

Abstract
Oseltamivir (Tamiflu), a neuraminidase inhibitor, was approved for seasonal flu by US Food and Drug Administration in 1999. A number of randomized controlled trials, systematic reviews, and meta-analysis emphasized a favorable efficacy and safety profile. Majority of them were funded by Roche, which also first marketed and promoted this drug. In 2005 and 2009, the looming fear of pandemic flu led to recommendation by prominent regulatory bodies such as World Health Organization (WHO), Centers for Disease Control and Prevention, European Medicines Agency and others for its use in treatment and prophylaxis of influenza, and it's stockpiling as a measure to tide over the crisis. Serious Adverse Events, especially neuropsychiatric events associated with Tamiflu started getting reported leading to a cascade of questions on clinical utility of this drug. A recent Cochrane review and related articles have questioned the risk-benefit ratio of the drug, besides raising doubts about the regulatory decision of approving it. The recommendations for stockpiling the said drug as given by various international organizations viz WHO have also been put to scrutiny. Although many reviewers have labeled the Tamiflu saga as a “costly mistake,” the episode leaves us with some important lessons. This article takes a comprehensive relook on the subject, and we proceed to suggest some ways and means to avoid a similar situation in the future.
KEY WORDS: Cochrane review, flu pandemic, H1N1, roche, stockpiling, Tamiflu
Introduction
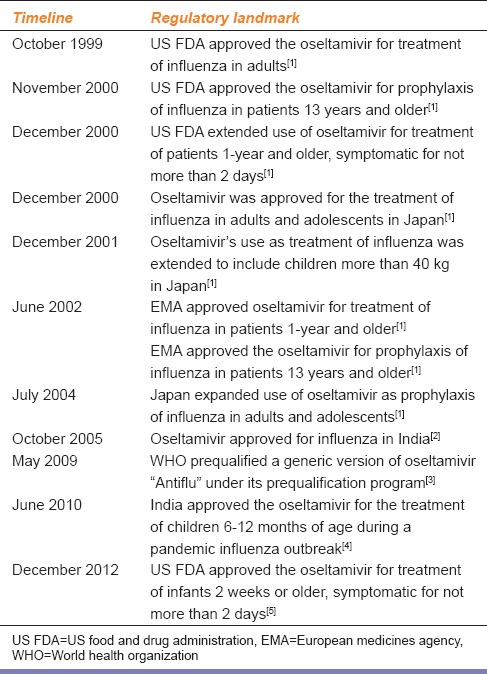
In 1999, the US Food and Drug Administration (US FDA) approved oseltamivir, a new drug in a class called Neuraminidase inhibitors proposed to be effective in seasonal flu, through its seemingly routine regulatory process. Roche, a pharmaceutical company launched oseltamivir in the global market with Tamiflu as its brand name. After US FDA approval, European Medicines Agency (EMA) soon followed suit. The chronology of its clinical development is given in Table 1.[1,2,3,4,5]
Table 1.
Chronology of clinical development of oseltamivir
Serious adverse events were first reported during post-marketing surveillance from Japan, UK, and subsequently from other places although most of the published articles did not report them. A recent Cochrane review and a series of articles in British Medical Journal (BMJ) have revealed the truth behind oseltamivir success story, which incidentally is one of the highest revenue earners for Roche. It is inexplicable that despite the lack of scientifically robust data on efficacy and safety of Oseltamivir, reputed organizations like World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), EMA, US FDA not only recommended the drug in question for treatment and prophylaxis of influenza but its stockpiling as well.
This fiasco essentially provides us with an opportunity to articulate tangible lessons so as to guard against such scientific transgressions in the future. There is a need to consider changes in the process of introduction of a new drug in the public health care system and to bring greater accountability and transparency in the way we practice science.
About flu and oseltamivir
Seasonal flu is a contagious viral infection which usually follows a mild course. Occasionally, complications such as pneumonia, bronchitis, otitis media, myocarditis, pericarditis, neurologic complications (viz confusion, convulsion, psychosis, neuritis, transverse myelitis, and encephalomyelitis), and dehydration occur.[6,7] The cause may be secondary bacterial illness or natural course of viral illness.
