

Abstract
Objective
Hallux valgus (HV) is common in older adults, but limited studies of risk factors have reported conflicting results. This cross-sectional analysis examined the association of HV with foot pain and other characteristics in older adults.
Methods
HV, foot pain, foot structure (planus, rectus, cavus), current and past high heel use, age, and body mass index were assessed in the population-based Framingham Foot Study. Sex-specific logistic and multinomial logistic regression examined the association of HV and HV with pain with study variables.
Results
Of 1352 men and 1725 women (mean age 66 ± 10.5 years), 22% of men and 44% of women had HV and 3% of men and 11% of women had HV with pain. Foot pain increased odds of HV in both sexes (p<0.05). In women, older age and past high heel use increased odds of HV by 27% and 47%, respectively (p<0.01), and cavus foot structure decreased odds of HV by 26% (p=0.02). BMI > 30 kg/m2 decreased odds of HV by 33% in men and 45% in women (p<0.05). In women only, odds of Pain & HV vs. No Pain & No HV were greater with older age and planus foot structure.
Conclusions
Our work showed different associations in participants who had HV with pain compared to those without foot pain. In both men and women, strong relations were observed between HV and foot pain and inversely with BMI. Older age was associated with HV in women only, as were protective associations with cavus foot structure.
Keywords: hallux valgus, foot, pain, epidemiology
Introduction
Hallux valgus is common in older adults, but its association with foot pain and other factors is unclear in a population setting. Hallux valgus is a structural foot deformity in which the angular deviation of the hallux is greater than 15 degrees toward the lesser toes with respect to the first metatarsal bone, and it appears as a medial bony enlargement of the first metatarsal head. A number of studies have examined factors linked to hallux valgus and have shown that characteristics such as age1-5, sex1, 2, 4-6, pes planus, high heeled shoe use3, 7-9, other shoe characteristics8, 10, 11, and high BMI3 are associated with hallux valgus. These studies have reported conflicting results, perhaps arising from differences in study design, study population and definitions of variables.
Studies examining biomechanical factors found that a greater calcaneal stance position angle (i.e. a more valgus rearfoot position), higher peak pressure under the hallux, a greater force-time integral under the hallux and central forefoot region, and altered forefoot plantar pressure patterns were associated with hallux valgus12-14. Additionally, planus (flat) foot structure has been shown to be associated with hallux valgus in men only3. Hallux valgus is also thought to be attributable to genetics, as found by Hannan et al15, although the evidence in the literature is very sparse.
Foot pain, decreased function and worsened foot health have also been reported to be associated with hallux valgus in both men and women1, 5, 12, 16 although at least one study found no association between hallux valgus and pain or functional limitation17. Prior studies often adjust for foot pain in analyses but do not attempt to distinguish between hallux valgus with and without pain. Painful disorders could have different associations with risk factors compared to non-painful disorders.
Given the lack of consistent characteristics associated with hallux valgus, the purpose of this study was to determine if hallux valgus is associated with generalized foot pain, age, body mass index, foot structure, and high heel use (in women only), in large numbers of community-dwelling older men and women of the Framingham Study. Secondly, we aimed to determine the association between hallux valgus with pain at the forefoot and the covariates listed above and whether those who have the foot disorder with forefoot pain are different from those without pain at the forefoot.
Materials and Methods
Study Sample
The Framingham Foot Study cohort was comprised of two large, population-based samples of residents of Framingham, Massachusetts, USA. The majority of the cohort is comprised of members from the Framingham Study. The Framingham Study Original Cohort was formed in 1948 from a two-thirds sample of the town of Framingham, MA in order to study risk factors for heart disease18. This cohort, originally comprised of 5,209 men and women, has been followed biennially since that time. The Framingham Offspring cohort, formed in 1972, consists of 5,124 adult offspring who had a parent in the Original Cohort, and the offspring spouses19. This group has been followed every four years since cohort inception to study familial risk factors for heart disease. Members of the Framingham Study were examined for the current study either at their scheduled Framingham clinic examination or at a call-back examination.
The second population-based group was derived from census-based, random-digit dialing within the Framingham community, selecting participants who were at least 50 years of age and ambulatory. This group, consisting of 982 participants, was added to the Framingham Foot Study recruitment to increase participation by minority persons and other community members of the Framingham catchment area. Persons contacted via the random-digit dialing methodology who were interested in being part of a multiphasic physical examination (foot, osteoarthritis, bone health, general health), were invited to join the study.
