

Dear Editor:
External genital warts, also known as condyloma acuminata, is one of the most common sexually transmitted diseases and is caused by human papillomavirus infection1. Currently used treatments include imiquimod, podophyllin, interferons, cryotherapy, chemotherapeutic agents, cidofovir, laser vaporization, and surgical removal2,3,4. However, none of these modalities are considered to be the gold standard, and all of them vary greatly with respect to cost, adverse effect profiles, dosing schedules, treatment duration, and overall effectiveness. Bleomycin, an antibiotic agent with antineoplastic properties, has been used to treat recalcitrant palmoplantar warts; however, there are few reports in the literature about its effect on genital warts5,6,7. Therefore, this preliminary prospective study assessed the efficacy and safety of intralesional bleomycin injection for genital warts.
From June 2011 to March 2013, we enrolled 15 patients (14 men, 1 woman) with a total of 164 genital warts. The patients' age ranged from 23~78 years (mean, 43.3 years). Regarding location, 3, 15, 39, 2, and 105 lesions were located on the vulva, scrotum, anus, glans penis, and penile shaft, respectively. The dimensions of these warts (short×long axes) ranged from 2×2 to 22×40 mm. Five patients were previously treated with other modalities (2 with podophyllin, 2 with carbon dioxide laser ablation, and 1 with 5% imiquimod cream) but experienced recurrence. Genital warts were diagnosed on the basis of clinical examination, and biopsy specimens were evaluated only if the lesions appeared ambiguous. Patients with peripheral vascular disease such as Raynaud's phenomenon were excluded from this study. The study was approved by the institutional review board of Kangdong Sacred Heart Hospital (No. 11-105) and conducted in accordance with the principles outlined in the Declaration of Helsinki. For injections, bleomycin (Bleocin; Nippon Kayaku Co., Ltd., Tokyo, Japan) was diluted with 4 ml normal saline and 6 ml 2% lidocaine to a final concentration of 1.5 mg/ml. This diluted solution was slowly injected into the base of the wart by using a 31-G insulin syringe (BD Ultra-Fine II Needle; Becton Dickinson, Franklin Lakes, NJ, USA) until blanching was observed. At each visit, <2 ml bleomycin was administered to prevent local adverse reactions. Any clinical changes or adverse reactions were recorded every 2 weeks, and injections were repeated if the wart remained. A wart was considered cleared if it was completely resolved; otherwise, the treatment was considered to have failed. The patients were followed up until dermatologists confirmed wart-free status; the total follow-up period ranged from 3~20 months (mean, 12.4 months).
The baseline clinical characteristics and treatment outcomes are described in Table 1. Of the 15 patients, warts were completely resolved in 11 (73.3%) (Fig. 1). Two patients (13.3%) experienced recurrence after complete resolution, and another 2 (13.3%) experienced only partial resolution. The total volume of bleomycin injected ranged from 0.1~1.44 ml, and the mean volume injected per treatment was 0.27 ml. No allergic reactions (e.g., anaphylaxis) or evidence of systemic adverse reactions were reported. Only local adverse reactions including pain, dyspigmentation, crust, and mild scar formation were noted. Five patients (33.3%) experienced moderate to severe pain after the procedure; however, the pain disappeared within 1 week with or without oral analgesics. Dyspigmentation in the treated region developed in 3 patients (20%) during follow-up. Furthermore, 10 patients (66.7%) experienced crust formation; in particular, 2 patients developed a mild atrophic scar on the lesion site after the crust was removed, whereas the crust resolved spontaneously without scarring in the remaining 8 patients.
Table 1. Characteristics and treatment outcomes of patients with genital warts.