Oseltamivir, a sialic acid analog, restrains viral population to one generation, decreases viral load, and so contains the infection and its outcomes.[8]
Oseltamivir is taken orally and is absorbed from the GIT. Its active moiety is formed in the liver by the action of enzyme carboxyl esterase. Its half-life is 6–10 h with good oral bioavailability. The side effects include nausea, diarrhea, insomnia, abdominal pain, and headache.[8]
Oseltamivir Success-ground Reality
During the 1990s, Roche sponsored 40 clinical trials on oseltamivir. One such trial that formed a strong argument in favor of oseltamivir was a Randomized Controlled Trial (RCT) published in the year 2000 in The Journal of the American Medical Association.[9] In this RCT conducted on otherwise healthy patients (patients with no comorbidities), the authors concluded that early initiation (within 36 h) of treatment reduced illness duration by 30% and severity by 40%. It also significantly reduced the frequency of secondary complications of influenza. The authors went on to suggest the possibility that early initiation of antiviral drug might decrease the frequency of complications in high risk population and potentially cut down hospitalization rates although the study itself was not designed to address these issues. Authors offered no reasoning behind these promising assumptions. In the same article, they accepted few limitations in their study. No formalized criteria were used to define secondary complications of influenza, e.g., bronchitis, sinusitis, and functional definitions based on clinical practice, were used.
Another study, which was momentous in oseltamivir success, was published in The Lancet in the year 2000. This study was also carried out in otherwise healthy patients. In this RCT, Nicholson et al. elaborated the benefits of oseltamivir in terms of alleviation of symptoms, decreased viral load and improvement in health and activity. They also noted a shortening of the duration of illness. They, however, did not report any adverse effects associated with oseltamivir.[10]
In 2003, Kaiser et al. published a meta-analysis on oseltamivir and concluded “oseltamivir treatment of influenza illness reduces lower respiratory tract complications, antibiotics uses, and hospitalization in healthy and ‘at risk’ adults.”[11] This much-cited article was also supported by Roche and apparently formed a robust scientific argument for stockpiling the drug in later years. Such stockpiling was one of the components of contingency plans of various governments in reducing disease burden during a possible flu pandemic.[12]
A WHO funded systematic review by Jonathan Hsu et al., pooled 74 observational studies. Authors concluded that the oral oseltamivir might reduce mortality, hospitalization, and duration of symptoms as compared to no treatment. The quality of evidence available for such an inference was low to very low. Authors conceded that the mortality was assessed in high-risk patients, and therefore, generalizability of this inference was limited. The overall evidence was compromised due to confounding factors and multiple biases.[13]
Roche funded another meta-analysis of individual participant data collected during an influenza pandemic, H1N1pdm09. This study reported that the oseltamivir was effective in reducing mortality (evaluated as the primary outcome) across the spectrum of severity on early initiation of therapy in adults, pregnant women, and critically ill adult patients. Investigators did not report any benefit in pediatric patients, although they attributed this finding to lower case fatality proportion and high viral load in children and proposed that the prescribed dose might not be therapeutically effective. Authors concluded that the greatest likelihood of reduced mortality was attributable to treatment initiation within 2 days of symptoms onset. However, delayed treatment was still found to be effective in severely ill patients. Authors claimed that the strength of this study was a potential reduction in confounding factors, adjustment for treatment propensity, and coherence with ecological data. Authors further argued that conducting an RCT during a pandemic is a difficult task, and this study presents an exhaustive retrospective observational study. They retrospectively vindicated the prepandemic stockpiling by various governments.[14]
What Went Wrong?
The Japanese Saga
Independent events of “abnormal behavior and disturbance of consciousness” and few deaths after oseltamivir intake were reported in Japan. Japanese authorities initiated cohort studies in children. The initial studies were inconclusive except for a small increase in abnormal behavior on the 1st day after drug intake. However, an independent analysis of the data showed the oseltamivir to be associated with an increased risk of abnormal behavior by over 50% and significant occurrence of an unconscious state of mind on the 1st day after drug intake. Thus, Japan, which was once the biggest consumer of oseltamivir in the world, introduced a package insert warning against giving the drug to children and overall restricted use of this drug.[15] In 2007, Roche reviewed its data and did not report any increased risk of neuropsychiatric events.[16] But, global accumulation of adverse events on databases led to the updating of label warning against rare adverse events, e.g., hallucination, self-injury, abnormal behavior.[17]
The British Experience
A symptomatic case in a local school in UK in 2009 led to an order by the Health Protection Agency (HPA) to initiate 7 days prophylaxis of oseltamivir to all the kids in the school. The general consensus of opinion at HPA was “Prophylactic oseltamivir reduces the risk of contacts becoming symptomatic, shedding the virus, and infecting others. There is also scientific evidence that treating symptomatic people with oseltamivir can reduce infectiousness.” The professional experience of the treating physicians concluded that the “likely benefits did not outweigh likely risks.” This led to disagreement among Birmingham NHS Primary care trust.[18,19]
The Cochrane Review
The Cochrane Collaboration published their analysis of Neuraminidase inhibitors in 1999, 2003, 2006, 2009, 2010, 2012, and 2014. Reviews of Cochrane collaboration did not raise any major issues over safety and efficacy of oseltamivir till 2009.