From these combined population-based cohorts, the Framingham Foot Study conducted a physical examination of the foot and obtained participant history, health and symptom information, performance measures and other data via questionnaire. All Framingham Foot Study participants have given informed consent for the data collection and this study has undergone institutional review by both the Hebrew SeniorLife and the Boston University Medical Center Institutional Review Boards.
Foot Assessment
Between 2002 and 2008, we used a validated foot examination with specific criteria to assess foot pain, foot symptoms and presence of specific structural foot disorders and conditions. Clinical examiners, trained by a podiatrist, performed all foot examinations. Our study examiners received training from a podiatric physician to help identify several specific foot disorders, including hallux valgus. The specific foot disorders under study were included in a “foot atlas” used as a reference tool by the examiners. While grades of the foot disorders were not quantified, the training and reference materials were sufficient to reliably identify foot disorders as present or absent across examiners. All participants were ambulatory and cognitively intact. Hallux valgus, foot pain and high heel shoe use (in women only) were assessed in the men and women of the population-based Framingham Foot Study. Plantar pressure data while standing were also obtained from the study participants. In 1998, the reliability of the foot exam was tested in elderly residents of a long-term care facility (mean age 89). Comparisons of examiners produced kappas >0.85 (all p<.01). All domains tested in the foot exam had excellent reliability, both inter-observer and intra-observer, indicating that study criteria for specific foot disorders and self-reported foot pain were reliable20, 21.
Hallux valgus
Presence or absence of hallux valgus was evaluated based upon visual inspection and considered to be present if the weight bearing angle of the hallux towards the lesser toes was observed to be greater than 15 degrees. Examiners used a laminated depiction of the angle to determine if the deviation of the hallux was greater than 15 degrees3-5, 22-25.
Hallux valgus with pain
Hallux valgus with pain was defined by a creating a 4-category variable to represent the presence or absence of pain and hallux valgus. For this variable, pain was defined by the report of pain, aching or stiffness on most days in toes or forefoot. Participants were shown a picture of the foot and asked to identify areas where they experienced pain, aching or stiffness. If toes or forefoot were identified, the participant would be defined as having pain. Hallux valgus was defined as described above. Four categories were then created: 1) pain and no hallux valgus (Pain Only); 2) no pain and hallux valgus (HV Only); 3) pain and hallux valgus (Pain & HV); and 4) no pain and no hallux valgus (referent).
Foot structure
Foot structure was defined using the Modified Arch Index (MAI)26 and determined by collecting plantar pressure scans during standing. The MAI is correlated with other measures of foot posture, notably navicular height27 and arch height26. We used the Tekscan Matscan system (Tekscan Inc, Boston, MA), a 5-mm thick floor mat, sampled at 40 Hz for plantar pressure data collection. The reliability of the Matscan system has been described in detail previously28.
From the plantar pressure scan, the foot, not including the toes, is divided into thirds along the longitudinal axis (Figure 129). To calculate the MAI, the plantar pressure in the arch (area B) is divided by pressure in the entire foot, not including the toes (areas A+B+C) (see Figure 1)26. For each foot separately, foot structure was classified based on sex-specific quintile distribution of the MAI scores. Using the entire distribution of Framingham Foot Study participants, cavus foot structure (high arch) was defined as the lowest 20%; normal foot structure (referent) was defined as the middle 60%, and planus foot structure (low arch) was defined as highest 20% of the MAI values. In order to determine an overall category of foot structure for each participant, the “worst” foot was included in the analysis. If both feet were not categorized the same, we chose the foot for which the MAI value was closest to the extremes of the distribution. That is, if one foot was normal and the other was planus or cavus, we chose the planus or cavus foot to represent the participant. If one foot was planus and the other was cavus, we chose the foot with the MAI value closest to the extremes of the distribution to represent the participant. The cut-off scores to define each category were: cavus (<0.030), rectus (0.031-0.163) and planus (>0.163).
Figure 1.
