient or outpatient psychiatric treatment. This was followed by community populations, in which individuals often come from a variety of backgrounds. The smallest effects were found in forensic populations, or populations in which adolescents were in a juvenile facility or directly involved with the juvenile courts. It is notable that the effect for forensic populations was not significant, as the confidence interval contained zero.
3.4.4 SU and RSB Assessment
Two categories were coded to differentiate the way in which SU and RSB were assessed. The first category includes studies in which either SU or RSB were measured by means of self-report or self-administered questionnaires. The second category includes studies in which either SU or RSB were measured by means of a face-to-face interview. Our results indicated that neither SU nor RSB assessment were significant moderators of the SU and RSB relationship, suggesting that effect sizes did not vary by the way in which the variables were measured.
3.4.5 SU definition
There were three categories that comprised the SU definition variable: clinical diagnosis, frequency and/or quantity, and dichotomous user/non-user. Studies in which participants were identified as having a substance use disorder were included in the clinical diagnosis category. Studies in which the measure of SU was based on how much (i.e., quantity) and/or how often (i.e., frequency) a participant used a given substance were included in the frequency and/or quantity category. Studies in which the measure of SU was based on a dichotomous distinction, such as user/non-user, were included in the dichotomous user/non-user category. Our results indicated that there was a significant effect of the way in which SU was defined on the SU to RSB relationship. The largest effect was found in studies that used clinical diagnoses to determine the presence of substance use disorders. This effect was followed in magnitude by studies in which SU was measured by frequency and/or quantity of use. The smallest effects were found in studies in which SU was defined dichotomously.
3.4.6 Level of SU and RSB measurement
We found that studies were often inconsistent in their classification of the level of SU and RSB relationship. Specifically, studies often measured SU at one level (e.g., global) and measured RSB at another level (e.g., event). As a result, it was necessary to separate this variable into two separate levels, one for SU and another for RSB.
Regarding level of SU measurement, moderator analyses indicated that there was a significant effect such that the largest effect was found in studies in which SU was measured at the situational level, followed by studies that measured SU globally, followed by studies that measured SU at the event level. It is notable that the point estimate for the event-level studies was not significantly different from zero. Regarding level of RSB measurement, moderator analyses indicated that there was a significant effect such that the largest effects were found in studies that measured RSB at the global level, followed by those that measured RSB at the situational level, followed by those that measured RSB at the event level. Just as with SU, the point estimate for the event-level studies was not significantly different from zero.
3.4.7 Publication year
We coded publication year continuously and found that there was a significant relationship between publication year and effect size, such that the relationship between SU and RSB was stronger in older studies than in newer studies.
3.4.8 Age
Age was also coded continuously and there was a significant relationship between age and effect size, such that the relationship between SU and RSB was stronger in studies with older participants.
3.4.9 Sex
Although sex is a categorical variable at the subject level, at the study level, it is naturally continuous. When a study reported frequencies of participants’ sex and did not provide results separately by sex, we coded the proportion of females in the study. When a study reported the results separately by sex, we included separate effect sizes for females and males, coding the effect size for females as 100% and the effect size for males as 0%. Our results indicated that there was a significant relationship between the percent of female participants and effect size, such that the relationship between SU and RSB was stronger in studies that had more female participants.
3.4.10 Ethnicity
We coded ethnicity continuously at the study level. Studies represented in our sample consisted of participants of African, Caucasian, Hispanic, and Asian descent. We coded the proportion of participants from each group from 0–100%. The moderating effects of ethnicity are illustrated in Figure 1. The relationship between SU and RSB was weaker in studies that had more participants of African descent. Conversely, the relationship between SU and RSB was stronger in studies that had more Caucasians, Hispanics, or Asians.
Figure 1.

Ethnicity
3.4.11 Sexuality
We coded sexuality continuously at the study level in the same way that we coded ethnicity. Sexuality consisted of four groups: homosexual, heterosexual, bisexual, or LGBT. We created a LGBT category because there were a significant amount of studies that did not distinguish between homosexual and bisexual participants thereby limiting our ability to use separate codes. The moderating effects of sexuality are illustrated in Figure 2. The relationship between SU and RSB was weaker when the samples had greater proportions of heterosexual or bisexual participants. The proportion of homosexual participants did not have a significant influence of the relationship between SU and RSB, but the relationship between SU and RSB was stronger in the samples that had greater proportions of participants in the LGBT category.
Figure 2.
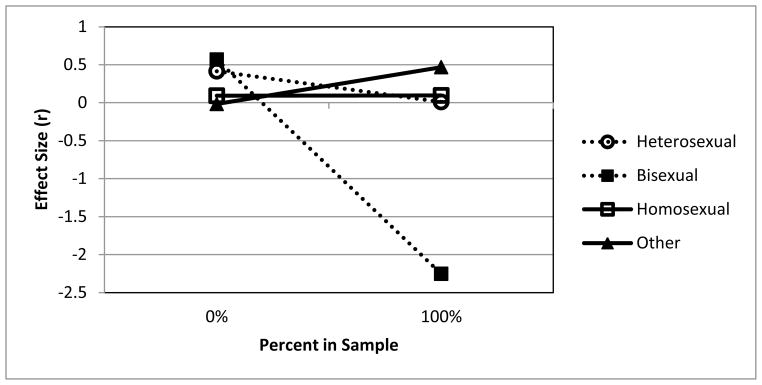
Sexuality
Note: Identification as homosexual was not a significant moderator.
3.5 Relations among moderator variables
The examination of individual moderators in isolation could be problematic, as it is possible that some of these significant relations were just due to collinearity among the moderators. Therefore, we next used correlations, chi-square tests, and ANOVAs to determine if there were any significant relations among the moderators. We observed 13 significant moderators of the relationship between SU and RSB. The significant results from these analyses (using α = 0.0004 based on a Bonferroni correction) are presented in Table 6. The associations between level of SU measurement and level of RSB measurement indicated that the way that one variable was measured tended to match the way that the other was measured (X2 = 195.87; p < 0.001). The associations of level of SU measurement (X2 = 26.82; p < 0.001) and level of RSB measurement (X2 = 52.55; p < 0.001) with RSB definition indicated that event analyses and situational measures are more commonly found in investigations of condom use than in studies using other definitions of RSB. The relationship between sample type and level of RSB measurement indicated that event analyses were more common in forensic samples than in clinical or community samples (X2 = 21.79; p < 0.001). The significant relationship between sample type and SU definition indicated that, compared to community samples, clinical samples are more likely to use clinical diagnoses and forensic samples are more likely to use dichotomous assessments (X2 = 24.63; p < 0.001). The relations of SU definition (F [2, 221] = 9.71; p < 0.001) and sample type (F [2, 231] = 20.72; p < 0.001) with mean age indicated that youth diagnosed with substance use disorders and those recruited from community samples were significantly older than their peers.
Table 6.
Significant relations among moderators
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||||
| 1. Publication year | -- | ||||||||||||
|
|
|||||||||||||
| 2. Mean age | -- | X | X | ||||||||||
|
|
|||||||||||||
| 3. Percent African descent | -- | ||||||||||||
|
|
|||||||||||||
| 4. Percent Caucasian | -- | ||||||||||||
|
|
|||||||||||||
| 5. Percent Hispanic | -- | ||||||||||||
|
|
|||||||||||||
| 6. Percent Asian | -- | ||||||||||||
|
|
|||||||||||||
| 7. Percent Heterosexual | -- | X | |||||||||||
|
|
|||||||||||||
| 8. Percent Bisexual | -- | ||||||||||||
|
|
|||||||||||||
| 9. Sample type | X | -- | X | X | |||||||||
|
|
|||||||||||||
| 10. SU definition | X | X | -- | ||||||||||
|
|
|||||||||||||
| 11. RSB definition | X | -- | X | X | |||||||||
|
|
|||||||||||||
| 12. Level of SU | X | -- | X | ||||||||||
|
|
|||||||||||||
| 13. Level of RSB | X | X | X | -- | |||||||||
|
|
|||||||||||||
4. DISCUSSION
Studies investigating the relationship between SU and RSB have generated mixed results; many studies have found a positive relationship (e.g., Bryan, Ray, & Cooper, 2007), others have found negative relations (Khasakhala & Mturi, 2008), and still others have found no association between the two variables (e.g., Ellickson et al., 2005). In the present meta-analysis, we investigated the association between each combination of type of SU and type of RSB. Our results indicated that, of all SU categories, alcohol use was the most studied substance, followed by hard drugs, multiple drugs, and marijuana use, respectively. Of all RSB categories, unprotected sex was the most studied sexual behavior, followed by number of sexual partners, multiple RSBs, and sex with an IVDU, respectively. It is notable that there was little variation in the relationship between specific substances and RSB across drugs, such that it appears that the type of substance being examined tended to have little impact on the relationship between SU and RSB. This finding would suggest that, for most adolescents, it does not matter which kind of substance use they engage in, as there is a persistent relationship between any type of SU and RSB. We did, however, find that effect sizes tended to vary by type of RSB, such that studies that defined RSB as intercourse with an IVDU reported the strongest effect sizes, followed by studies that used an aggregate measure of RSB, number of sexual partners, and unprotected sex. Taken together, these findings call for greater focus on type of RSB and moderators of the relationship between SU and RSB.