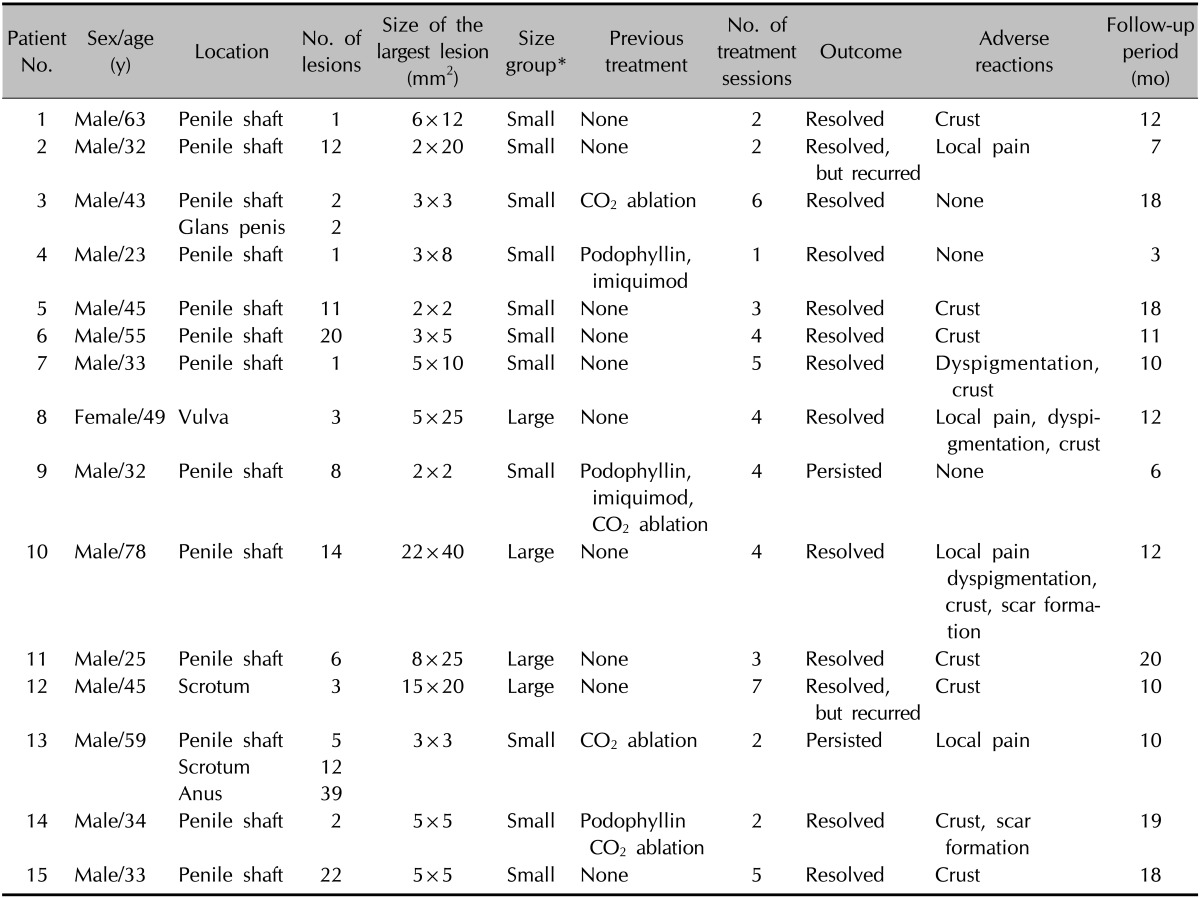
*Dimensions of the largest lesion with warts (short×long axes) were estimated by using calipers. Warts were classified as large if they were >100 mm2.
Fig. 1. Clinical findings in patient #10. (A) A crusted, verrucous plaque (average dimensions, 22×40 mm) located on the penile shaft. (B) After the second intralesional bleomycin injection, the genital warts had nearly resolved, although mild erosion had developed. (C) Clearance of genital warts with hypopigmentation at 2 weeks after 4 treatment sessions of intralesional bleomycin injection.