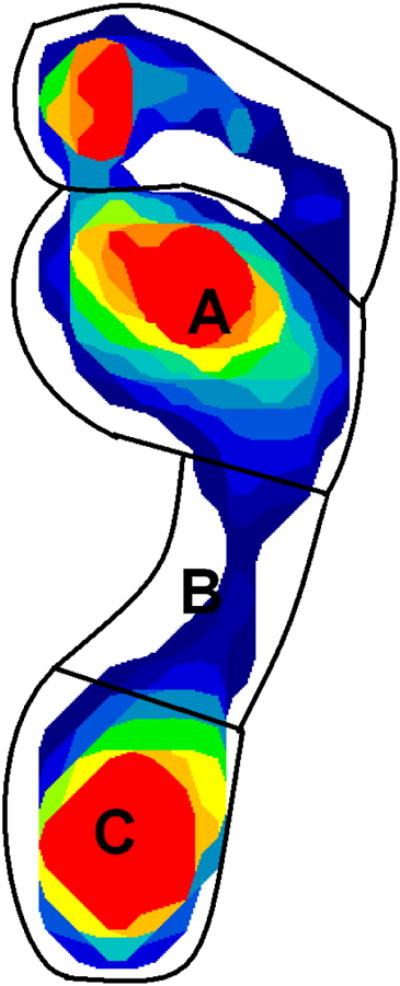
An example of a plantar pressure scan with the divisions of the foot used to calculate the modified arch index as B/(A+B+C).
(Note: Figure previously published by Riskowski JL, et al. Associations of Foot Posture and Function to Lower Extremity Pain: The Framingham Foot Study. Arthritis Care Res (Hoboken). 2013 Jun 5. doi: 10.1002/acr.22049. – Use with permission)
Generalized foot pain
Generalized foot pain was measured using a National Health and Nutrition Examination Survey (NHANES)-based query about foot pain: “on most days, do you have pain, aching or stiffness in either of your feet?” Responses included: no; yes, left foot only; yes, right foot only; yes, both feet; yes, not sure which side; and unknown. For this analysis, responses were collapsed into two groups: yes, pain in one or both foot; or no, no pain in either foot. All participants responded with either yes or no.
High Heeled Shoe Use
From a list of shoewear types, women were asked to choose their one most regularly worn shoe type during the current time frame and across past age groupings (ages 20-29, 30-44, 45-65). If “high heeled shoe” was chosen from the list as the type of shoe currently worn most frequently, participants were categorized as “current high heel user”. Past high heeled shoe use was categorized into three groups: Always, Sometimes, and Never. If a participant reported high heeled shoes as the typical shoe worn at ages 20-29 years, 30-44 years, and 45-65 years, then her past high heeled shoe use was categorized as wearing high heeled shoes “always”. If a participant chose high heeled shoes as the main shoe during some, but not all, of the three age categories, her past high heeled shoe use was categorized as wearing high heeled shoes “sometimes” in the past. If a participant did not choose high heeled shoes as the main shoe at any age category, her past high heeled shoe use was categorized as “never”.
Other characteristics
We also examined age and body mass index (BMI) for their association with hallux valgus. Age (years) at time of exam was recorded and categorized by 10-year increments. Weight in pounds was measured using a standardized balance beam scale and recorded to the nearest ½ pound. Height (without shoes) was measured in inches using a calibrated stadiometer and recorded to the nearest ¼ inch. BMI was calculated from these measurements and categorized into three groups for analysis: <25 kg/m2 (referent), 25-30 kg/m2; >30 kg/m2.
Statistical Analysis
Descriptive statistics were generated overall and separately for men and women. Sex-specific multivariate logistic models were performed to examine the association between presence of hallux valgus and age, BMI categories, generalized foot pain, foot structure category and current and past high heel use in women. To examine the association between the 4-category outcome of hallux valgus with pain and age, BMI categories, foot structure category and current and past high heel use in women, we used sex-specific multinomial logistic regression. All analyses were conducted using the SAS statistical analysis package (SAS Institute Inc., Cary, NC, U.S.A.; version 9.3) and the alpha level was set to 0.05.
Results
Of the 3429 members of the Framingham Foot Study, several participants were excluded from this analysis due to missing data: 341 were missing plantar pressure data, while others were missing data on BMI (n=7), foot pain (n=2), and hallux valgus (n=2). The remaining 1352 men and 1725 women had a mean age of 66 ± 10.5 years (range 36-100 years). Hallux valgus was present in 22% of the men and 44% of the women. The distributions of characteristics under study are shown in Table 1.