After examining the effect sizes by SU type and RSB type, we investigated whether a consistent relationship exists between SU and RSB across all studies. Overall, a small to moderate, positive association (r = .22) was identified. According to Cohen (1992), this is a small-to-medium-sized effect. Based on Hemphill’s (2003) analysis, an effect size of this magnitude would fall in the middle third of those typically observed in the psychological literature. We observed a significant amount of heterogeneity in the effect sizes. Moderator analyses demonstrated that this heterogeneity could be explained by sample characteristics, measurement factors, and publication characteristics.
4.1. Effects of sample characteristics on the relationship between SU and RSB
4.1.1 Sex
The results of this study suggest that samples including more females had stronger relations between SU and RSB. One study, for example, found that females were twice as likely as their male counterparts to report that alcohol prior to intercourse influenced their decision to engage in unprotected intercourse (Bryan et al., 2007). There are several reasons why the magnitude of the association between SU and RSB might be greater among females than among males. Physiological research has shown that the effects of SU can vary substantially by sex. For example, women are more affected by alcohol because of their lower rates of gastric metabolism, body weights, and body mass indices (Wechsler, Dowdall, Davenport, & Rimm, 1995). This may lead to a greater impairment of their sexual decision-making abilities.
There may also be social reasons why the relationship between SU and RSB is stronger for females. DiClemente et al. (2002) have reported that adolescent females are more likely to report having intercourse with older partners than adolescent males. According to the Theory of Gender and Power, power differentials favoring the male partner in a romantic relationship often put females at increased health risk (Marin, Coyle, Gomez, Carvajal, & Kirby, 2000). For example, adolescent female substance users may perceive that they have less self-efficacy to insist on condom use when their primary drug supplier is their older male sexual partner (DiClemente et al., 2002). Similarly, when an adolescent female has been using drugs, the difficulty of negotiating condom use with a partner may be exacerbated, especially given the perceived control that the male has over condom use (e.g., Bryan et al., 2007).
4.1.2 Ethnicity
The pattern of results suggests that the most positive relationship between SU and RSB was found amongst Hispanics, followed by Asians, followed by Caucasians. The results also suggest that there is not a relationship between SU and RSB amongst those of African descent. For Hispanics, Asians, and Caucasians, it is possible that engagement in both behaviors is indicative of a Problem Behavior Syndrome (PBS) (Donovan, Jessor, & Costa, 1988). PBS is often defined as a general tendency to engage in multiple problematic behaviors, in this case, SU and RSB (Sullivan, Childs, & O’Connell, 2009). Consistent with this theory, previous research has linked Conduct Disorder and impulsivity to RSB and alcohol misuse (Crockett, Raffaelli, & Shen, 2006). If the presence of PBS varies across ethnicity, we would expect to also see the relationship between SU and RSB vary across ethnicity. We observed that adolescents of African descent show weaker associations between SU and RSB, which may suggest that problem behaviors are more individualized in this group. This could explain the lackluster results reported by some intervention programs whose aims to reduce HIV-risk behaviors have centered on interventions designed to reduce SU in this population (Jackson, Geddes, Haw, & Frank, 2012).
4.1.3 Age
Our results indicate that samples with a higher mean age reported greater associations between SU and RSB than samples of younger adolescents. There are many reasons why stronger associations between these two risk behaviors may be found among older adolescents. As children age, there is often a reduction in the social controls, such as parental monitoring, that limit the opportunities they have to engage in risk behaviors. Not only do older adolescents enjoy less oversight, they are also more likely to befriend peers who engage risky behaviors, thereby creating pressure to conform (e.g., Millburn, 2007). It is possible that older adolescents are more likely to test the effects of drugs on their behaviors, including sexual behaviors, as the drugs themselves are more available and cultural norms make their use more acceptable as the adolescents grow older (Casey & Jones, 2010).
4.1.4 Sample type
The results of this study indicate that the strength of the relationship between SU and RSB was greatest among adolescents in clinical settings, such as inpatient or outpatient psychiatric institutions, followed by those in community settings, followed by those in forensic settings (where the relationship was not significant). The large relationship between SU and RSB found in clinical samples may be caused by the increased likelihood of these individuals having psychological disorders. Brown, Danovsky, Lourie, DiClemente, and Ponton (1997) found that adolescents with psychiatric disorders were at greater risk for contracting a sexually transmitted disease (Brown et al., 1997). Furthermore, previous research has demonstrated that adolescents with comorbid psychiatric and substance use disorders within inpatient settings are at increased risk for engaging in HIV-risk behaviors (DiClemente & Ponton, 1993).
The nonsignificant effect within forensic samples is difficult to explain. We believe that we may have obtained inconclusive findings because this category includes several distinct subpopulations. Unfortunately, we are not able to take a more precise investigation of these studies because many studies conducted on juvenile populations fail to indicate the category in which their alleged crimes fall. It is possible that the relationship between SU and RSB varies between those incarcerated for different types of criminal offenses, which, when averaged together, produce the overall null finding.
4.1.5 Sexuality
The pattern of results suggests that there was no relationship between SU and RSB in homosexual or heterosexual populations, a negative relationship between SU and RSB in bisexual populations, and a positive relationship between SU and RSB in LGBT populations. We do not believe that this necessarily reflects reality. We instead believe this pattern to be an artifact of our need to include a general LGBT category. Some studies combined homosexual and bisexual participants into a single category and other studies combined heterosexual and bisexual participants into a single category. Given that our results suggest that the relationship between SU and RSB found in bisexual samples may be very different from those found in heterosexual or homosexual samples, this could lead to contradictory and confusing results. Rather than drawing firm conclusions about how sexuality moderates the relationship between SU and RSB, we would instead like to suggest that future research on this relationship be more careful and precise about the way in which they assess the sexuality of their participants.
4.2 Effects of measurement factors on the relationship between SU and RSB
4.2.1 RSB definition
The strongest association between SU and RSB was found when studies examined whether participants had intercourse with an IVDU, followed by studies using an aggregate measure of RSB, followed by studies examining the number of sexual partners, followed by studies examining condom use. There was a relatively small number of studies that examined the relationship between SU and intercourse with an IVDU, so the estimate in this category must be interpreted cautiously. Social and contextual factors might explain the strength of the association between SU and RSB when RSB is defined by sex with an IVDU or composite measure of RSB. Previous research, for example, has suggested that mental health challenges, such as depression and anxiety, may be driving the observed associations (Chan, Passetti, Garner, Lloyd, & Dennis, 2011). Furthermore, adolescents with substance use disorder and co-morbid psychiatric challenges are at greater risk for engaging in high-risk and multiple risky sexual behaviors (Chan et al., 2011).
4.2.2 SU definition
The strongest association was found in studies assessing SU through clinical diagnoses of substance use disorders, followed by studies in which SU was measured by frequency and/or quantity of use, followed by studies in which SU was measured dichotomously (e.g., user versus nonuser). The differences in these effects may be due to the different types of substance use captured by the different definitions. Adolescents with substance use disorders often report greater participation in risky behaviors, including SU and RSB (Cook et al., 2006). Specifically, adolescents with substance use disorders have reported having at least twice as many sexual partners and were 70% more likely to have been diagnosed with an STI than their peers without substance abuse disorders (Cook et al., 2006). Dichotomous measures of SU, on the other hand, are often global measurements of SU that may or may not present problems for emerging adults. Such measures may fail to assess the severity of SU or may present a spurious relationship due to the impact of an unidentified third variable, such as personality (Newcomb, Clerkin, & Mustanski, 2011). Additionally, the dichotomization of continuous variables often produces less powerful and more biased results (DeCoster, Iselin, & Gallucci, 2009).
4.2.3 Level of measurement
For RSB, the largest effects were observed when RSB was measured at the global level, followed by when RSB was measured at the situational level, followed when RSB was measured at the event level. For SU, the strongest effects were found when SU was measured at the situational level, followed by studies that measured SU at the global level, followed by studies that measure SU at the event level. The results for SU and RSB are similar in that, in both cases, the strongest relationship is observed using some type of aggregate measure (either global or situational), and the weakest relationship is observed using a specific, event-level measure. Taken together, these findings suggest that while the extent to which someone uses drugs and the extent to which they engage in risky sex may be related at an aggregate level, it is not necessarily the case that when someone uses drugs prior to having sex on a specific occasion that they are significantly more likely to participate in RSB than they would compared to another occasion where they were not using drugs. This interpretation is consistent with Brown and Vanable (2007), who found that for many adolescents, RSB is just as likely when someone is or is not under the influence. However, event-level studies are susceptible to retrospective bias. Depending the quantity and frequency of SU, it is often difficult for participants to recall specific events, such as the first or last intercourse (Halpern-Felsher, Millstein, & Ellen, 1996).
4.3 Effects of publication characteristics on the relationship between SU and RSB
4.3.1 Publication year
Older studies tended to report higher effect sizes than newer studies. This is likely due to the advances in our knowledge of best practices in terms of studying the relationship between SU and RSB. For example, most of the older studies assessed the relationship between SU and RSB globally. Newer studies, on the other hand, have incorporated new methods, such as situational and event-level measurements, that have been associated with weaker effects. Additionally, newer studies also include more specific measures of risky sex and consider a wider range of substances. Alternatively, lower effect sizes over time could be a function of our advancement in education and knowledge of adolescent RSB. It is possible that intervention and prevention programs have led to an overall weakening of the relationship between these two behaviors by educating people on the effects of pairing SU and sexual intercourse.