In 2009, Dr. Hayashi, a Japanese pediatrician questioned the Cochrane team regarding the results of their review pointing out the fact that the conclusion of the study was not based on their own data analysis. Cochrane team had derived their report from a meta-analysis done by Kaiser et al. According to Hayashi, Kaiser et al. had based their review on 10 RCTs. Of these, only 2 RCTs (Nicholson 2000 and Treanor 2000) were published as articles in peer-reviewed journals. Other 8 RCTs were either presented as proceedings of the congress (5 RCTs), as abstracts in meetings and conferences (01 RCT each) or were available as data on file of the sponsor (01 RCT).[20]
In view of the emerging safety issues and Dr. Hayashi's specific objections, Cochrane collaboration decided to undertake a complete analysis of the clinical trial data set. However, they had difficulties in accessing the data, and it was not before protracted efforts lasting from 2009 to 2013 that they could gain access to all the materials. They needed full data set to formulate exhaustive and scientifically robust evidence. Cochrane had correspondence with WHO, US FDA, CDC, EMA, and European center for disease prevention and control. And it came as another surprise as none of them possessed full data.[21]
On April 10, 2014 Cochrane team published their revised review on oseltamivir after details of all the trials were revealed by Roche. Cochrane team based their review on clinical study reports from sponsors as well as minutes of proceedings of regulatory meetings.[22] This review comes as an eye-opener for the scientific community. The questions they have asked and the issues they have raised appear to be justified in the context of their tremendous importance for public health.
Revelations of Cochrane Review
Risk Benefit Ratio
Benefit-paltry or substantial?
Oseltamivir reduced the time to first alleviation of symptoms by 16.8 h (95% confidence interval 8.4–25.1 h P < 0.001) and by 29 h (95% confidence interval 12–47 h, P < 0.001) in healthy children.[23] The benefit of oseltamivir in asthmatic patients was insignificant. Pneumonia, hospitalization, and virus transmission were the major concerns with the disease for which benefits have been claimed in various studies. However, Cochrane review failed to establish any definitive benefit on these parameters.
Adverse effect profile-conveniently concealed
There had been no mention of adverse effects associated with the use of this drug in the published trials. Post-marketing surveillance had uncovered adverse effects like raised liver enzymes, hepatitis, neuropsychiatric events, cardiac arrhythmia, skin hypersensitivity reactions including toxic epidermal necrolysis, Stevens-Johnson syndrome and erythema multiforme, metabolic side effects and renal events.[24] In some cases, increased QTc prolongation was seen in ECG in the treatment group compared with placebo during on-treatment periods. The most important serious adverse events which raised concerns were neuropsychiatric events such as depressed mood, behavior disturbance, panic attack, suicidal ideation, delusion, delirium, convulsion, and encephalitis. These were reported more frequently in children than in adults and generally occurred within 48 h of drug intake.[25]
Harms Underplayed, and Benefits Overplayed?