Table 1. Characteristics of Framingham Foot Study Members.
| Men (n=1352) | Women (n=1725) | |
|---|---|---|
| Age (years ± SD) | 66 ± 10.1 | 66 ± 10.8 |
| BMI (kg/m2± SD) | 29 ± 4.7 | 28 ± 5.9 |
| BMI <25 (referent) (n, %) | 252 (19) | 573 (33) |
| BMI 25-30 (n, %) | 617 (46) | 615 (36) |
| BMI >30 (n, %) | 483 (36) | 537 (31) |
| Hallux Valgus (n, %) | 295 (22) | 751 (44) |
| Foot pain (yes/no) (n, %) | 245 (18) | 512 (30) |
| Hallux valgus with pain | ||
| No pain & No HV (n, %) | 938 (69) | 782 (45) |
| Pain & No HV (n, %) | 119 (9) | 192 (11) |
| No pain & HV (n, %) | 254 (19) | 558 (32) |
| Pain and HV (n, %) | 41 (3) | 193 (11) |
| Foot structure | ||
| Rectus (normal) (n, %) | 601 (44) | 772 (45) |
| Cavus (high arch) (n, %) | 350 (26) | 493 (29) |
| Planus (low arch) (n, %) | 401 (30) | 460 (27) |
| High heel use (women only) | ||
| Current (n, %) | - | 79 (5) |
| Past | ||
| Never (n, %) | - | 744 (43) |
| Some (n, %) | - | 686 (40) |
| Always (n, %) | - | 295 (17) |
Those missing plantar pressure data were of similar age (68 ± 11.6 years), similar BMI (28.5 ± 6.0 kg/m2) and similar percent women (57%) compared to those who were not missing plantar pressure data. Additionally, women missing these data were similar in terms of prevalence of hallux valgus, foot pain, BMI>30 and high heeled shoe use. Men who were missing plantar pressure data had slightly higher prevalence of foot pain and BMI>30, with similar prevalence of hallux valgus. Since participants who were missing data were very similar to those not missing these data, it is unlikely that the missing data have biased our results.
Hallux Valgus
Table 2 shows odds ratios and 95% confidence intervals for the associations between the examined characteristics and hallux valgus by sex. Odds ratios shown are adjusted for all other covariates in the model. Having foot pain increased the odds of having hallux valgus by approximately 40% in both women and men (all p<0.05), even after adjusting for other factors. BMI > 30 was inversely associated with hallux valgus in both sexes, decreasing the odds by 33-45% (p<0.05). Older age was associated with increased odds of hallux valgus in women (p<.0001) and was borderline significant in men (p=0.07). Current high heel use was not associated with hallux valgus in women and did not contribute to the model; thus, it is not reported in the results. Despite this, women who reported wearing high heels as the main shoe during ages 20-64 years (always) had increased odds of hallux valgus by 47% (p=0.01), after adjusting for the other factors. There was a suggested 24% increased odds of hallux valgus in the “sometimes” high heel use group but it was borderline significant (p=0.05). We found no significant associations between hallux valgus and foot structure in men, although cavus compared to normal foot structure did show a protective association with hallux valgus in women (p=0.02).
Table 2. Odds Ratios (95% Confidence Intervals) for the Association* Between Examined Characteristics and Hallux Valgus.
| Men (n=1352) | Women (n=1725) | |
|---|---|---|
| Age (10 year increments) | 1.13 (0.99, 1.28) | 1.27 (1.15, 1.40) |
| BMI, kg/m2 | ||
| <25 (referent) | 1.0 | 1.0 |
| 25-30 | 0.86 (0.61,1.22) | 0.88 (0.69.1.12) |
| >30 | 0.67 (0.46,0.98) | 0.55 (0.42,0.72) |
| Foot pain (yes/no) | 1.41 (1.02,1.94) | 1.43 (1.16,1.78) |
| Foot structure | ||
| Normal (referent) | 1.0 | 1.0 |
| Cavus | 0.87 (0.63,1.21) | 0.74 (0.58,0.95) |
| Planus | 1.00 (0.73,1.37) | 1.21 (0.94,1.55) |
| Past High Heel Use | ||
| Never (referent) | - | 1.0 |
| Some | - | 1.24 (1.00,1.54) |
| Always | - | 1.47 (1.09,1.97) |
adjusted for all other risk factors
Hallux valgus with pain
Table 3 shows odds ratios and 95% confidence intervals for the results of the multinomial logistic regression examining the associations between the examined characteristics and the 4-category outcome of hallux valgus with pain by sex. In women, compared to those with neither condition, a 10 year increase in age and a planus foot structure was associated with increased odds of having Pain & HV by 24% (p=0.008) and 48% (p=0.06), respectively. Additionally, increased age and any high heel use increased the odds of HV Only by 27-58% in women only. BMI>30 and cavus foot structure was associated with a decreased odds of HV Only. Finally, increased BMI increased the odds of Pain Only, with odds ratios between 1.88 and 2.83. There were no statistically significant associations between hallux valgus with pain and the factors of interest in men, although we did see a borderline statistically significant increased odds of HV Only of 15% with increased age and a borderline protective association with HV Only and BMI>30 of 33%.