4.4 Relations between significant moderators
Our analyses indicated that there were many significant relations among the examined moderators. For example, the percentage of females in the study was significantly related to other moderators, such as sample type and level of SU and RSB. These findings support the call for additional research to separate the effects of these variables and enable us to understand how they impact the relationship between SU and RSB among adolescents. We must therefore be careful when interpreting the tests of moderators that are related to other factors because the moderator may only have a significant relationship because of collinearity, and not because it actually influences the effect.
4.5 Limitations
Prior to discussing the implications, there are some limitations that must be considered when drawing conclusions from this meta-analysis. While we did observe a significant positive association between SU and RSB, the correlational nature of meta-analytic data does not allow us to make causal inferences. Accordingly, we cannot make the claim that these data indicate that SU causes RSB because the relationship between the two variables could be caused by an unmeasured third variable, or the causal direction could be reversed.
A second potential limitation of this meta-analysis arises from our broad inclusion criteria. We wanted our analyses to estimate the relationship between SU and RSB across all of adolescence and young adulthood, including studies that were performed in a variety of settings. While our method successfully enabled us to describe these broad trends, it simultaneously limits our ability to detect trends that may only appear in specific subpopulations or age groups. It may also be that the mechanisms responsible for this relationship may vary between these groups.
The diversity of methodology and assessment techniques often makes examining the impact of mediators and moderators on specific health risk behaviors difficult. It is important, for reliability and validity purposes, that researchers operationalize behaviors in similar ways. However, in the SU and RSB literature, these risk behaviors are often measured in a variety of ways, often with insufficient items. This reduces our ability to generalize from our results.
4.6 Implications for intervention and prevention
Although our meta-analysis indicates that there is a positive association between SU and RSB, this effect was small to moderate in size and was heterogeneous across the sample of studies. This suggests that there may be individual, contextual, and environmental factors that significantly impact the co-occurrence of these risk behaviors. The diversity of the potential causes for adolescent participation in these risky behaviors calls for the development of targeted intervention programs that are aimed at individuals who participate in similar risk behaviors for similar reasons in similar contexts. In other words, intervention programs should be tailored to the population being treated.
The present meta-analysis indicates that context, sexuality, sex, and ethnicity are important sources of variability in the relationship between SU and RSB. This suggests some changes in the way in which future studies investigating this relationship should be conducted. For example, previous research has tended to lump all adolescents into the same category under the assumption that the similarity in age was more important than dissimilarities due to contextual factors. Future studies may be more successful if researchers accommodate potential differences in the relationship between SU and RSB in different demographic groups.
4.7 Conclusions
This meta-analysis showed that the relationship between SU and RSB is in the small-to-moderate range. We found that this relationship is moderated by several study and sample characteristics. Study design had a significant impact on the observed relationship between SU and RSB. Though our study demonstrated that relationships assessed at the global and situational levels produced the strongest effect sizes, it is important to note that global and situational studies lack the appropriate specificity to enable researchers to link specific instances of SU to specific sexual acts. Similarly, event level studies that focus only on a single event, such as first or last intercourse, lack the detail needed to gauge trends in youth sexual behavior. More longitudinal studies employing event level measurements are needed to allow more accurate predictions of sexual behavior. The significant moderators of this relationship suggest that contextual factors must be considered when examining the relationship between SU and RSB. More studies are needed that go beyond simplistic examination of these two variables in order to understand how individual, social, and environmental factors interact to contribute to engagement in both SU and RSB. Furthermore, we suggest that intervention and prevention programs for adolescents should be tailored to the characteristics of those being treated. Our results, for example, suggest that SU is more strongly related to RSB among females, individuals of Asian, Hispanic, and Caucasian descent, and older youth. Intervention and prevention programs targeting these groups should therefore pay greater attention the role of SU in the performance of RSB in order to have the greatest impact.
Highlights.
Substance use is more strongly related to risky sex among females than males
Ethnicity moderated the relationship between substance use and risky sex
Type of drug had little impact on the link between substance use and risky sex
Event-level studies did not moderate the link between substance use and risky sex
Acknowledgments
The research reported here was supported by the National Institute on Drug Abuse (3R01DA023156-02S2).
Appendix. Descriptives from included studies
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| Pritchard & Cox (2007) | 15 | Community | A | C | 1690 | 0.231 | |
| Ramrakha et al. (2000) | 21 | Community | P | G | 992 | 0.273 | |
| Hoffman et al. (2006) | 19.1 | Community | A | C | 50 | 0.154 | |
| Bryan, Ray, & Cooper (2007) | 15.56 | Forensic | A | C | 226 | 0 | |
| Naff Johnson (1996) | Males | 19 | Community | A | G | 262 | 0.313 |
| Naff Johnson (1996) | Females | 19 | Community | A | G | 262 | 0.567 |
| Poulin & Graham (2001) | Males | 16 | Community | A, M | C, MSP | 1789 | 0.061 |
| Poulin & Graham (2001) | Females | 16 | Community | A, M | C, MSP | 1789 | 0.083 |
| Guo et al. (2002) | 21 | Community | A, M, H | C, MSP | 625 | 0.38 | |
| Koopman, Rosario, & Rotheram-Borus (1994) | 15.6 | Community | A, M, H, | C, MSP | 302 | 0.236 | |
| Lowry et al. (1994) | Community | M, H | C, MSP | 11,631 | 0.374 | ||
| Gomez, Sola, Cortes, & Mira (2007) | 18.24 | Community | A | G | 338 | 0.211 | |
| Kingree & Betz (2003) | 15.43 | Forensic | A, M | C | 210 | 0.113 | |
| Kingree & Phan (2002) | 14.82 | Forensic | A, M | C | 205 | 0.126 | |
| Ellickson et al. (2005) | Males | 23 | Community | A, M, H, P | C, G | 3401 | 0.408 |
| Ellickson et al. (2005) | Females | 24 | Community | A, M, H, P | C, G | 3401 | 0.383 |
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| Twa-Twa, Oketcho, Siziya, & Muula (2008) | 16.34 | Community | A, P | C | 193 | −0.064 | |
| Voisin et al. (2007) | 15.4 | Forensic | A, M, H, P | C | 550 | 0.068 | |
| Deas-Nesmith, Brady, White, & Campbell (1999) | 14.8 | Clinical | P | C | 90 | 0.475 | |
| Rotheram-Borus et al. (1994) | 16.8 | Community | A, M, H | C | 131 | −0.177 | |
