

Abstract
Porokeratotic eccrine ostial and dermal duct nevus (PEODDN) is a rare nevoid condition characterized by asymptomatic grouped keratotic papules and plaques with a linear pattern on the extremities, having distinct porokeratotic histopathological features. The lesions usually present at birth or in childhood. We present here a case of late-onset PEODDN in a 23-year-old man who had lesions on the palm, forearm, arm and the chest along the lines of Blaschko, strictly localized to the left side of the body.
Keywords: Blaschko's lines, nevus, porokeratotic
INTRODUCTION
Porokeratotic eccrine ostial and dermal ductal nevus (PEODDN) is a rare benign nevoid disorder characterized by porokeratotic histopathologic features. Believed to be an eccrine hamartoma, this disorder of keratinization usually presents at birth or during childhood with multiple punctate or keratotic papules localized to the extremities. The lesions usually display linear distribution along the Blaschko's lines.[1] Involvement of the palms and soles is characteristic, and lesions are often systematized.[2] Lesions are usually persistent and grow as the patient grows up.[3] Not more than 50 cases of this disorder have been reported in the English literature (PubMed search) till date. We report a case of adult-onset widespread unilateral PEODDN along the lines of Blaschko for its rarity.
CASE REPORT
A 23-year-old otherwise-healthy young man presented with multiple elevated skin lesions on his left upper extremity and upper chest for five years. Lesions initially appeared on the left palm as multiple horny elevations and subsequently developed over the entire left upper extremity and left side of the chest in a linear fashion. The condition was stable for three years. The lesions were accompanied by mild itching. Past and family medical history were unremarkable. The patient had consulted several physicians and applied various topical medications without any benefit.
Clinical examination revealed skin-colored to brownish, discrete, verrucous papules, nodules, and plaques in a linear configuration following Blaschko's lines distributed over the left forearm, arm, and the left side of the upper chest strictly respecting the midline [Figures 1 and 2]. There were depigmented macules and scars along the lateral border of the forearm, reportedly owing to burns sustained a few months previously. There were multiple small keratotic and pitted papules linearly arranged along the medial border and central part of the palm [Figure 3]. A few of the palmar lesions had coalesced to form plaques. Apart from these keratotic papules, numerous punctate pits were also visualized over the palm. The rest of the mucocutaneous and systemic examination was within normal limits. Routine laboratory tests, serum chemistry panel and human immunodeficiency virus serology were normal.
Figure 1.

Verrucous papules and nodules on the upper extremity and upper chest along the lines of Blaschko
Figure 2.

Close-up view showing papulonodular lesions along the Blaschko's lines on the chest and upper arm
Figure 3.

Punctate pits and pitted papules, linearly arranged on the central portion and lateral border of the left palm
We considered linear lichen planus, nevus comedonicus and PEODDN as differentials and skin biopsy specimens were obtained. Histopathology showed hyperkeratosis, acanthosis and papillomatosis and no dermal infiltrate. Cornoid lamella-like columns of parakeratosis were seen invaginating the epidermis. Granular layer were absent beneath these columns [Figures 4 and 5]. Dilated acrosyringia were however not visualized in the sections examined. The absence of interface dermatitis ruled out lichen planus. Nevus comedonicus was excluded by the absence of grouped undeveloped hair follicles filled with cornified debris devoid of hair shafts. Linear porokeratosis was not included in the differentials as the patient did not have the characteristic plaques with furrowed borders. Based on the distinct clinical findings corroborated by the histology, the case was diagnosed as PEODDN and the patient was referred for ablative laser therapy.
Figure 4.