Table 3. Odds Ratios (95% Confidence Intervals) for the Association1 Between Examined Characteristics and Hallux Valgus with Pain at the Forefoot.
| Pain and HV2 | HV Only2 | Pain Only2 | |
|---|---|---|---|
| Men | |||
|
| |||
| 10 yr increased age | 1.13 (0.83, 1.53) | 1.15 (1.00, 1.31) | 1.18 (0.98, 1.43) |
| BMI categories | |||
| BMI 25-30 vs. <25 | 0.80 (0.33, 1.91) | 0.87 (0.60, 1.27) | 1.13 (0.63, 2.03) |
| BMI>30 vs. <25 | 0.88 (0.35, 2.18) | 0.67 (0.44, 1.01) | 1.35 (0.74, 2.46) |
| Foot structure | |||
| cavus vs. normal | 0.69 (0.29, 1.63) | 0.83 (0.59, 1.18) | 0.63 (0.37, 1.08) |
| planus vs. normal | 1.27 (0.62, 2.59) | 0.99 (0.71, 1.39) | 1.15 (0.75, 1.77) |
|
| |||
| Women | |||
|
| |||
| 10 yr increased age | 1.24 (1.06, 1.45) | 1.27 (1.14, 1.42) | 0.99 (0.84, 1.17) |
| BMI categories | |||
| BMI 25-30 vs. <25 | 1.40 (0.95, 2.08) | 0.90 (0.69, 1.17) | 1.88 (1.19, 2.97) |
| BMI>30 vs. <25 | 1.07 (0.68, 1.67) | 0.62 (0.46, 0.84) | 2.83 (1.78, 4.50) |
| Foot structure | |||
| cavus vs. normal | 1.08 (0.73, 1.60) | 0.68 (0.52, 0.90) | 1.12 (0.74, 1.69) |
| planus vs. normal | 1.48 (0.99, 2.21) | 1.27 (0.96, 1.68) | 1.45 (0.99, 2.14) |
| Past High Heel Use | |||
| always vs. never | 1.44 (0.91, 2.29) | 1.58 (1.13, 2.22) | 1.29 (0.78, 2.13) |
| some vs. never | 0.92 (0.64, 1.32) | 1.37 (1.07, 1.75) | 1.05 (0.74, 1.49) |
adjusted for all other risk factors
compared to no pain at the forefoot and no hallux valgus
Discussion/Conclusions
In our population-based study, the presence of hallux valgus (not distinguishing between hallux valgus with or without pain) was associated with increased age and foot pain, and inversely associated with BMI in both men and women. In women, hallux valgus was also associated with past use of high heel shoes and inversely associated with cavus foot structure. These associations remained in those who had hallux valgus without pain at the forefoot, compared to those having neither condition, when examining the four-category outcome of hallux valgus with pain, although of borderline significance in men. In women only, we saw additional increased odds of having both hallux valgus and pain at the forefoot with increased age and planus foot structure and increased odds of pain at the forefoot with no hallux valgus and increased BMI.
In agreement with previous studies2, 4, 5, we found that, in both ways that we defined hallux valgus (with and without considering the presence of pain), hallux valgus was associated with increased age, although this is contrary to two prior reports1, 3. Although many clinicians have been taught that the risk of hallux valgus increases as a person ages, two studies have reported no association between older age and hallux valgus1, 3, while others have found a significant association between older age and hallux valgus2, 4, 5, including a study of historical remains from the 5th through 17th centuries in France2. These conflicting results could be due to different distributions of age across the various studies.
A previous study of 600 MOBILIZE Boston cohort participants found that obesity (BMI≥30 kg/m2) was associated with a decreased odds of hallux valgus in women, while finding a non-significant, but increased risk of hallux valgus with increasing body mass index in men3. We found that obesity (BMI>30 kg/m2) was associated with a decreased odds of hallux valgus both when considering the presence of hallux valgus and also the second definition of hallux valgus without pain at the forefoot in both women and men in our study, which is similar to the associations seen in the MOBILIZE Boston cohort in women. The differences seen in men may be due to the fact that men in the Framingham Foot Study were more obese (36%) compared to the men in the MOBILIZE cohort (21%).