| Bachanas et al. (2002a) | 12–15 years old | 15.7 | Community | P | G | 72 | −0.029 |
| Bachanas et al. (2002a) | 16–19 years old | 15.7 | Community | P | G | 92 | −0.076 |
| Donenberg et al. (2001) | 16.01 | Clinical | P | G | 86 | 0.66 | |
| Brown & Vanable (2007) | 18.9 | Community | A | C | 320 | 0.054 | |
| Roberts & Kennedy (2006) | 20.2 | Community | P | C | 100 | 0.237 | |
| Strunin & Hingson (1992) | 17.34 | Community | A, M | C | 398 | 0.02 | |
| Mpofu et al. (2005) | 16.36 | Community | A, M, H | MSP | 1526 | 0.288 | |
| Baskin-Sommers & Sommers (2006) | 21.41 | Community | A, M, H | C, MSP | 243 | 0.135 | |
| Fergusson & Lynskey (1996) | Males | 15.5 | Community | A | C, MSP | 953 | 0.541 |
| Fergusson & Lynskey (1996) | Females | 15.5 | Community | A | C, MSP | 953 | 0.501 |
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| Crockett, Raffaelli, & Shen (2006) | 16.5 | Community | P | G | 518 | 0.26 | |
| Cook et al. (2006) | Males | 20.4 | Community | P | C, MSP | 448 | 0.204 |
| Cook et al. (2006) | Females | 20.4 | Community | P | C, MSP | 448 | 0.235 |
| Morrison et al. (2003) | 17 | Community | A | C | 73 | 0.033 | |
| Babikian et al. (2004) | 18.3 | Community | A | G | 299 | 0.51 | |
| MacKellar et al. (2000) | Males | 16.5 | Community | A | C | 879 | 0 |
| MacKellar et al. (2000) | Females | 16.5 | Community | A | C | 879 | −0.09 |
| Bailey, Camlin, & Ennett (1998) | 17 | Community | A, M, H | C, MSP, IV | 289 | 0.401 | |
| Wislar & Fendrich (2000) | Males | 15.2 | Forensic | M, H | MSP | 12,887 | 0.16 |
| Wislar & Fendrich (2000) | Females | 15.2 | Forensic | M, H | MSP | 12,887 | 0.126 |
| Celentano et al. (2006) | 18.5 | Community | A, M, H | C | 3492 | 0.07 | |
| Grossbard et al. (2007) | 18 | Community | A | MSP | 2123 | 0.38 | |
| Heffernan, Chiasson, & Sackoff (1996) | 17.5 | Community | H | MSP, IV | 220 | 0.322 | |
| Khasakhala & Mturi (2008) | Males | 19.94 | Community | A | G | 3716 | −0.193 |
| Khasakhala & Mturi (2008) | Females | 19.94 | Community | A | G | 3716 | 0.032 |
| Bailey, Gao, & Duncan (2006) | 19.7 | Other | A, P | C | 134 | 0.107 | |
| McNall & Remafedi (1999) | 19.23 | Community | A, M, H | C | 817 | 0.234 | |
| Morrison-Beedy, Carey, Feng, & Tu (2008) | 19.5 | Community | A, M, H | C | 102 | 0.228 | |
| Gleghorn, Marx, Vittinghoff, & Katz (1998) | 17.5 | Community | H | MSP | 766 | 0.235 | |
| Kebede et al. (2005) | 19.5 | Community | A, H | C | 16606 | 0.451 | |
| Smith & Brown (1998) | 20.03 | Community | Alcohol | Multiple RSB | 215 | 0.373 | |
| Duncan, Strycker, & Duncan (1999) | 15.96 | Community | A, M | G | 172 | 0.206 | |
| Duncan, Strycker, & Duncan (1999) | 15.96 | Community | A, M | G | 172 | 0.14 | |
| Mpofu et al. (2006) | 16.3 | Community | A | MSP | 630 | 0.25 | |
| Rotheram-Borus, Rosario, Reid, & Koopman (1995) | 16.5 | Community | A, P | C | 65 | 0.282 | |
| Hingson, Strunin, Berlin, & Heeren (1990) | 17.5 | Community | A, H | C | 1050 | 0.113 | |
| Remafedi (1994) | 19.9 | Community | P | C | 238 | 0.235 | |
| Brook, Brook, Pahl, & Montoya (2002) | 15.1 | Community | P | C, MSP | 2837 | 0.36 | |
| Thompson Jr. (2003) | 16.3 | Community | A, M | G | 351 | 0.306 | |
| Baker & Mossman (1991) | 14.4 | Clinical | P | G, MSP | 23 | 0.765 | |
| Kraft, Rise, & Traeen (1990) | Males | 18.07 | Community | A | C | 1172 | 0.214 |
| Kraft, Rise, & Traeen (1990) | Females | A | C | 0.256 | |||
| Crosby et al. (2008) | 17.8 | Community | P | C | 715 | 0.19 |
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| Koniak-Griffin & Brecht (1995) | 16.64 | Community | A, M, H | C, MSP | 151 | 0.239 | |
| Rotheram-Borus, Mann, & Chabon (1999) | 21.4 | Community | H | C, MSP | 337 | 0.125 | |
| Abrantes et al. (2006) | 15.3 | Clinical | P | C, MSP | 239 | 0.197 | |
| Refaat (2004) | 18 | Community | P | G | 687 | 0.457 | |
| Yan, Chiu, Stoesen, & Wang (2007) | 16.1 | Community | A, M, H, P | C, MSP | 5745 | 0.149 | |
| Mbulo (2005) | 20.6 | Community | A | C, MSP | 961 | −0.132 | |
| Donenberg, Emerson, Bryant, & King (2006) | 15.12 | Clinical | P | G | 207 | 0.54 | |
| Tubman & Langer (1995) | 17.2 | Clinical | A | C | 115 | −0.662 | |
| Hou & Basen-Engquist (1997) | Caucasian | 16 | Community | M | C | 2706 | 0.034 |
| Hou & Basen-Engquist (1997) | Asian/PI | 16 | Community | P | C | 2706 | −0.055 |
| Bachanas et al. (2002b) | 15.7 | Community | P | G | 158 | 0.43 | |
| Scivoletto et al. (2002) | 17.7 | Community | A, M, H | C | 689 | 0.178 | |
| Donenberg, Wilson, Emerson, & Bryant (2002) | Males | 15.45 | Clinical | P | C, MSP, G | 169 | 0.612 |
| Donenberg, Wilson, Emerson, & Bryant (2002) | Females | 15.45 | Clinical | P | C, MSP, G | 169 | 0.633 |
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| St. Lawrence & Scott (1996) | 15.4 | Community | A | C | 249 | 0.211 | |
| Siahaan (2007) | Males | 18.04 | Community | A, M | MSP, G | 5374 | 0.038 |
| Siahaan (2007) | Females | 18.04 | Community | A, M | MSP, G | 5374 | 0.037 |
| Yen (2004) | 17.05 | Forensic | P | C, MSP | 87 | 0.045 | |
| Noell et al. (1993) | Males | 17 | Community | A, H | C, MSP | 56 | 0.226 |
| Noell et al. (1993) | Females | 17 | Community | A, H | C, MSP | 56 | 0.348 |
| Caspi et al. (1997) | 21 | Community | A | G | 154 | 0.394 | |
| Stein, Rotheram-Borus, Swendeman, & Millburn (2005) | 21.3 | Community | H, P | G | 248 | 0.341 | |
| Tho et al. (2007) | Males | 20.1 | Community | A | C, MSP | 880 | 0.348 |
| Tho et al. (2007) | Females | 20.1 | Community | A | C, MSP | 880 | 0.175 |
| Ku, Sonenstein, & Pleck (1993) | 19.5 | Community | P | C, MSP | 1389 | 0.095 | |
| Darling, Palmer, & Kipke (2005) | 18.8 | Community | P | MSP | 225–687 | 0.051 | |
| Barnes et al. (2007) | 16.5 | Community | P | C | 606 | 0.215 | |
| Goggin et al. (2002) | 15 | Community | A, M | C | 193 | 0.24 | |
| Fullilove et al. (1993) | Males | 17 | Community | P | C, MSP | 338 | 0.086 |
| Fullilove et al. (1993) | Females | 17 | Community | P | C, MSP | 0.143 | |
| Weimann & Berenson (1998) | Community | A | MSP | 199 | 0.397 | ||
| Chen & Yen (2011) | Community | P | C | 79 | 0.165 | ||
| Millburn et al. (2007) | 17.3 | Community | P | G | 896 | 0.77 | |
| Zapata et al. (2008) | Community | P | G | 15548 | 0.266 |
| Author Name | Subgroup | Mean Age | Sample Type | Type of drug | RSB definition | N | Effect Size |
|---|---|---|---|---|---|---|---|
| Lester et al. (2010) | 15.6 | Community | P | C | 264 | 0.13 | |
| Prinstein & La Greca (2004) | 16.82 | Community | A, M, H | C, MSP | 55 | 0.256 | |
| Gillmore, Butler, Lohr, & Gilchrist (1992) | 16 | Community | A, P | C, MSP, G | 214 | 0.298 | |
| Kraft & Rise (1991) | Males | 18.15 | Community | P | MSP | 1172 | 0.105 |
| Kraft & Rise (1991) | Females | 18.15 | Community | P | MSP | 1172 | 0.157 |
| Morris, Baker, Valentine, & Pennisi (1998) | 16 | Forensic | A, P | C, MSP | 1428–2354 | 0.21 | |
| Palen et al. (2006) | 14 | Community | A, H | C, MSP | 158–1155 | 0.014 |
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Abrantes AM, Strong DR, Ramsey SE, Kazura AN, Brown RA. HIV-risk behaviors among psychiatrically hospitalized adolescents with and without comorbid SUD. Journal of dual diagnosis. 2006;2(3):85–100. doi: 10.1300/J374v02n03_08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Substance Abuse Mental health Services Administration (SAMHSA) Office of applied studies, NSDUH series H–36, DHHS publication no. SMA 09–4434. Rockville, MD: SAMHSA; 2009. Results from the 2008 national survey on drug use and health: National findings. Retrieved June 6, 2011. Rockville, MD. [Google Scholar]
