

A 29-year-old woman presented with a known nephrocalcinosis that had developed nine years earlier. Her past medical history was remarkable for a cardiac arrest secondary to a profound hypokalaemia (1.7 mEq/L) in the post-operative period following a complicated appendicular peritonitis at 19 years of age. Her on-going treatment included potassium citrate supplementation and increased fluid intake to induce hyperdiuresis. There was no relevant family history. On admission, pertinent laboratory data were as follows: hypokalaemia (3.4 mEq/L), normal anion gap hyperchloraemic metabolic acidosis (plasma  21 mEq/L), inappropriately high urine pH (7.0), positive urinary anion gap (þ21 mEq/L), tubular proteinuria 0.5 g per 24 h and chronic kidney disease (serum creatinine, 1.4 mg/dL. CKD Epi MDRD creatinine clearance, 72 mL/min). A urine pH of >5.3 in the presence of metabolic acidosis suggests distal renal tubular acidosis. On bicarbonate loading,
21 mEq/L), inappropriately high urine pH (7.0), positive urinary anion gap (þ21 mEq/L), tubular proteinuria 0.5 g per 24 h and chronic kidney disease (serum creatinine, 1.4 mg/dL. CKD Epi MDRD creatinine clearance, 72 mL/min). A urine pH of >5.3 in the presence of metabolic acidosis suggests distal renal tubular acidosis. On bicarbonate loading,  was <5%, with a low (urinary–blood) DpCO2 (13 mmHg), suggesting defective H+ secretion by alpha-intercalated cells. A CT scan imaging (Figure 1A) and plain X-ray of the abdomen (Figure 1B) showed macroscopic bilateral nephrocalcinosis. Biochemical analysis of the kidney stone revealed a calcium phosphate stone type suggestive of distal renal tubular acidosis (dRTA). She had polyclonal hypergammaglobulinaemia and positive antinuclear antibodies (1/1600) of anti-Ro/SS-A type. Accessory salivary gland biopsy showed Grade 2 inflammatory infiltrates on the Chisholm–Mason scale. The kidney biopsy revealed mild inflammatory cell infiltrates, with interstitial fibrosis.
was <5%, with a low (urinary–blood) DpCO2 (13 mmHg), suggesting defective H+ secretion by alpha-intercalated cells. A CT scan imaging (Figure 1A) and plain X-ray of the abdomen (Figure 1B) showed macroscopic bilateral nephrocalcinosis. Biochemical analysis of the kidney stone revealed a calcium phosphate stone type suggestive of distal renal tubular acidosis (dRTA). She had polyclonal hypergammaglobulinaemia and positive antinuclear antibodies (1/1600) of anti-Ro/SS-A type. Accessory salivary gland biopsy showed Grade 2 inflammatory infiltrates on the Chisholm–Mason scale. The kidney biopsy revealed mild inflammatory cell infiltrates, with interstitial fibrosis.
Fig. 1.
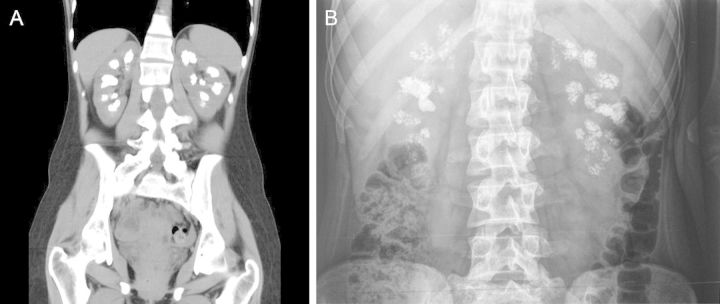
(A) Bilateral macroscopic nephrocalcinosis. (B) Plain X-ray.
Distal RTA is the most common cause of nephrocalcinosis due to hypercalciuria without hypercalcaemia. The reported prevalence of nephrocalcinosis in patients with dRTA ranges from 60 to 80%. Distal renal tubular acidosis (dRTA) related to Sjögren's syndrome occurred in up to 33%. Primary Sjögren's syndrome may manifest itself as dRTA-associated nephrocalcinosis by autoantibodies directed against the A-type intercalated cells in the collecting tubules leading to a defect in hydrogen ion secretion.