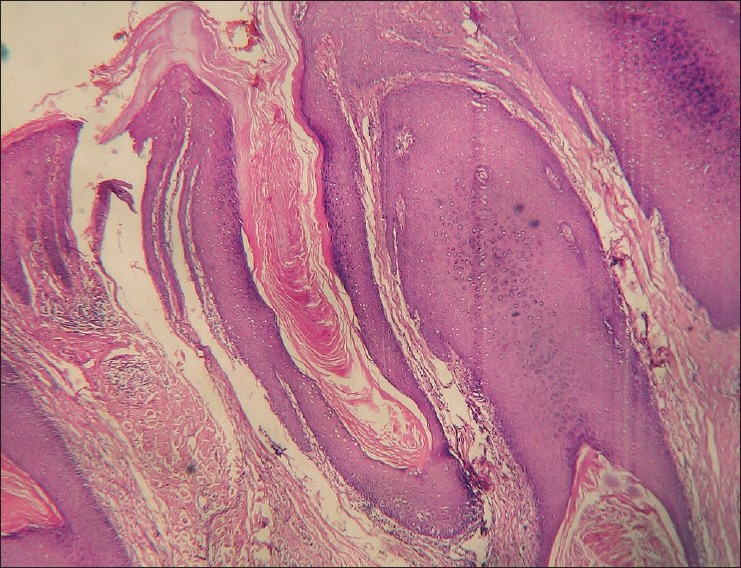
Broad parakeratotic column occupying an epidermal invagination beneath which the granular layer is absent (H and E, ×100)
Figure 5.
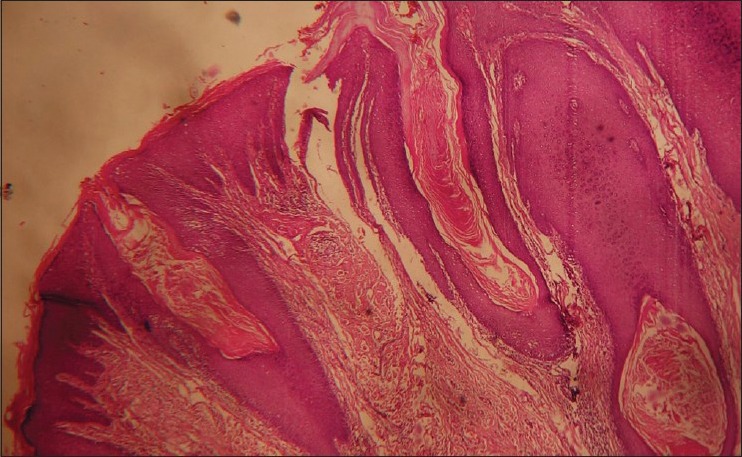
Multiple cornoid lamella-like keratotic invaginations of the epidermis (H and E, ×50)
DISCUSSION
Porokeratotic eccrine ostial and dermal duct nevus was first described by Marsden et al. in 1979 as “comedo nevus of the palm.”[4] The condition owes its present name to Abell and Read who described a linear nevus located on foot in 1980.[5] The pathogenesis of the disease is unclear. Studies point toward genetic mosaicism and a possible eccrine or circumscribed epidermal abnormality of keratinization as the putative pathomechanism of the entity.[6] Recent findings indicate that PEODDN may be a mosaic form of keratitis ichthyosis deafness (KID) syndrome and is caused by somatic mutation in GJB2 encoding a gap junction protein connexin-26.[7]
The lesions are commonly present at birth or in childhood, although cases of adult-onset PEODDN have been described. A review of the literature by Valks et al. however showed that the frequency of late onset disease may be as high as 26%.[8] Gender distribution is nearly equal. The lesions are asymptomatic or mildly pruritic and predominantly occur on the palms and soles as linear punctate pits or pitted papules. Elsewhere, they consist of multiple verrucous, keratotic, brown to flesh-colored papules often coalescing into linear plaques. The lesions follow the Blaschko lines and may be systematized.[2] Several case reports have described PEODDN associated with conditions such as hyperthyroidism and sensory polyneuropathy, breast hypoplasia, Bowen disease, deafness and development delay, seizure disorder, hemiparesis, scoliosis, alopecia, onychodysplasia, and squamous cell carcinoma.[9]
Depending on the morphology, extent and patterns of involvement, the clinical differentials of PEODDN may include nevus comedonicus, linear verrucous epidermal nevus, inflammatory linear verrucous epidermal nevus (ILVEN), linear psoriasis, linear porokeratosis, dilated pore nevus, linear lichen planus, punctate palmoplantar keratoderma, and punctate porokeratosis. The condition can be differentiated from ILVEN by the absence of extremely pruritic bands of eczematous or psoriasiform lesions and the presence of pitted papules and punctate pits on palms and/or soles. Histological features, however, can discriminate the clinical differentials. Characteristic histopathological features of PEODDN include orthokeratosis, and a column of parakeratosis occupying an invagination of the epidermis, which, at the base of the column shows loss of granular cells.[8] Dilated acrosyringia at the base of the invaginations point to an eccrine origin. However, demonstration of an anatomic relationship between the porokeratotic columns and the underlying acrosyringeal duct may be barely visible.[3] There may be histologic involvement of acrotrichia and based on the observation of overlapping histologic features, the name “porokeratotic adnexal ostial nevus” was proposed to incorporate PEODDN and porokeratotic eccrine and hair follicle nevus.[1]