One study reported a higher prevalence of hallux valgus in men2 while others have reported higher prevalence in women1, 4-6. Marfart speculates that the higher prevalence of hallux valgus found in the 5th through 17th century men may have been due to the heeled and leather boots that were worn during those times2. A few studies have examined shoewear and found high heeled shoes, in women3, 7-9, improper fitting shoes in men, women and children8, 10 and increased numbers of years wearing shoes to be associated with hallux valgus11. Similarly, we also found that regular past use of high heeled shoes is associated with increased odds of hallux valgus (without considering pain at the forefoot), and in those who had hallux valgus without pain at the forefoot, which agrees with previous findings regarding high heel shoes. Although current high heel use was not associated with hallux valgus in our study, the association with past high heel use highlights the importance of limiting use earlier in life.
We found that foot structure was not associated with hallux valgus in men. In women, cavus foot structure was protective against hallux valgus and against hallux valgus without pain at the forefoot. Additionally in women, planus foot structure was associated with increased odds of having hallux valgus with pain at the forefoot. This is contrary to the results found in the prior study by Nguyen et al, where pes planus foot structure was associated with hallux valgus in men3. This could be due to differing definitions used to characterize foot structure or to the fact that pain was not considered in conjunction with hallux valgus. Nguyen et al used the Staheli Arch Index27, which is the ratio of the arch width to rearfoot width, as opposed to the ratio of arch pressure to rearfoot pressure of the MAI. With the MAI, there is a higher coefficient of variation, which increases the ability to detect foot structure, and may better characterize how the foot functions relative to the Staheli Arch Index. Further, Nguyen et al. only evaluated if participants had planus foot structure (dichotomized) and used a referent population that included both cavus and rectus foot structures. Combining participants with both cavus and rectus foot structure in order to compare to planus foot structure may help explain the differences in results.
This study has important strengths and limitations that should be acknowledged. We are limited by the fact that this is a cross-sectional study of hallux valgus and potential risk factors which cannot determine temporality and thus cannot comment on causality. We are also limited by our definition of foot pain in our ability to determine whether the foot pain used to define hallux valgus with pain was actually pain caused by the hallux valgus. While we used pain at the toes and forefoot to define hallux valgus with pain, it is possible that the hallux valgus caused pain in other parts of the foot or that pain in the 1st metatarsophalangeal joint was not captured by pain at the toes or forefoot. Additionally, our definition of hallux valgus is not radiographically based. Despite this, we used a common, visual definition that has been used in other studies and described in clinical text books3-5, 23, 30, 31. There is the potential for recall bias of high heel shoe use, especially in past shoewear groups, since we are asking participants to remember what shoe they were wearing decades in the past. However, participants were not asked to link an outcome to their shoewear, perhaps minimizing the likelihood of bias in the recall. Misclassification remains a problem as we used 3 grouped ages to anchor the responses, which may introduce misclassification into the groups of high heeled shoe use. Also, the Framingham study is primarily Caucasian, so our results are not generalizable beyond this racial group. This study also has important strengths. We have a large population-based sample which includes both men and women. We conducted a validated foot examination as well as self-report questionnaire of pain. Additionally, we determined foot structure based on the MAI using foot pressure data as opposed to using a simple clinical impression of foot structure.
The foot types that are most likely to be observed in a clinical setting are those that include pain (pain only and hallux valgus with pain), and the findings from this study, particularly among women, are consistent with current weight loss interventions for pain management and shoewear recommendations for hallux valgus, such as sufficient arch support and avoidance of high heel shoes. Future research is needed determine whether the hallux valgus only and the hallux valgus with pain conditions are truly different phenotypes or if those who have hallux valgus only will develop forefoot pain over time. If the latter scenario is the case, modifying risk factors associated with hallux valgus only may be important for preventing the development of forefoot pain.
In conclusion, we saw strong relations between hallux valgus and foot pain in both men and women. In women only, age and high heel shoe use were strongly related, with additional protective associations with cavus foot structure and obesity. Increased BMI was associated with decreased odds of hallux valgus in both men and women. In teasing apart the relation between pain and hallux valgus, we found no associations in men. However, in women with hallux valgus without pain at the forefoot followed the same trends as the hallux valgus analysis which ignored the presence of pain. Women with both pain at the forefoot and hallux valgus had an association only with increased age and planus foot structure, with the latter association not seen when the presence of pain was not considered. Therefore, it is important to consider those with pain at the forefoot and toes differently than those who do not have pain when examining hallux valgus. Future studies should address additional factors of interest, such as weight bearing load during occupational demands and pregnancies32, as well as examination of the specific structures of shoewear.
Significance and Innovations.
Hallux valgus is common and associated with having foot pain in men and women, and increased age and past high heel shoe use in women.