- 3.Babikian T, Freier M, Hopkins GL, DiClemente R, McBride D, Riggs M. An assessment of HIV/AIDS risk in higher education students in Yerevan, Armenia. AIDS and Behavior. 2004;8(1):47–61. doi: 10.1023/b:aibe.0000017525.92015.5d. [DOI] [PubMed] [Google Scholar]
- 4.Bachanas PJ, Morris MK, Lewis-Gess JK, et al. Psychological adjustment, substance use, HIV knowledge, and risky sexual behavior in at-risk minority females: Developmental differences during adolescence. Journal of Pediatric Psychology. 2002a;27:373–384. doi: 10.1093/jpepsy/27.4.373. [DOI] [PubMed] [Google Scholar]
- 5.Bachanas PJ, Morris MK, Lewis-Gess JK, et al. Predictors of risky sexual behavior in African American adolescent girls: Implications for prevention interventions. J Pediatr Psychol. 2002b;27(6):519–530. doi: 10.1093/jpepsy/27.6.519. [DOI] [PubMed] [Google Scholar]
- 6.Bailey SL, Gao W, Clark DB. Diary study of substance use and unsafe sex among adolescents with substance use disorders. Journal of Adolescent Health. 2006;38(3):297.e13–297.e20. doi: 10.1016/j.jadohealth.2004.12.001. [DOI] [PubMed] [Google Scholar]
- 7.Bailey S, Camlin C, Ennett S. Substance use and risky sexual behavior among homeless and runaway youth. Journal of Adolescent Health. 1998;23(6):378–388. doi: 10.1016/s1054-139x(98)00033-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baker DG, Mossman D. Potential HIV exposure in psychiatrically hospitalized adolescent girls. Am J Psychiatry. 1991;148(4):528–530. doi: 10.1176/ajp.148.4.528. [DOI] [PubMed] [Google Scholar]
- 9.Baliunas D, Rehm J, Irving H, Shuper P. Alcohol consumption and risk of incident human immunodeficiency virus infection: A meta-analysis. International Journal of Public Health. 2010;55:159–166. doi: 10.1007/s00038-009-0095-x. [DOI] [PubMed] [Google Scholar]
- 10.Barnes GM, Hoffman JH, Welte JW, Farrell MP, Dintcheff BA. Adolescents’ time use: Effects on substance use, delinquency and sexual activity. Journal of Youth and Adolescence. 2007;36(5):697–710. [Google Scholar]
- 11.Baskin-Sommers A, Sommers I. The co-occurrence of substance use and high-risk behaviors. Journal of Adolescent Health. 2006;38:609–611. doi: 10.1016/j.jadohealth.2005.07.010. [DOI] [PubMed] [Google Scholar]
- 12.Borenstein M, Hedges LV, Higgins J, Rothstein HR. Comprehensive Meta-Analysis 2.2 [Computer software] 2006. Comprehensive meta-Analysis 2.2 [computer software] [Google Scholar]
- 13.Brook DW, Brook JS, Pahl T, Montoya I. The longitudinal relationship between drug use and risky sexual behaviors among Colombian adolescents. Arch Pediatr Adolesc Med. 2002;156(11):1101–1107. doi: 10.1001/archpedi.156.11.1101. [DOI] [PubMed] [Google Scholar]
- 14.Brown JL, Vanable PA. Alcohol use, partner type, and risky sexual behavior among college students: Findings from an event-level study. Addictive Behaviors. 2007;32:2940–2952. doi: 10.1016/j.addbeh.2007.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Brown LK, Danovsky MB, Lourie KJ, DiClemente RJ, Ponton LE. Adolescents with psychiatric disorders and the risk for HIV. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36:1609–1617. doi: 10.1016/S0890-8567(09)66573-4. [DOI] [PubMed] [Google Scholar]
- 16.Bryan A, Ray LA, Copper ML. Alcohol use and protective sexual behaviors among high-risk adolescents. Journal of Studies on Alcohol and Drugs. 2007;68:327–335. doi: 10.15288/jsad.2007.68.327. [DOI] [PubMed] [Google Scholar]
- 17.Casey BJ, Getz S, Galvan A. The adolescent brain. Developmental Review. 2008;28:62–77. doi: 10.1016/j.dr.2007.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Caspi A, Begg D, Dickson N, et al. Personality differences predict health-risk behaviors in young adulthood: Evidence from a longitudinal study. J Pers Soc Psychol. 1997;73(5):1052–1063. doi: 10.1037//0022-3514.73.5.1052. [DOI] [PubMed] [Google Scholar]
- 19.Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Cottler LB, Bierut LJ. Number of sexual partners and associations with initiation and intensity of substance use. AIDS and Behavior. 2011;15:869–874. doi: 10.1007/s10461-010-9669-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Celentano DD, Valleroy LA, Sifakis F, et al. Associations between substance use and sexual risk among very young men who have sex with men. Sex Transm Dis. 2006;33(4):265–271. doi: 10.1097/01.olq.0000187207.10992.4e. [DOI] [PubMed] [Google Scholar]
- 21.Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Hawkins J, Lim C. Youth risk behavior surveillance-United States, 2011. MMWR Surveill Summ. 2012;61(4):1–162. [PubMed] [Google Scholar]
- 22.Centers for Disease Control and Prevention. Sexually transmitted disease surveillance, 2010. 2011. [Google Scholar]
- 23.Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: A critical period of addiction vulnerability. American Journal of Psychiatry. 2003;160:1041–1052. doi: 10.1176/appi.ajp.160.6.1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chan Y, Passetti LI, Garner BR, Lloyd JJ, Dennis ML. HIV risk behaviors: Risky sexual activities and needle use among adolescents in substance abuse treatment. AIDS and Behavior. 2011;15:114–124. doi: 10.1007/s10461-010-9702-3. [DOI] [PubMed] [Google Scholar]
- 25.Chen T, Yen C. Sexual intercourse experience and engagement in unprotected sex in adolescent MDMA users in Taiwan. Subst Use Misuse. 2011;46(4):398–403. doi: 10.3109/10826084.2010.501670. [DOI] [PubMed] [Google Scholar]
- 26.Cohen J. Psychological bulletin. Psychological Bulletin. 1992;112:37–46. [Google Scholar]
- 27.Cohen J. A coefficient of agreement for nominal scales. Educational and Psychological Measurement. 1960;60:37–46. [Google Scholar]
- 28.Connell CM, Gilreath TD, Hansen NB. A multiprocess latent class analysis of the co-occurrence of substance use and sexual risk behavior among adolescents. Journal of Studies on Alcohol and Drugs. 2009;70:943–951. doi: 10.15288/jsad.2009.70.943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cook RL, Comer DM, Wiesenfeld HC, et al. Alcohol and drug use and related disorders: An underrecognized health issue among adolescents and young adults attending sexually transmitted disease clinics. Sexually Transmitted Diseases. 2006;33:565–570. doi: 10.1097/01.olq.0000206422.40319.54. [DOI] [PubMed] [Google Scholar]
- 30.Cooper ML. Does drinking promote risky sexual behavior? A complex answer to a simple question. Current Directions in Psychological Science. 2006;15:19–23. [Google Scholar]
- 31.Crockett L, Raffaelli M, Shen Y. Linking self-regulation and risk proneness to risky sexual behavior: Pathways through peer pressure and early substance use. Journal of Research on Adolescence. 2006;16:503–525. [Google Scholar]
- 32.Crosby R, DiClemente RJ, Wingood GM, et al. Co-occurrence of intoxication during sex and sexually transmissible infections among young African American women: Does partner intoxication matter? Sexual Health. 2008;5:285–289. doi: 10.1071/sh07098. [DOI] [PubMed] [Google Scholar]
- 33.Da Ros CT, Schmitt CDS. Global epidemiology of sexually transmitted diseases. Asian Journal of Andrology. 2008;10:110–114. doi: 10.1111/j.1745-7262.2008.00367.x. [DOI] [PubMed] [Google Scholar]
- 34.Darling N, Palmer RF, Kipke MD. Do street youths’ perceptions of their caregivers predict HIV-risk behavior? Journal of Family Psychology. 2005;19:456–464. doi: 10.1037/0893-3200.19.3.456. [DOI] [PubMed] [Google Scholar]
- 35.Deas-Nesmith D, Brady KT, White R, Campbell S. HIV-risk behaviors in adolescent substance abusers. J Subst Abuse Treat. 1999;16(2):169–172. doi: 10.1016/s0740-5472(98)00040-3. [DOI] [PubMed] [Google Scholar]
- 36.DeCoster J. [Accessed August 19, 2010];Meta-analysis notes. http://www.stat-help.com/notes.html. Updated 2009.