The course of PEODDN is usually stationary or sometimes progressive. Long term involution of the lesions has been observed rarely.[10] The lesions are benign and no malignant transformation had been reported. Treatment of PEODDN is generally unsatisfactory. Small and localized lesions may be surgically excised. There was little success with topical corticosteroids, tar, psoralen ultraviolet A, ultraviolet B, anthralin, keratolytics, and retinoids in our patient. Good results with laser therapy, in the form of ultrapulse CO2 laser and combined erbium/CO2 laser have been reported.[6]
CONCLUSION
We have reported a case of widespread PEODDN along the lines of Blaschko for the rarity of the condition. The notable features of our case were: Adult onset, presence of nodular lesions, and truncal involvement. This entity should be taken into consideration in the differential diagnosis of linear keratotic eruptions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Goddard DS, Rogers M, Frieden IJ, Krol AL, White CR, Jr, Jayaraman AG, et al. Widespread porokeratotic adnexal ostial nevus: Clinical features and proposal of a new name unifying porokeratotic eccrine ostial and dermal duct nevus and porokeratotic eccrine and hair follicle nevus. J Am Acad Dermatol. 2009;61:1060.e1–14. doi: 10.1016/j.jaad.2009.03.036. [DOI] [PubMed] [Google Scholar]
- 2.Masferrer E, Vicente MA, Bassas-Vila J, Rovira C, González-Enseñat MA. Porokeratotic eccrine ostial and dermal duct naevus: Report of 10 cases. J Eur Acad Dermatol Venereol. 2010;24:847–51. doi: 10.1111/j.1468-3083.2009.03498.x. [DOI] [PubMed] [Google Scholar]
- 3.Cambiaghi S, Gianotti R, Caputo R. Widespread porokeratotic eccrine ostial and dermal duct nevus along Blaschko lines. Pediatr Dermatol. 2007;24:162–7. doi: 10.1111/j.1525-1470.2007.00367.x. [DOI] [PubMed] [Google Scholar]
- 4.Marsden RA, Fleming K, Dawber RP. Comedo naevus of the palm – A sweat duct naevus? Br J Dermatol. 1979;101:717–22. doi: 10.1111/j.1365-2133.1979.tb05653.x. [DOI] [PubMed] [Google Scholar]
- 5.Abell E, Read SI. Porokeratotic eccrine ostial and dermal duct naevus. Br J Dermatol. 1980;103:435–41. doi: 10.1111/j.1365-2133.1980.tb07268.x. [DOI] [PubMed] [Google Scholar]
- 6.Wong JW, Summers EM, Taylor MB, Harris RM. Porokeratotic eccrine ostial and dermal duct nevus treated with a combination erbium/CO2 laser: A case and brief review. Dermatol Online J. 2011;17:10. [PubMed] [Google Scholar]
- 7.Easton JA, Donnelly S, Kamps MA, Steijlen PM, Martin PE, Tadini G, et al. Porokeratotic eccrine nevus may be caused by somatic connexin26 mutations. J Invest Dermatol. 2012;132:2184–91. doi: 10.1038/jid.2012.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Valks R, Abajo P, Fraga J, Aragüés M, García-Diez A. Porokeratotic eccrine ostial and dermal duct nevus of late onset: More frequent than previously suggested? Dermatology. 1996;193:138–40. doi: 10.1159/000246230. [DOI] [PubMed] [Google Scholar]
- 9.Pathak D, Kubba R, Kubba A. Porokeratotic eccrine ostial and dermal duct nevus. Indian J Dermatol Venereol Leprol. 2011;77:174–6. doi: 10.4103/0378-6323.77457. [DOI] [PubMed] [Google Scholar]
- 10.Mazuecos J, Ortega M, Ríos JJ, Camacho F. Long-term involution of unilateral porokeratotic eccrine ostial and dermal duct naevus. Acta Derm Venereol. 2003;83:147–9. doi: 10.1080/00015550310007599. [DOI] [PubMed] [Google Scholar]