Bleomycin is an antitumor, antibacterial, and antiviral agent that was first isolated by Umezawa from the fungus Streptomyces verticillus in 1966; it is widely used to treat recalcitrant palmoplantar warts6,7. Several clinical trials have evaluated the efficacy of bleomycin in the treatment of cutaneous warts, with success rates ranging from 16%~94%2. However, only a few studies have focused on genital warts. Figueroa and Gennaro5 report a 70% treatment success rate of genital warts by using bleomycin with a few complications such as local soreness, pruritus, and spotting of blood, none of which required further treatment. Similarly, in the present study, bleomycin successfully resolved genital warts in 73.3% of patients, without any significant complications. Complications including pain, dyspigmentation, crust, and scar did not interfere with the ability to administer further treatment. In particular, crust formation may suggest adequate infiltration of bleomycin during the injection, because bleomycin decreases blood flow, thus inducing necrosis and subsequent detachment of the lesion8. The most serious complication in such cases is local tissue necrosis, although this was not observed in the present study. Necrosis can occur because bleomycin hydrolase, which inactivates the injected bleomycin solution by hydrolyzing the amide bond in the β-amino-alanine-amide moiety, is present in very small amounts in skin9. The most effective strategy for preventing this cutaneous toxicity is decreasing the total cumulative dose of bleomycin8,9. In the case of genital warts, the delicate nature of the mucosal skin in the genital area makes it easy to control the amount and distribution of bleomycin, leading to fewer adverse reactions and increasing effectiveness. This study has several limitations such as the small number of patients and lack of precise methods to determine the total number of warts in each patient. The confounding factors in the assessment of the success rate, including the number, location, distribution, and depth of the warts, may be associated with treatment failure and thus require further investigation. Nevertheless, the results of our study suggest intralesional bleomycin injection is a simple treatment with only mild complications that is easy to administer in outpatient settings and may yield a satisfactory success rate for the treatment of genital warts.
References
- 1.Yanofsky VR, Patel RV, Goldenberg G. Genital warts: a comprehensive review. J Clin Aesthet Dermatol. 2012;5:25–36. [PMC free article] [PubMed] [Google Scholar]
- 2.Husseinzadeh N. Basic therapeutic principles and the strategy in the management of the external anogenital warts (condylomas): A review. J Clin Gynecol Obstet. 2013;2:1–9. [Google Scholar]
- 3.Sterling JC, Handfield-Jones S, Hudson PM British Association of Dermatologists. Guidelines for the management of cutaneous warts. Br J Dermatol. 2001;144:4–11. doi: 10.1046/j.1365-2133.2001.04066.x. [DOI] [PubMed] [Google Scholar]
- 4.Gunter J. Genital and perianal warts: new treatment opportunities for human papillomavirus infection. Am J Obstet Gynecol. 2003;189(3 Suppl):S3–S11. doi: 10.1067/s0002-9378(03)00789-0. [DOI] [PubMed] [Google Scholar]
- 5.Figueroa S, Gennaro AR. Intralesional bleomycin injection in treatment of condyloma acuminatum. Dis Colon Rectum. 1980;23:550–551. doi: 10.1007/BF02988993. [DOI] [PubMed] [Google Scholar]
- 6.Munn SE, Higgins E, Marshall M, Clement M. A new method of intralesional bleomycin therapy in the treatment of recalcitrant warts. Br J Dermatol. 1996;135:969–971. doi: 10.1046/j.1365-2133.1996.d01-1104.x. [DOI] [PubMed] [Google Scholar]
- 7.Amer M, Diab N, Ramadan A, Galal A, Salem A. Therapeutic evaluation for intralesional injection of bleomycin sulfate in 143 resistant warts. J Am Acad Dermatol. 1988;18:1313–1316. doi: 10.1016/s0190-9622(88)70140-1. [DOI] [PubMed] [Google Scholar]
- 8.Saitta P, Krishnamurthy K, Brown LH. Bleomycin in dermatology: a review of intralesional applications. Dermatol Surg. 2008;34:1299–1313. doi: 10.1111/j.1524-4725.2008.34281.x. [DOI] [PubMed] [Google Scholar]
- 9.Yamamoto T. Bleomycin and the skin. Br J Dermatol. 2006;155:869–875. doi: 10.1111/j.1365-2133.2006.07474.x. [DOI] [PubMed] [Google Scholar]