The risk of hallux valgus is greater in both men and women when body mass index is lower and is less in women who have a cavus foot structure.
Those with hallux valgus with and without pain should be evaluated differently in future research.
Acknowledgments
Funding for this project was provided by: Beth Israel Deaconess Medical Center/Harvard NIH T32 Translational Research in Aging Predoctoral Training Program; the ACR REF/Abbott Graduate Student Achievement Award; the National Institute of Arthritis and Musculoskeletal and Skin Diseases and the National Institute on Aging (R01-AR47853); and the National Heart, Lung and Blood Institute's Framingham Heart Study (N01-HC-25195); Arthritis Foundation Postdoctoral Fellowship Award and National Center for Advancing Translational Sciences, National Institutes of Health, through Grant KL2TR000084
Contributor Information
Virginia A. Casey, Email: virginiacasey@hsl.harvard.edu.
Yvonne M. Golightly, Email: golight@email.unc.edu.
Marian T. Hannan, Email: hannan@hsl.harvard.edu.
References
- 1.Cho NH, Kim S, Kwon DJ, Kim HA. The prevalence of hallux valgus and its association with foot pain and function in a rural Korean community. J Bone Joint Surg Br. 2009;91:494–8. doi: 10.1302/0301-620X.91B4.21925. [DOI] [PubMed] [Google Scholar]
- 2.Mafart B. Hallux valgus in a historical French population: paleopathological study of 605 first metatarsal bones. Joint Bone Spine. 2007;74:166–70. doi: 10.1016/j.jbspin.2006.03.011. [DOI] [PubMed] [Google Scholar]
- 3.Nguyen US, Hillstrom HJ, Li W, et al. Factors associated with hallux valgus in a population-based study of older women and men: the MOBILIZE Boston Study. Osteoarthritis Cartilage. 2010;18:41–6. doi: 10.1016/j.joca.2009.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res. 2010;3:21. doi: 10.1186/1757-1146-3-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Roddy E, Zhang W, Doherty M. Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum. 2008;59:857–62. doi: 10.1002/art.23709. [DOI] [PubMed] [Google Scholar]
- 6.Menz HB, Lord SR. Foot pain impairs balance and functional ability in community-dwelling older people. J Am Podiatr Med Assoc. 2001;91:222–9. doi: 10.7547/87507315-91-5-222. [DOI] [PubMed] [Google Scholar]
- 7.Cong Y, Cheung JT, Leung AK, Zhang M. Effect of heel height on in-shoe localized triaxial stresses. J Biomech. 2011;44:2267–72. doi: 10.1016/j.jbiomech.2011.05.036. [DOI] [PubMed] [Google Scholar]
- 8.Menz H, Morris M. Footwear Characteristics and Foot Problems in Older People. Gerontology. 2005;51:346–51. doi: 10.1159/000086373. [DOI] [PubMed] [Google Scholar]
- 9.Yu J, Cheung JT, Fan Y, Zhang Y, Leung AK, Zhang M. Development of a finite element model of female foot for high-heeled shoe design. Clin Biomech (Bristol, Avon) 2008;23(Suppl 1):S31–8. doi: 10.1016/j.clinbiomech.2007.09.005. [DOI] [PubMed] [Google Scholar]
- 10.Klein C, Groll-Knapp E, Kundi M, Kinz W. Increased hallux angle in children and its association with insufficient length of footwear: a community based cross-sectional study. BMC Musculoskelet Disord. 2009;10:159. doi: 10.1186/1471-2474-10-159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shine IB. Incidence of Hallux Valgus in a Partially Shoe-Wearing Community. Br Med J. 1965;1:1648–50. doi: 10.1136/bmj.1.5451.1648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kernozek TW, Elfessi A, Sterriker S. Clinical and biomechanical risk factors of patients diagnosed with hallux valgus. J Am Podiatr Med Assoc. 2003;93:97–103. doi: 10.7547/87507315-93-2-97. [DOI] [PubMed] [Google Scholar]
- 13.Mickle KJ, Munro BJ, Lord SR, Menz HB, Steele JR. Gait, balance and plantar pressures in older people with toe deformities. Gait Posture. 2011;34:347–51. doi: 10.1016/j.gaitpost.2011.05.023. [DOI] [PubMed] [Google Scholar]