- 37.DeCoster J, Iselin AR, Gallucci M. A conceptual and empirical examination of justifications for dichotomization. Psychological Methods. 2009;14:349–366. doi: 10.1037/a0016956. [DOI] [PubMed] [Google Scholar]
- 38.Dehne KL, Riedner G. Sexually transmitted infections among adolescents: The need for adequate health services. 2005. [DOI] [PubMed] [Google Scholar]
- 39.Dehne KL, Riedner G. Adolescence: A dynamic concept. Reproduction Health Matters. 2001;9:11–15. doi: 10.1016/s0968-8080(01)90003-5. [DOI] [PubMed] [Google Scholar]
- 40.Diane M, Mary M, Gillmore R, et al. Adolescent drinking and sex: Findings from a daily diary study. Perspectives on Sexual and Reproductive Health. 2003;35(4):162–168. doi: 10.1363/psrh.35.162.03. [DOI] [PubMed] [Google Scholar]
- 41.DiClemente RJ, Wingood GM, Crosby RA, et al. Sexual risk behaviors associated with having older sex partners: A study of black adolescent females. Sex Transm Dis. 2002;29(1):20–24. doi: 10.1097/00007435-200201000-00004. [DOI] [PubMed] [Google Scholar]
- 42.Donenberg GR, Emerson E, Bryant FB, King S. Does substance use moderate the effects of parents and peers on risky sexual behaviour. AIDS Care. 2006;18:194–200. doi: 10.1080/09540120500456391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Donenberg GR, Emerson E, Bryant FB, Wilson H, Weber-Shifrin E. Understanding AIDS-risk behavior among adolescents in psychiatric care: Links to psychopathology and peer relationships. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40(6):642–653. doi: 10.1097/00004583-200106000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Donovan C, McEwan RT. A review of the literature examining the relationship between alcohol use and HIV-related sexual risk-taking in young people. Addiction. 1995;90:319–328. doi: 10.1046/j.1360-0443.1995.9033192.x. [DOI] [PubMed] [Google Scholar]
- 45.Donovan JE, Jessor R, Costa FM. Syndrome of problem behavior in adolescence: A replication. Journal of Consulting and Clinical Psychology. 1988;56:762–765. doi: 10.1037//0022-006x.56.5.762. [DOI] [PubMed] [Google Scholar]
- 46.Duncan SC, Strycker LA, Duncan TE. Exploring associations in developmental trends of adolescent substance use and risky sexual behavior in a high-risk population. J Behav Med. 1999;22(1):21–34. doi: 10.1023/a:1018795417956. [DOI] [PubMed] [Google Scholar]
- 47.Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(455):463. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- 48.Ellickson PL, Collins RL, Bogart LM, Klein DJ, Taylor SL. Scope of HIV risk and co-occuring psychosocial health problems among young adults: Violence, victimization, and substance use. Journal of Adolescent Health. 2005;36:401–409. doi: 10.1016/j.jadohealth.2004.06.008. [DOI] [PubMed] [Google Scholar]
- 49.Fleiss JL, Cohen J. The equivalence of weighted kappa and the intraclass correlation coefficient as measures of reliability. Educational and Psychological Measurement. 1973;33:613–619. [Google Scholar]
- 50.Fullilove MT, Golden E, Fullilove RE, III, et al. Crack cocaine use and high-risk behaviors among sexually active black adolescents. Journal of Adolescent Health. 1993;14(4):295–300. doi: 10.1016/1054-139x(93)90177-q. [DOI] [PubMed] [Google Scholar]
- 51.Gleghorn AA, Marx R, Vittinghoff E, Katz MH. Association between drug use patterns and HIV risks among homeless, runaway, and street youth in northern California. Drug Alcohol Depend. 1998;51(3):219–227. doi: 10.1016/s0376-8716(98)00042-8. [DOI] [PubMed] [Google Scholar]
- 52.Goggin K, Metcalf K, Kennedy S, et al. Unpublished manuscript. 2002. HIV risk and substance use behaviors among African American youth. [Google Scholar]
- 53.Gogtay N, Giedd J, Rapoport JL. Brain development in healthy, hyperactive, and psychotic children. Archieves of Neurology. 2002;59:1244–1248. doi: 10.1001/archneur.59.8.1244. [DOI] [PubMed] [Google Scholar]
- 54.Gómez MA, Sola A, Cortés MJ, Mira JJ. Sexual behaviour and contraception in people under the age of 20 in Alicante, Spain. European J of Contraception and Reproductive Healthcare. 2007;12(2):125–130. doi: 10.1080/13625180701330555. [DOI] [PubMed] [Google Scholar]
- 55.Griffin JA, Umstattd MR, Usdan SL. Alcohol use and high-risk sexual behavior among collegiate women: A review of research on alcohol myopia theory. Journal of American College Health. 2010;58:523–532. doi: 10.1080/07448481003621718. [DOI] [PubMed] [Google Scholar]
- 56.Grossbard JR, Lee CM, Neighbors C, Hendershot CS, Larimer ME. Alcohol and risky sex in athletes and nonathletes: What roles do sex motives play? Journal of studies on alcohol and drugs. 2007;68(4):566–574. doi: 10.15288/jsad.2007.68.566. [DOI] [PubMed] [Google Scholar]
- 57.Guo J, Chung I, Hill KG, Hawkins JD, Catalano RF, Abbott RD. Developmental relationships between adolescent substance use and risky sexual behavior in young adulthood. Journal of Adolescent Health. 2002;31(4):354–362. doi: 10.1016/s1054-139x(02)00402-0. [DOI] [PubMed] [Google Scholar]
- 58.Hallfors D, Vevea JL, Iritani B, Cho H, Khatapoush S, Saxe L. Truancy, grade point average, and sexual activity: A meta-analysis of risk indicators for youth substance use. Journal of School Health. 2002;72:205–211. doi: 10.1111/j.1746-1561.2002.tb06548.x. [DOI] [PubMed] [Google Scholar]
- 59.Halpern-Felsher BL, Millstein SG, Ellen JM. Relationship of alcohol use and risky sexual behavior: A review and analysis of findings. Journal of American College Health. 1996;19:331–336. doi: 10.1016/S1054-139X(96)00024-9. [DOI] [PubMed] [Google Scholar]
- 60.Hedges LV, Vevea JL. Fixed- and random-effects models in meta-analysis. Psychological Bulletin. 1998;3:486–504. [Google Scholar]
- 61.Hedges LV, Olkin I. Statistical methods for Meta-analysis. Orlando: Academic Press; 1985. [Google Scholar]
- 62.Heffernan R, Chiasson MA, Sackoff JE. HIV risk behaviors among adolescents at a sexually transmitted disease clinic in New York City. Journal of adolescent health. 1996;18(6):429–434. doi: 10.1016/1054-139X(95)00277-Y. [DOI] [PubMed] [Google Scholar]
- 63.Hemphill JF. Interpreting the magnitudes of correlation coefficients. American Psychologist. 2003;58:78–80. doi: 10.1037/0003-066x.58.1.78. [DOI] [PubMed] [Google Scholar]
- 64.Hendershot CS, Magnan RE, Bryan AD. Associations of marijuana use and sex-related marijuana expectancies with HIV/STD risk behavior in high-risk adolescents. Psychology of Addictive Behaviors. 2010;24(3):404–414. doi: 10.1037/a0019844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hingson RW, Strunin L, Berlin BM, Heeren T. Beliefs about AIDS, use of alcohol and drugs, and unprotected sex among Massachusetts adolescents. Am J Public Health. 1990;80(3):295–299. doi: 10.2105/ajph.80.3.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hoffman S, O’Sullivan LF, Harrison A, Dolezal C, Monroe-Wise A. HIV risk behaviors and the context of sexual coercion in young adults’ sexual interactions: Results from a diary study in rural South Africa. Sex Transm Dis. 2006;33(1):52–58. doi: 10.1097/01.olq.0000187198.77612.d8. [DOI] [PubMed] [Google Scholar]
- 67.Hou S, Basen-Engquist K. Human immunodeficiency virus risk behavior among white and Asian/Pacific islander high school students in the United States: Does culture make a difference? Journal of Adolescent Health. 1997;20(1):68–74. doi: 10.1016/S1054-139X(96)00323-0. [DOI] [PubMed] [Google Scholar]
- 68.Jackson C, Geddes R, Haw S, Frank J. Interventions to prevent substance use and risky sexual behaviour in young people: A systematic review. Addiction. 2012;107:733–747. doi: 10.1111/j.1360-0443.2011.03751.x. [DOI] [PubMed] [Google Scholar]
- 69.Johnson BT. DSTAT 1.10: Software for the meta-analytic review of research literatures [computer software] 1993. [Google Scholar]
- 70.Kebede D, Alem A, Mitike G, et al. Khat and alcohol use and risky sex behaviour among in-school and out-of-school youth in Ethiopia. BMC Public Health. 2005;5(1):109. doi: 10.1186/1471-2458-5-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Khan MR, Berger AT, Wells BE, Cleland CM. Longitudinal associations between adolescent alcohol use and adulthood sexual risk behavior and sexually transmitted infection in the United States: Assessment of differences by race. American Journal of Public Health. 2012;102:867–876. doi: 10.2105/AJPH.2011.300373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Khasakhala AA, Mturi AJ, Naar-King S, et al. Factors associated with risky sexual behaviour among out-of-school youth in Kenya. J Biosoc Sci. 2008;50(5):641–653. doi: 10.1017/S0021932007002647. [DOI] [PubMed] [Google Scholar]
- 73.Kingree JB, Betz H. Risky sexual behavior in relation to marijuana and alcohol use among African–American, male adolescent detainees and their female partners. Drug Alcohol Depend. 2003;72(2):197–203. doi: 10.1016/s0376-8716(03)00196-0. [DOI] [PubMed] [Google Scholar]
- 74.Kingree J, Phan D. Marijuana use and unprotected sexual intercourse among adolescent detainees an event analysis. Crim Justice Behav. 2002;29(6):705–717. [Google Scholar]
- 75.Koniak-Griffin D, Brecht M. Linkages between sexual risk taking, substance use, and AIDS knowledge among pregnant adolescents and young mothers. Nurs Res. 1995;44(6):340–346. [PubMed] [Google Scholar]