Majority of the published studies described advantages with oseltamivir. According to Jonathan Hsu et al., oseltamivir decreased the risk of mortality in high-risk population (Odds ratio = 0.23, 95% confidence interval - 0.13–0.43) and hospitalization (Odds ratio = 0.75, 95% confidence interval - 0.66–0.89) compared with no treatment.[13] Rationality and importance of these data create a doubt when analyzed in the context of the case fatality rate of influenza. The estimated case fatality rate of influenza is 0.15–0.25%, with most deaths in middle-aged adults with underlying diseases.[26]
Cochrane review states that oseltamivir showed significant benefit in cases where pneumonia was nonverified or self-verified. The studies in which standard definition and diagnostic criteria were applied, statistical analysis of study reports concluded that the benefit was insignificant. Similar conclusions were obtained with other secondary illnesses of influenza-like otitis media, sinusitis, and bronchitis. Reporting of other complications was also passive. Oseltamivir was found to be ineffective in asthmatic children. Thus, according to Cochrane team oseltamivir does not appear to be effective in cases where it may found a better application. In a similar vein, a systematic review of systematic reviews, published in PLOS One in April 2013 concluded that oseltamivir did not provide any treatment benefit in elderly and at risk groups and it did not affect rate of hospitalization or mortality. To sum it up, cumulative risks prevail over small benefits of oseltamivir for prophylaxis and treatment of influenza in healthy humans.[27]
Though a large number of RCTs and meta-analyses had been conducted on oseltamivir, these failed to report important adverse events such as neuropsychiatric adverse effects. These were later revealed by independent clinicians, post-marketing studies and led to label change warning. Finally, sound evidence was provided by a systematic review conducted by Cochrane Collaboration, published in BMJ in April 2014. In this systematic review, the magnitude of risk difference of neuropsychiatric events during the combined “on-treatment” and “off-treatment” periods was 1.06% (0.07–2.76%) and two “pivotal” treatment trials showed significant association of oseltamivir dose (75 mg [standard dose] and 150 mg [high dose] twice daily) with neuropsychiatric events (P = 0.038).[24]
There was no significant difference in the rate of admission to the hospital in the treatment and placebo arms. Drug was given to symptomatic patients only, missing out on large no of asymptomatic patients who were a major source of viral transmission. Thus, any inference that the drug reduced transmission of the virus from infected individuals to healthy contacts appears to be incomplete. Further studies are needed to reach such a conclusion.
In other words, benefits had been overplayed, and harms had been underplayed in the reporting of the trials.[23]
Other Issues Raised by Cochrane Team
In the context of evidence-based medicine, an RCT is considered as the gold standard.[28] In the case of oseltamivir, RCTs had lacked precision, and most of them provided low-quality evidence. The study designs were poor for most of the trials. Dummy placebo containing dehydrocholic acid and dibasic calcium phosphate dihydrate had been used, which caused mainly gastrointestinal symptoms.[23] For documentation of complications, non-specific forms had been used and reporting itself was passive. Diagnosis had been confirmed on the basis of clinical judgment of physicians without a detailed definition, diagnostic criteria, and confirmatory investigations. Reporting of the adverse effects had been selective so was reporting of trial data. Thus, there was reporting, publication, and survivor bias.
Some of the glaring shortcomings brought out by the Cochrane review team are:
Why was there no reporting of neuropsychiatric events during the trial? Was it due to small scale trial?
Why was large-scale trial not commanded from the pharmaceutical industry when it was obviously a case of enormous public health importance and would have huge commercial impact on industry's revenues?
Why had there been no study on relapse cases?
Why was the adverse events profile studied till the treatment lasted? Why was no analysis done after the patients stopped treatment even though it was known that side-effects could present even after stopping the treatment.
Drug was widely used for H1N1 strain of virus in 2009 though before that strain was virtually unknown. Hence, the drug's efficacy was never before tested on the strain. Why was a scientifically sound observational study not done after this “experiment” by independent investigators?
A Chain Reaction of Failure
Cochrane study group have raised questions on the data retrieving and analyzing processes of many of the world's eminent regulatory bodies. And they have fallen short of expectations, an instance of propagation of failure based on which decisions of enormous capital value had been taken. They have highlighted inherent defects in the methods utilized for regulatory processes which are likely to bias the results of trials, systematic reviews, and meta-analysis.