- 14.Martinez-Nova A, Sanchez-Rodriguez R, Perez-Soriano P, Llana-Belloch S, Leal-Muro A, Pedrera-Zamorano JD. Plantar pressures determinants in mild Hallux Valgus. Gait Posture. 2010;32:425–7. doi: 10.1016/j.gaitpost.2010.06.015. [DOI] [PubMed] [Google Scholar]
- 15.Hannan MT, Menz HB, Jordan JM, Cupples LA, Cheng CH, Hsu YH. Hallux valgus and lesser toe deformities are highly heritable in adult men and women: The Framingham foot study. Arthritis Care Res (Hoboken) 2013 doi: 10.1002/acr.22040. NA. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Menz HB, Morris ME. Determinants of Disabling Foot Pain in Retirement Village Residents. Journal of the American Podiatric Medical Association. 2005;95:573–9. doi: 10.7547/0950573. [DOI] [PubMed] [Google Scholar]
- 17.Badlissi F, Dunn JE, Link CL, Keysor JJ, McKinlay JB, Felson DT. Foot musculoskeletal disorders, pain, and foot-related functional limitation in older persons. J Am Geriatr Soc. 2005;53:1029–33. doi: 10.1111/j.1532-5415.2005.53315.x. [DOI] [PubMed] [Google Scholar]
- 18.Dawber T, Meadors G, Moore F. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health. 1951;41:279–81. doi: 10.2105/ajph.41.3.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Feinleib M, Kannel W, Garrison R, McNamara P, Castelli W. The Framingham Offspring Study. Design and preliminary data. Prev Med. 1975;4:518–25. doi: 10.1016/0091-7435(75)90037-7. [DOI] [PubMed] [Google Scholar]
- 20.Hannan M, Murabito J, Felson D, Rivinus M, Kaplan J, Kiel D. The Epidemiology of Foot Disorders and Foot Pain in Men and Women: the Framingham Study. Arthritis and Rheumatism. 2003;48:S672. abstract. [Google Scholar]
- 21.Hannan M, Zimmer J, Sullivan E, Kiel D. Physical Limitations and foot disorders in elders. Journal of the American Geriatric Society. 2001;49:S22. abstract. [Google Scholar]
- 22.Hagedorn TJ, Dufour AB, Riskowski JL, et al. Foot disorders, foot posture, and foot function: the Framingham foot study. PLoS One. 2013;8:e74364. doi: 10.1371/journal.pone.0074364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bascarevic Z, Vukasinovic ZS, Bascarevic VD, Stevanovic VB, Spasovski DV, Janicic RR. Hallux valgus. Acta Chir Iugosl. 2011;58:107–11. [PubMed] [Google Scholar]
- 24.Birrer RB, Dellacorte MP, PJ G. Common foot problems in primary care. 2nd. Philadelphia, PA: Hanley & Belfus, Inc.; 1998. [Google Scholar]
- 25.Menz HB. Foot problems in older people: Assessment and Management. Philadelphia, PA: Elsevier; 2008. [Google Scholar]
- 26.Chu WC, Lee SH, Chu W, Wang TJ, Lee MC. The use of arch index to characterize arch height: a digital image processing approach. IEEE Trans Biomed Eng. 1995;42:1088–93. doi: 10.1109/10.469375. [DOI] [PubMed] [Google Scholar]
- 27.Shiang TY, Lee SH, Lee SJ, Chu WC. Evaluating different footprint parameters as a predictor of arch height. IEEE Eng Med Biol Mag. 1998;17:62–6. doi: 10.1109/51.731323. [DOI] [PubMed] [Google Scholar]
- 28.Zammit GV, Menz HB, Munteanu SE. Reliability of the TekScan MatScan(R) system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. J Foot Ankle Res. 2010;3:11. doi: 10.1186/1757-1146-3-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Riskowski J, Dufour A, Hagedorn T, Hillstrom H, Casey V, Hannan M. Associations of foot posture and function to lower extremity pain: The Framingham Foot Study. Arthritis Care Res (Hoboken) 2013 doi: 10.1002/acr.22049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Birrer RB, Dellacorte MP, Grisafi PJ. Common foot problems in primary care. 2nd. Philadelphia, PA: Hanley & Belfus, Inc.; 1998. [Google Scholar]
- 31.Menz HB. Foot problems in older people: Assessment and Management. Philadelphia, PA: Elsevier; 2008. [Google Scholar]
- 32.Segal NA, Boyer ER, Teran-Yengle P, Glass NA, Hillstrom HJ, Yack HJ. Pregnancy leads to lasting changes in foot structure. Am J Phys Med Rehabil. 2013;92:232–40. doi: 10.1097/PHM.0b013e31827443a9. [DOI] [PMC free article] [PubMed] [Google Scholar]