- 76.Koopman C, Rosario M, Rotheram-Borus MJ. Alcohol and drug use and sexual behaviors placing runaways at risk for HIV infection. Addict Behav. 1994;19(1):95–103. doi: 10.1016/0306-4603(94)90055-8. [DOI] [PubMed] [Google Scholar]
- 77.Kraft P, Rise J. Contraceptive behaviour of Norwegian adolescents. Health Educ Res. 1991;6(4):431–441. doi: 10.1093/her/6.4.431. [DOI] [PubMed] [Google Scholar]
- 78.Kraft P, Rise J, Træen B. The HIV epidemic and changes in the use of contraception among Norwegian adolescents. AIDS. 1990;4(7):673–678. doi: 10.1097/00002030-199007000-00011. [DOI] [PubMed] [Google Scholar]
- 79.Ku L, Sonenstein FL, Pleck JH. Young men’s risk behaviors for HIV infection and sexually transmitted diseases, 1988 through 1991. Am J Public Health. 1993;83(11):1609–1615. doi: 10.2105/ajph.83.11.1609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lawrence JS, Scott CP. Examination of the relationship between African American adolescents’ condom use at sexual onset and later sexual behavior: Implications for condom distribution programs. AIDS Educ Prev. 1996;8(3):258–266. [PubMed] [Google Scholar]
- 81.Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to HIV: Issues in methodology, interpretation, and prevention. Am Psychol. 1993;48(10):1035. doi: 10.1037//0003-066x.48.10.1035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Leigh BC, Vanslyke JG, Hoppe MJ, Rainey DT, Morrison DM, Gillmore MR. Drinking and condom use: Results from an event-based daily diary. AIDS and Behavior. 2008;12(1):104–112. doi: 10.1007/s10461-007-9216-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Lester P, Stein JA, Bursch B, et al. Family-based processes associated with adolescent distress, substance use and risky sexual behavior in families affected by maternal HIV. Journal of Clinical Child & Adolescent Psychology. 2010;39(3):328–340. doi: 10.1080/15374411003691677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Lipsey MW, Wilson DB. Practical meta-analysis. In: Bickman L, Rog D, editors. Applied social research methods series. Vol. 49. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- 85.Lowry R, Holtzman D, Truman BI, Kann L, Collins JL, Kolbe LJ. Substance use and HIV-related sexual behaviors among US high school students: Are they related? Am J Public Health. 1994;84(7):1116–1120. doi: 10.2105/ajph.84.7.1116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.MacKellar DA, Valleroy LA, Hoffmann JP, et al. Gender differences in sexual behaviors and factors associated with nonuse of condoms among homeless and runaway youths. AIDS education and prevention. 2000;12(6):477–491. [PubMed] [Google Scholar]
- 87.Madkour AS, Farhat T, Halpern CT, Godeau E, Gabhainn SN. Early adolescent sexual initiation as a problem behavior: A comparative study of five nations. Journal of Adolescent Health. 2010;47(4):389–398. doi: 10.1016/j.jadohealth.2010.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Martinez G, Copen CE, Abma JC. Teenagers in the United States: Sexual activity, contraceptive use, and childbearing, 2006–2010 national survey of family growth. Vital Health Stat. 2011;23(31):1–35. [PubMed] [Google Scholar]
- 89.Matthews AK, Cho YI, Hughes T, Wilsnack SC, Johnson T, Martin K. The relationships of sexual identity, hazardous drinking, and drinking expectancies with risky sexual behaviors in a community sample of lesbian and bisexual women. J Am Psychiatr Nurses Assoc. 2013;19(5):259–270. doi: 10.1177/1078390313505644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Mbulo L. Alcohol use and alcohol-sexual expectations as risk factors for HIV/AIDS among young people in Zambia. Lincoln, NE: University of Nebraska; 2005. [Google Scholar]
- 91.McNall M, Remafedi G. Relationship of amphetamine and other substance use to unprotected intercourse among young men who have sex with men. Arch Pediatr Adolesc Med. 1999;153(11):1130–1135. doi: 10.1001/archpedi.153.11.1130. [DOI] [PubMed] [Google Scholar]
- 92.Milburn NG, Stein JA, Rice E, et al. AIDS risk behaviors among American and Australian homeless youth. J Soc Iss. 2007;63(3):543–565. [Google Scholar]
- 93.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi: 10.7326/0003-4819-151-4-200908180-00135. [DOI] [PubMed] [Google Scholar]
- 94.Morris RE, Baker CJ, Valentine M, Pennisi AJ. Variations in HIV risk behaviors of incarcerated juveniles during a four-year period: 1989–1992. Journal of Adolescent Health. 1998;23(1):39–48. doi: 10.1016/s1054-139x(97)00268-1. [DOI] [PubMed] [Google Scholar]
- 95.Morrison-Beedy D, Carey MP, Feng C, Tu XM. Predicting sexual risk behaviors among adolescent and young women using a prospective diary method. Res Nurs Health. 2008;31(4):329–340. doi: 10.1002/nur.20263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Mpofu E, Bility K, Flisher AJ, Onya H, Lombard C. Correlates of drug use in rural Africa: Drug/substance use and sexual behaviour in Mankweng district, South Africa. Journal of Psychology in Africa. 2005;15(1):11–15. [Google Scholar]
- 97.Mpofu E, Flisher AJ, Bility K, Onya H, Lombard C. Sexual partners in a rural South African setting 1. AIDS and Behavior. 2006;10(4):399–404. doi: 10.1007/s10461-005-9037-7. [DOI] [PubMed] [Google Scholar]
- 98.Naff Johnson C. Independent and interactive effects of personality and alcohol use on AIDS-related risky sexual behavior. Newark, DE: University of Delaware; 1996. [Google Scholar]
- 99.Newcomb ME, Clerkin EM, Mustanski B. Sensation seeking moderates the effects of alcohol and drug use prior to sex on sexual risk in young men who have sex with men. AIDS and Behavior. 2011;15(3):565–575. doi: 10.1007/s10461-010-9832-7. [DOI] [PubMed] [Google Scholar]
- 100.Noell J, Biglan A, Berendt J, Ochs L. Problematic sexual situations for adolescents: Alcohol and unsafe sex. Health Values: The Journal of Health Behavior, Education & Promotion. 1993;17:40–49. [Google Scholar]
- 101.Palen L, Smith EA, Flisher AJ, Caldwell LL, Mpofu E. Substance use and sexual risk behavior among south african eighth grade students. Journal of Adolescent Health. 2006;39(5):761–763. doi: 10.1016/j.jadohealth.2006.04.016. [DOI] [PubMed] [Google Scholar]
- 102.Poulin C, Graham L. The association between substance use, unplanned sexual intercourse and other sexual behaviours among adolescent students. Addiction. 2001;96(4):607–621. doi: 10.1046/j.1360-0443.2001.9646079.x. [DOI] [PubMed] [Google Scholar]
- 103.Prinstein MJ, La Greca AM. Childhood peer rejection and aggression as predictors of adolescent girls’ externalizing and health risk behaviors: A 6-year longitudinal study. J Consult Clin Psychol. 2004;72(1):103. doi: 10.1037/0022-006X.72.1.103. [DOI] [PubMed] [Google Scholar]
- 104.Pritchard C, Cox M. Comparison of problematic behaviours of 10th and 11th year southern English adolescents in 1985 and 2005. Part 1: Trends in gender behaviour. Int J Adolesc Med Health. 2007;19(2):127–140. doi: 10.1515/ijamh.2007.19.2.127. [DOI] [PubMed] [Google Scholar]
- 105.Ramrakha S, Caspi A, Dickson N, Moffitt TE, Paul C. Psychiatric disorders and risky sexual behaviour in young adulthood: Cross sectional study in birth cohort. BMJ. 2000;321(7256):263–266. doi: 10.1136/bmj.321.7256.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Rawson RA, Washton A, Domier CP, Reiber C. Drugs and sexual effects: Role of drug type and gender. J Subst Abuse Treat. 2002;22(2):103–108. doi: 10.1016/s0740-5472(01)00215-x. [DOI] [PubMed] [Google Scholar]
- 107.Refaat A. Practice and awareness of health risk behaviour among Egyptian university students. Eastern Mediterranean Health Journal. 2004;10(1/2):72–81. [PubMed] [Google Scholar]
- 108.Reid H, Koopman C. Predicting patterns of sexual acts among homosexual and bisexual youths. Am J Psychiatry. 1995;1(52):589–595. doi: 10.1176/ajp.152.4.588. [DOI] [PubMed] [Google Scholar]
- 109.Remafedi G. Predictors of unprotected intercourse, among gay and bisexual youth: Knowledge, beliefs, and behavior. Pediatrics. 1994;94(2):163–168. [PubMed] [Google Scholar]
- 110.Reyna VF, Farley F. Risk and rationality in adolescent decision making implications for theory, practice, and public policy. Psychological science in the public interest. 2006;7(1):1–44. doi: 10.1111/j.1529-1006.2006.00026.x. [DOI] [PubMed] [Google Scholar]
- 111.Richter DL, Valois RF, McKeown RE, Vincent ML. Correlates of condom use and number of sexual partners among high school adolescents. J Sch Health. 1993;63(2):91–97. doi: 10.1111/j.1746-1561.1993.tb06087.x. [DOI] [PubMed] [Google Scholar]
- 112.Riggs NR, Greenberg MT. Neurocognition as a moderator and mediator in adolescent substance misuse prevention. Am J Drug Alcohol Abuse. 2009;35(4):209–213. doi: 10.1080/00952990903005940. [DOI] [PubMed] [Google Scholar]