World Health Organization has not clarified oseltamivir's status as an essential medicine.[29] WHO set aside questions raised regarding the management of A/H1N1 pandemic flu as “Conspiracy Theories”.[30] Interruption of transmission which theoretically will allow time for intervention by vaccine was the strongest rationale behind using oseltamivir according to WHO. But, WHO never had a complete set of trial data to prove or disprove its theory.[16]
US Food and Drug Administration's Lack of a Strong Stance
Marketing practices of Roche were “false or misleading” as declared by US FDA in Nov 2000 because of Roche's extravagant advertisement claiming significant reduction in secondary bacterial infections in flu cases.[31] According to Jefferson, its methods were invisible and appeared to have ignored the evidence of psychiatric harms from the trials it had full access to. It observed 75 cases of adverse events during a safety review and noted 12 child death cases in its adverse events database. US FDA accepted that the oseltamivir has not been shown to prevent serious bacterial infections.[32]
Centers for Disease Control and Prevention
Early initiation of treatment (within 48 h) with neuraminidase inhibitors may reduce complications (e.g. otitis media in young children, pneumonia, and respiratory failure) and death, and decrease the duration of hospitalization. It also recommends treatment with oseltamivir in patients who are more likely to develop complications of influenza.[33] However, it does not provide any credible evidence for its continued advocation of oseltamivir in the treatment and prophylaxis of influenza.
European Medicines Agency denied not having full set of data. It made cautious statements when confronted by BMJ over cases of neuropsychiatric events in UK as having assessed “all data provided by Roche” or “no available data” showed an increased risk of neuropsychiatric events.[34]
Indian Scenario
Jan 2006, an Indian firm Hetero-Drugs was granted sublicense by Roche for producing oseltamivir to assist in stockpiling the drug.[35]
Considering the social and demographic factors of India, government initiated plans to tackle a pandemic influenza by stockpiling oseltamivir.[36] Cipla obtained regulatory approval for its generic drug Antiflu when WHO prequalified it,[3] and acquired compulsory licensing to manufacture its product.[37] Antiflu was introduced in the market in the late 2009 during H1N1 pandemic flu.
The question is which data did WHO look at to reach its decision? Did regulatory authority of India perform their own data analysis before it authorized the drug to be marketed in the country or look at the data of post-marketing surveillance later on? It appears incredible that no scientifically sound observational study had been conducted to assess the efficacy and safety issues, e.g. incidence of SAEs like neuropsychiatric events in postmarketing surveillance which had been reported in other parts of the world. Should the Government consider large-scale study to credit or discredit controversy surrounding oseltamivir? It is obviously a matter of national importance considering the huge sum of public money.
Oseltamivir – Is It a Case of Multisystem Failure?
Approval by US US FDA and EMA appears to be a judgment based medicine rather than evidence-based medicine. It appears that the regulatory authorities took their decision under the pressure of providing a pharmaceutical solution to a pandemic disease.
Stockpiling by the countries was based on assumptions and not hard data. None of the studies were done during a pandemic. Access to full methods and results was not available to regulatory authority. There is always a high degree of control over the trial if it is conducted by manufacturer, and it creates conflict of interest.[38]
Oseltamivir – Windfall for Pharma Company
Roche has been benefitted with oseltamivir by more than 18 billion $ since its launch in 1999. Its sales were increased by 84% by oseltamivir during US flu season in 2013. UK stockpiled the drug worth 710 million $ for 40 million treatments. US spent 1.3 billion $ on stockpiling oseltamivir for 65 million dosages.[39] India also increased its stock by 10 fold.[40]
What May Be the Way Forward?
While oseltamivir has been identified as a classical case of multiple, linearly aligned errors and omissions; wherein manipulated evidence, selective disclosures, and a favorably timed pandemic disease have ensured windfall for pharmaceutical companies. We need to devise ways and means so that wasteful exercises such as this can be minimized, and patients are not made to consume medicines of questionable risk-benefit ratio.
Pharmaceutical Company
Pharmaceutical companies need to share full data of clinical trials and place the same in the public domain. They can go ahead and publish their study results in the manner they like, but the study should be verifiable with full data. There should be an independent expert committee to look into the matter of reporting bias and poor design of the study associated with the trials funded by pharmaceutical companies.
Government and Funding Agency
Inadequacy of present resources, e.g. time allocation, funding configuration, are major limitations for scrutinizing clinical study report by systematic reviewers. A detailed rational evidence formulation is an essential prerequisite for evidence-based medicine. It is the cornerstone of modern science. But, it is capital intensive like pure science for a long-term benefit of society. It is the responsibility of the government to develop a realistic attitude toward a genuine problem.
