

Sir,
Porokeratotic eccrine ostial and dermal duct nevus (PEODDN) is a rare disorder of keratinization involving the intraepidermal part of the eccrine duct (acrosyringium) and hair follicles. It was initially described by Marsden et al. as comedo nevus of the palm. However, Abell and Reed coined the term “PEODDN” in 1980.[1]
We herein present a case of PEODDN that had unique clinical and histopathological findings. Our patient was a 30-year-old healthy lady who presented with multiple, asymptomatic, elevated skin lesions over her left upper limb. Small lesions appeared three years ago over her left index finger and gradually extended to the forearm. There was no seasonal variation. Cutaneous examination demonstrated multiple well-circumscribed, hyperpigmented, verrucous papules on the dorsum of the left index finger extending up to the extensor aspect of mid forearm. Some of the lesions were discrete while others coalesced to form plaques in a linear configuration. Of note, many of these papules showed a central pit [Figure 1]. Hair, nails, and mucosae were within normal limits; however, the nail of the index finger showed multiple shallow pits and a single longitudinal groove. Family history and systemic examination were not contributory. Linear porokeratosis, linear lichen planus, linear verrucous epidermal nevus, and linear Darier's disease were considered in the list of clinical differentials. A complete blood cell count with differential analysis and a comprehensive biochemistry panel did not reveal any abnormality. Histopathology of a representative skin lesion from the forearm showed hyperkeratosis, acanthosis, and papillomatosis. Cornoid lamella overlying a dilated eccrine duct ostium was visualized. An interesting finding was the presence of focal lichenoid infiltrate in the upper dermis [Figure 2a and b]. Based on the clinical and histopathological findings, our case was diagnosed as PEODDN along with a unique histological finding of a lichenoid infiltrate.
Figure 1.

Multiple verrucous papules and plaques arranged in a linear manner over left index finger and forearm. Note many papules have a central pit (a). Close up of lesions over index finger (b)
Figure 2.
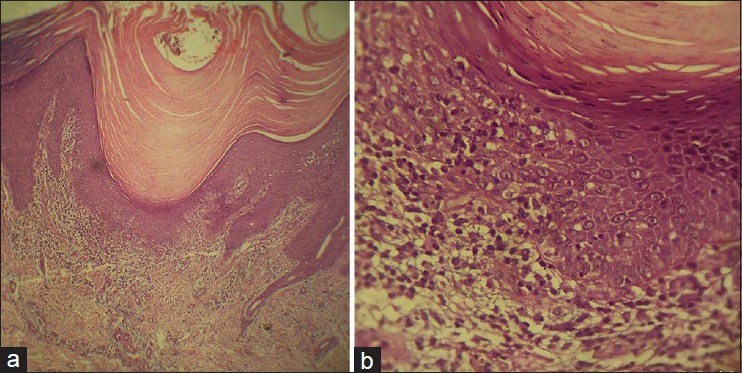
Cornoid lamella, irregular acanthosis with focal mononuclear cell infiltration in upper dermis at epidermal–dermal interface (H and E, ×100) (a). Note focal degeneration of the basal layer (H and E, ×400) (b)
Porokeratotic eccrine ostial and dermal duct nevus is a rare dermatological entity, whose pathogenesis is yet to be described. Stoof et al. had proposed that the epidermal invagination originates from a widely dilated acrosyringium which is continuous with dermal duct at its base;[2] while others believe that the invagination is the end result of the proliferation of abnormal clone of epidermal cells producing the cornoid lamella.[3] Masferrer et al. suggested that PEODDN originates from a circumscribed keratinization abnormality based on carcinoembryonic antigen staining positivity along the ductal lumina through the parakeratotic column of cornoid lamella.[4]
The condition is usually asymptomatic but is occasionally pruritic with or without hidrotic changes and the onset may range from birth till adulthood. PEODDN usually presents as grouped keratotic pits and is usually noted on the palms and soles. When sites other than palm and sole are involved, it presents as keratotic papules and plaques resembling linear verrucous epidermal nevus, as evident in our case. The uniqueness of our case lies in the involvement of dorsum of the hand, with sparing of the most common site (palms). Goddard et al. described five cases with atypical presentations of PEODDN; one of them being characterized by involvement of the dorsum of the fourth finger. Histopathology showed features of porokeratosis along with lichenoid infiltrate; similar to our case.[5]
There are rare reports of associations with Bowen disease, deafness and development delay, seizure disorder, hemiparesis, scoliosis, hyperthyroidism and sensory polyneuropathy, breast hypoplasia, alopecia, onychodysplasia, and squamous cell carcinoma.[5]
Treatment options are limited. Some lesions may undergo spontaneous flattening with time. Small and localized lesions may be suitable candidates for surgery. Laser therapy, preferably ultra-pulse CO2 laser, is an excellent modality because the chances of pigmentary changes and scarring are minimal. Combined erbium/CO2 laser therapy has been shown to offer significant cosmetic improvement in PEODDN patients. Modalities such as topical steroids, retinoids, keratolytics, phototherapy, electrocautery, and cryotherapy have not shown any promising results.[4,5]
The presence of two unusual findings, namely involvement of dorsum of the hand and presence of a focal lichenoid infiltrate in a case of PEODDN prompted the present report.
ACKNOWLEDGMENT
The authors would like to thank Prof. M. Ramam for his valuable inputs in reviewing the case and clinic-pathological correlation.
REFERENCES
- 1.Kumar P, Mondal AK, Ghosh K, Mondal A, Gharami RC, Chowdhury SN. Multiple keratotic papules on palm. Dermatol Online J. 2012;18:10. [PubMed] [Google Scholar]
- 2.Stoof TJ, Starink TM, Nieboer C. Porokeratotic eccrine ostial and dermal duct nevus. Report of a case of adult onset. J Am Acad Dermatol. 1989;20:924–7. doi: 10.1016/s0190-9622(89)70110-9. [DOI] [PubMed] [Google Scholar]
- 3.Bergman R, Lichtig C, Cohen A, Friedman-Birnbaum R. Porokeratotic eccrine ostial and dermal duct nevus. An abnormally keratinizing epidermal invagination or a dilated, porokeratotically plugged acrosyringium and dermal duct? Am J Dermatopathol. 1992;14:319–22. doi: 10.1097/00000372-199208000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Masferrer E, Vicente MA, Bassas-Vila J, Rovira C, González-Enseñat MA. Porokeratotic eccrine ostial and dermal duct naevus: Report of 10 cases. J Eur Acad Dermatol Venereol. 2010;24:847–51. doi: 10.1111/j.1468-3083.2009.03498.x. [DOI] [PubMed] [Google Scholar]
- 5.Goddard DS, Rogers M, Frieden IJ, Krol AL, White CR, Jr, Jayaraman AG, et al. Widespread porokeratotic adnexal ostial nevus: Clinical features and proposal of a new name unifying porokeratotic eccrine ostial and dermal duct nevus and porokeratotic eccrine and hair follicle nevus. J Am Acad Dermatol. 2009;61:1060.e1–14. doi: 10.1016/j.jaad.2009.03.036. [DOI] [PubMed] [Google Scholar]