- 113.Robbins RN, Bryan A. Relationships between future orientation, impulsive sensation seeking, and risk behavior among adjudicated adolescents. J Adolesc Res. 2004;19(4):428–445. doi: 10.1177/0743558403258860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Roberts ST, Kennedy BL. Why are young college women not using condoms? Their perceived risk, drug use, and developmental vulnerability may provide important clues to sexual risk. Arch Psychiatr Nurs. 2006;20(1):32–40. doi: 10.1016/j.apnu.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 115.Rotheram-Borus MJ, Rosario M, Meyer-Bahlburg HF, Koopman C, Dopkins SC, Davies M. Sexual and substance use acts of gay and bisexual male adolescents in New York City. J Sex Res. 1994;31(1):47–57. [Google Scholar]
- 116.Rotheram-Borus M, Mann T, Chabon B. Amphetamine use and its correlates among youths living with HIV. AIDS Education and Prevention. 1999;11(3):232–242. [PubMed] [Google Scholar]
- 117.Sales JM, Brown JL, Vissman AT, DiClemente RJ. The association between alcohol use and sexual risk behaviors among African American women across three developmental periods: A review. Curr Drug Abuse Rev. 2012;5(2):117–128. doi: 10.2174/1874473711205020117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Sawyer SM, Afifi RA, Bearinger LH, et al. Adolescence: A foundation for future health. The Lancet. 2012;379(9826):1630–1640. doi: 10.1016/S0140-6736(12)60072-5. [DOI] [PubMed] [Google Scholar]
- 119.Schuster RM, Mermelstein R, Wakschlag L. Gender-specific relationships between depressive symptoms, marijuana use, parental communication and risky sexual behavior in adolescence. Journal of Youth and Adolescence. 2012:1–16. doi: 10.1007/s10964-012-9809-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Schwartz SJ, Unger JB, Rosiers SED, et al. Substance use and sexual behavior among recent Hispanic immigrant adolescents: Effects of parent–adolescent differential acculturation and communication. Drug Alcohol Depend. 2012;125:S26–S34. doi: 10.1016/j.drugalcdep.2012.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Scivoletto S, Tsuji RK, Najjar Abdo CH, de Queiroz S, de Andrade AG, Gattaz WF. Use of psychoactive substances and sexual risk behavior in adolescents. Subst Use Misuse. 2002;37(3):381–398. doi: 10.1081/ja-120002484. [DOI] [PubMed] [Google Scholar]
- 122.Shrier LA, Schillinger JA, Aneja P, et al. Depressive symptoms and sexual risk behavior in young, chlamydia-infected, heterosexual dyads. Journal of Adolescent health. 2009;45(1):63–69. doi: 10.1016/j.jadohealth.2008.11.016. [DOI] [PubMed] [Google Scholar]
- 123.Shuper PA, Neuman M, Kanteres F, Baliunas D, Joharchi N, Rehm J. Causal considerations on alcohol and HIV/AIDS—a systematic review. Alcohol and alcoholism. 2010;45(2):159–166. doi: 10.1093/alcalc/agp091. [DOI] [PubMed] [Google Scholar]
- 124.Siahaan F. An exploration of the relationship between risky sexual behavior and substance use by teenagers and young adults. New York: City University of New York; 2006. [Google Scholar]
- 125.Smith CD, Brown JM. Sexual behaviors, extroversion, and alcohol use among college students. J Alcohol Drug Educ. 1998;44(1):70–79. [Google Scholar]
- 126.Steele CM, Josephs RA. Alcohol myopia: Its prized and dangerous effects. Am Psychol. 1990;45(8):921. doi: 10.1037//0003-066x.45.8.921. [DOI] [PubMed] [Google Scholar]
- 127.Steinberg L. A social neuroscience perspective on adolescent risk-taking. Developmental Review. 2008;28(1):78–106. doi: 10.1016/j.dr.2007.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Strunin L, Hingson R. Alcohol, drugs, and adolescent sexual behavior. Subst Use Misuse. 1992;27(2):129–146. doi: 10.3109/10826089209068734. [DOI] [PubMed] [Google Scholar]
- 129.Swartzendruber A, Sales J, Brown J, DiClemente R, Rose E. P3. 001 patterns of recent alcohol and marijuana use as predictors of condom use, pregnancy and sexually transmitted infections during 18-months of follow-up among African-American female adolescents. Sex Transm Infect. 2013;89(Suppl 1):A148–A148. [Google Scholar]
- 130.Tho LH, Singhasivanon P, Kaewkungwal J, Kaljee LM, Charoenkul C. Sexual behaviors of alcohol drinkers and non-drinkers among adolescents and young adults in Nha. Trang, Vietnam. 2007;38:152–160. [PubMed] [Google Scholar]
- 131.Thompson J, RG . Mental health problems, co-occurring substance use, and HIV risk behaviors among adolescents in foster care. Missouri: Washington University; 2003. [Google Scholar]
- 132.Tubman JG, Langer LM. “About last night”: The social ecology of sexual behavior relative to alcohol use among adolescents and young adults in substance abuse treatment. J Subst Abuse. 1995;7(4):449–461. doi: 10.1016/0899-3289(95)90015-2. [DOI] [PubMed] [Google Scholar]
- 133.Tucker JS, Ryan GW, Golinelli D, et al. Substance use and other risk factors for unprotected sex: Results from an event-based study of homeless youth. AIDS and Behavior. 2012;16(6):1699–1707. doi: 10.1007/s10461-011-0017-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Twa-Twa J, Oketcho S, Siziya S, Muula A. Prevalence and correlates of condom use at last sexual intercourse among in-school adolescents in urban areas of Uganda. East Afr J Public Health. 2008;5:22–25. doi: 10.4314/eajph.v5i1.38972. [DOI] [PubMed] [Google Scholar]
- 135.Valente T, Bharath U. An evaluation of the use of drama to communicate HIV/AIDS information. AIDS Education and Prevention. 1999;11(3):203–211. [PubMed] [Google Scholar]
- 136.Valera P, Epperson M, Daniels J, Ramaswamy M, Freudenberg N. Substance use and HIV-risk behaviors among young men involved in the criminal justice system. Am J Drug Alcohol Abuse. 2009;35(1):43–47. doi: 10.1080/00952990802342923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Van Rie A, Sengupta S, Pungrassami P, et al. Measuring stigma associated with tuberculosis and HIV/AIDS in southern Thailand: Exploratory and confirmatory factor analyses of two new scales. Tropical Medicine and International Health. 2008;13:21–30. doi: 10.1111/j.1365-3156.2007.01971.x. [DOI] [PubMed] [Google Scholar]
- 138.Vanoss Marín B, Coyle KK, Gómez CA, Carvajal SC, Kirby DB. Older boyfriends and girlfriends increase risk of sexual initiation in young adolescents. Journal of Adolescent Health. 2000;27(6):409–418. doi: 10.1016/s1054-139x(00)00097-5. [DOI] [PubMed] [Google Scholar]
- 139.Voisin DR, Crosby R, Yarber WL, Salazar LF, DiClemente RJ, Staples-Horne M. Witnessing community violence and Health-Risk behaviors among detained adolescents. Am J Orthopsychiatry. 2007;77(4):506–513. doi: 10.1037/0002-9432.77.4.506. [DOI] [PubMed] [Google Scholar]
- 140.Wallerstein N, Bernstein E. Empowerment education: Freire’s ideas adapted to health education. Health Education and Behavior. 1988;15(4):379–394. doi: 10.1177/109019818801500402. [DOI] [PubMed] [Google Scholar]
- 141.Wang C, Burris MA. Photovoice: Concept, methodology, and use for participatory needs. Health Education and Behavior. 1997;24(3):369–387. doi: 10.1177/109019819702400309. [DOI] [PubMed] [Google Scholar]
- 142.Wang C, Burris MA. Empowerment through photo novella: Portraits of participation. Health Education and Behavior. 1994;21(2):171–186. doi: 10.1177/109019819402100204. [DOI] [PubMed] [Google Scholar]
- 143.Wechsler H, Dowdall GW, Davenport A, Rimm EB. A gender-specific measure of binge drinking among college students. Am J Public Health. 1995;85(7):982–985. doi: 10.2105/ajph.85.7.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Weinstock H, Berman S, Cates W. Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspectives on sexual and reproductive health. 2004;36(1):6–10. doi: 10.1363/psrh.36.6.04. [DOI] [PubMed] [Google Scholar]
- 145.White House Office of National AIDS Policy. [Accessed October 24];National HIV/AIDS strategy for the United States. 2010 2013 [Google Scholar]
- 146.Wiemann, Constance M, Berenson MDAB. Factors associated with recent and discontinued alcohol use by pregnant adolescents. Journal of Adolescent Health. 1998;22(5):417–423. doi: 10.1016/s1054-139x(97)00215-2. [DOI] [PubMed] [Google Scholar]
- 147.Wislar JS, Fendrich M. Can self-reported drug use data be used to assess sex risk behavior in adolescents? Arch Sex Behav. 2000;29(1):77–89. doi: 10.1023/a:1001838605520. [DOI] [PubMed] [Google Scholar]
- 148.World Health Organization. [Accessed November 13, 2013];Sexually transmitted diseases. http://www.who.int/mediacentre/factsheets/fs110/en/index.html.
- 149.Yan AF, Chiu Y, Stoesen CA, Wang MQ. STD-/HIV-related sexual risk behaviors and substance use among US rural adolescents. J Natl Med Assoc. 2007;99(12):1386. [PMC free article] [PubMed] [Google Scholar]
- 150.Yen C. Relationship between methamphetamine use and risky sexual behavior in adolescents. Kaohsiung J Med Sci. 2004;20(4):160–165. doi: 10.1016/S1607-551X(09)70101-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Yonas MA, Burke JG, Rak K, Bennet AVK, Gielen AC. A Picture’s worth a thousand words: Engaging youth in CBPR using the creative arts. Progress in Community Health Partnerships: Research, Education, and Action. 2009;3(4):349–358. doi: 10.1353/cpr.0.0090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Zapata LB, Hillis SD, Marchbanks PA, Curtis KM, Lowry R. Methamphetamine use is independently associated with recent risky sexual behaviors and adolescent pregnancy. J Sch Health. 2008;78(12):641–648. doi: 10.1111/j.1746-1561.2008.00360.x. [DOI] [PubMed] [Google Scholar]