Regulatory Policies
There should be change in the policy of the regulatory authorities. In all studies where humans are a part of the trial, all the data should be made available in the public domain if demanded. It should not be the prerogative of sponsors. The inconsistencies among major regulatory bodies have been a prime feature of oseltamivir fiasco. They need a new think-tank to come up with a solution for this conflicting situation. A central regulatory body which will work out the discrepancy and integrate their analysis might be a step toward finding a solution. EMA has already taken the lead and changed its policy vis-à-vis data availability.[41] A concerted public awareness initiative should also be undertaken to underscore the scientific imperatives behind drug development and the inherent inefficiency of the entire process. There needs to be wider social understanding of the fact that modern evidence-based medicine is unlikely to throw up quick fix solution to emerging public health problems irrespective of their seriousness. A case in point is the emerging epidemic of Ebola that in spite of its high infectivity and mortality, is still away from a reliable, effective, and safe therapeutic solution.
What should India do?
A good start has been made in India by making the registry of any clinical trial mandatory at Clinical Trials Registry India. This needs to be taken further by placing all the trial data in open access public domain. There should be mandatory seamless integration of ethical approval, regulatory approval, trial registry, availability of trial data, and post-trial publication in scientific journals in such a manner, and hence that all these steps are mutually identifiable and accessible.
The government should look at the advisory from international regulatory bodies and health organizations into our perspective before its acceptance and subsequent application. The oseltamivir fiasco proves that India needs to build appropriate capacity so that emerging scientific evidence is analyzed in-house keeping in mind the country's peculiar social and economic context and the reliance on international guidelines to formulate national policies is reduced.
It might be a better move for the government to improve its manufacturing capacity by involving Pharma central public sector enterprises. They work on a “no profit no loss” basis compared to “for profit” motive of private pharmaceutical companies. Pharma CPSEs can be entrusted with such tasks of medical and national importance. Compulsory licensing can be provided to them. However, this will entail tremendous capacity building at the end of Pharma CPSEs as currently they are neither mandated nor geared up for such an onerous task. Further, to safeguard against possible future rise in demand, raw material can be stockpiled rather than the finished product. Government needs to take a dynamic approach in its endeavors to reduce its wasteful exercises and to save hard earned public money.
In consideration of future redundancy, it is a necessary step for India to expeditiously upscale its manufacturing and marketing practices.
Conclusion
A cocktail of pandemic panic, publicity propaganda, and scientific misconduct turned a new medicine with only modest efficacy into a blockbuster. It appears that the multiple regulatory checks and balances gave way as science lost its primacy and pharmaceutical enterprise lost no time in making the most of it. This reminds one of Prof R. P. Feynman's statements after Challenger space shuttle disaster.
“Reality must take precedence over public relations as nature can’t be fooled”
- Prof R. P. Feynman
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Hoffmann-La Roche Inc. Pediatric Advisory Committee Executive Summary for Oseltamivir. 2005. [Last accessed on 2014 May 22]. Available from: http://www.US FDA.gov/ohrms/dockets/ac/05/briefi ng/2005-4180b0607Oseltamivir%20Executive%20Summary_Oct25.pdf .
- 2.Central Drugs Standard Control organization. List of drugs approved during. 2005. [Last accessed on 2014 May 22]. Available from: http://www.cdsco.nic.in/writereaddata/list_of_drugs_approved_during_2005.htm .
- 3.World Health Organization. WHO Prequalification Programme prequalifies first generic Oseltami vir Product. Prequalification. [Last accessed on 2014 May 21; Last update on 2009 May 13]. Available from: http://apps.who.int/prequal/info_press/pq_news_13May09_List.htm .
- 4.Central Drugs Standard Control organization. List of drugs approved from 01/01/2010-31/12/2010. [Last accessed on 2014 May 22]. Available from: http://www.cdsco.nic.in/writereaddata/LIST%20OF%20APPROVED%20DRUG%20FROM%2001.htm .
- 5.Food and Drug Administration. US FDA expands Oseltamivir's use to treat children younger than 1 year US FDA News Release. 2012. [Last accessed on 2014 May 22]. Available from: http://www.USFDA.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333205.htm .
- 6.Nicholson KG. Clinical features of influenza. Semin Respir Infect. 1992;7:26–37. [PubMed] [Google Scholar]
- 7.Rothberg MB, Haessler SD, Brown RB. Complications of viral influenza. Am J Med. 2008;121:258–64. doi: 10.1016/j.amjmed.2007.10.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Moscona A. Neuraminidase inhibitors for influenza. N Engl J Med. 2005;353:1363–73. doi: 10.1056/NEJMra050740. [DOI] [PubMed] [Google Scholar]
- 9.Treanor JJ, Hayden FG, Vrooman PS, Barbarash R, Bettis R, Riff D, et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: A randomized controlled trial. US Oral Neuraminidase Study Group. JAMA. 2000;283:1016–24. doi: 10.1001/jama.283.8.1016. [DOI] [PubMed] [Google Scholar]
- 10.Nicholson KG, Aoki FY, Osterhaus AD, Trottier S, Carewicz O, Mercier CH, et al. Efficacy and safety of oseltamivir in treatment of acute influenza: A randomised controlled trial. Neuraminidase Inhibitor Flu Treatment Investigator Group. Lancet. 2000;355:1845–50. doi: 10.1016/s0140-6736(00)02288-1. [DOI] [PubMed] [Google Scholar]
- 11.Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med. 2003;163:1667–72. doi: 10.1001/archinte.163.14.1667. [DOI] [PubMed] [Google Scholar]
- 12.Wan Po AL, Farndon P, Palmer N. Maximizing the value of drug stockpiles for pandemic influenza. Emerg Infect Dis. 2009;15:1686–7. doi: 10.3201/eid1510.090844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Geneva: World Health Organization; 2010. [Last accessed on 2014 May 25]. WHO Guidelines for Pharmacological Management of Pandemic (H1N1) 2009 Influenza and other Influenza Viruses. Available from: http://www.who.int/csr/resources/publications/swineflu/h1n1_guidelines_pharmaceutical_mngt.pdf . [PubMed] [Google Scholar]
- 14.Hsu J, Santesso N, Mustafa R, Brozek J, Chen YL, Hopkins JP, et al. Antivirals for treatment of influenza: A systematic review and meta-analysis of observational studies. Ann Intern Med. 2012;156:512–24. doi: 10.7326/0003-4819-156-7-201204030-00411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Muthuri SG, Venkatesan S, Myles PR, Leonardi-Bee J, Al Khuwaitir TS, Al Mamun A, et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: A meta-analysis of individual participant data. Lancet Respir Med. 2014;2:395–404. doi: 10.1016/S2213-2600(14)70041-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cohen D. Oseltamivir: Another case of regulatory failure? Br Med J. 2014;348:g2591. [Google Scholar]
- 17.Oseltamivir linked to abnormal behavior in children, label changes sought. Nov 26, 2007. Parker Waichman LLP. [Last accessed on 2014 May 28]. Available from: http://www.yourlawyer.com/articles/title/Oseltamivir-linked-to-abnormal-behavior-in-children-label-changes-sought .
- 18.Toovey S, Rayner C, Prinssen E, Chu T, Donner B, Thakrar B, et al. Assessment of neuropsychiatric adverse events in influenza patients treated with oseltamivir: A comprehensive review. Drug Saf. 2008;31:1097–114. doi: 10.2165/0002018-200831120-00006. [DOI] [PubMed] [Google Scholar]
- 19.Waknine Y. US FDA Safety Changes: Lexiva, Oseltamivir, Pexeva. Medscape Multispeciality. [Last accessed on 2014 May 28]. Available from: http://www.medscape.org/viewarticle/552171 .
- 20.Kitching A, Roche A, Balasegaram S, Heathcock R, Maguire H. Oseltamivir adherence and side effects among children in three London schools affected by influenza A (H1N1) v, May 2009-an internet-based cross-sectional survey. Euro Surveill. 2009;14:19287. doi: 10.2807/ese.14.30.19287-en. [DOI] [PubMed] [Google Scholar]
- 21.Rouse A. Oseltamivir, the state and informed consent. Br Med J. 2009. [Last accessed on 2014 May 22]. Available from: http://www.bmj.com/rapid-response/2011/11/02/Oseltamivir-state-and-informed-consent .
- 22.Cohen D. Complications: Tracking down the data on oseltamivir. BMJ. 2009;339:b5387. doi: 10.1136/bmj.b5387. [DOI] [PubMed] [Google Scholar]
- 23.Doshi P, Jones M, Jefferson T. Rethinking credible evidence synthesis. BMJ. 2012;344:d7898. doi: 10.1136/bmj.d7898. [DOI] [PubMed] [Google Scholar]
- 24.Jefferson T, Jones M, Doshi P, Spencer EA, Onakpoya I, Heneghan CJ. Oseltamivir for influenza in adults and children: Systematic review of clinical study reports and summary of regulatory comments. BMJ. 2014;348:g2545. doi: 10.1136/bmj.g2545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Simon RJ. Oseltamivir and neuropsychiatric disturbance in adolescents. The case is not proved but caution is advisable. Br Med J. 2007;334:1232–3. [Google Scholar]
- 26.Chung S, Joung YS. Oseltamivir (tamiflu) induced depressive episode in a female adolescent. Psychiatry Investig. 2010;7:302–4. doi: 10.4306/pi.2010.7.4.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Michiels B, Van Puyenbroeck K, Verhoeven V, Vermeire E, Coenen S. The value of neuraminidase inhibitors for the prevention and treatment of seasonal influenza: A systematic review of systematic reviews. PLoS One. 2013;8:e60348. doi: 10.1371/journal.pone.0060348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Girard MP, Tam JS, Assossou OM, Kieny MP. The 2009 A (H1N1) influenza virus pandemic: A review. Vaccine. 2010;28:4895–902. doi: 10.1016/j.vaccine.2010.05.031. [DOI] [PubMed] [Google Scholar]
- 29.Freemantle N, Shallcross LJ, Kyte D, Rader T, Calvert MJ. Oseltamivir: The real world data. BMJ. 2014;9(348):g2371. doi: 10.1136/bmj.g2371. [DOI] [PubMed] [Google Scholar]
- 30.World Health Organization. Unedited Report of the Supplementary Meeting of the Expert Committee on the Selection and Use of Essential Medicines. 2010. [Last accessed on 2014 May 22]. Available from: http://www.who.int/entity/selection_medicines/committees/expert/emergency_session/unedited_Emergency_report.pdf .
- 31.Cohen D, Carter P. Conflicts of interest. WHO and the pandemic flu “conspiracies”. BMJ. 2010;340:c2912. doi: 10.1136/bmj.c2912. [DOI] [PubMed] [Google Scholar]
- 32.US FDA warning letters. [Last accessed on 2014 May 24]. Available from: http://www.US FDA.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/EnforcementActivitiesbyUSFDA/WarningLettersandNoticeofViolationLetterstoPharmaceuticalCompanies/UCM166329.pdf .
- 33.Jefferson T, Doshi P. Multisystem failure: The story of anti-influenza drugs. BMJ. 2014;348:g2263. doi: 10.1136/bmj.g2263. [DOI] [PubMed] [Google Scholar]
- 34.Centers for Disease Control and Prevention. Influenza Antiviral Medications: Summary for Clinicians. [Last accessed on 2014 May 23]. Available from: http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm .
- 35.O’Dowd A. UK regulators deny claims that their access to oseltamivir trial data was insufficient. Br Med J. 2013;346:f3966. doi: 10.1136/bmj.f3966. [DOI] [PubMed] [Google Scholar]
- 36.News Medical. Oseltamivir-Oseltamivir production. [Last accessed on 2014 May 25]. Available from: http://www.news-medical.net/health/Oseltamivir-Oseltamivir-Production.aspx .
- 37.Clinical Management Protocol (Novel Influenza A H1N1) [Last accessed on 2014 May 25]. Available from: http://mohfw-h1n1.nic.in/documents/PDF/Annexure-XX.pdf .
- 38.Staton T. Will Cipla's Antiflu prompt mass patent-waiving? Fierce Pharm. 2009. [Last accessed on 2014 May 25]. Available from: http://www.fiercepharma.com/story/will-ciplas-antifluprompt-mass-patent-waiving/2009-05-14 .
- 39.Jack A. Tamiflu: A nice little earner. BMJ. 2014;9(348):g2524. doi: 10.1136/bmj.g2524. [DOI] [PubMed] [Google Scholar]
- 40.24*7 News. India to increase anti-flu drug stockpile 10 times. [Last accessed on 2014 May 25]. Available from: http://www. 24×7news.wordpress.com/2009/05/02/india-to-increase-anti-flu-drug-stockpile-10-times/
- 41.Torjesen I. Europe's drug agency will publish clinical trial data for new products from 2014. BMJ. 2012;345:e8061. doi: 10.1136/bmj.e8061. [DOI] [PubMed] [Google Scholar]