

Abstract
The dentigerous cysts are the common cause that inhibits the eruption of the teeth. Large dentigerous cysts can cause pathological fractures in mandible. Temporary or permanent inferior alveolar and lingual nerve damage can occur associated with deeply impacted third molar surgery. We treated the dentigerous cyst arised from deeply impacted mandibular third molar with orthodontic extraction combined with the marsupialization therapy. This orthodontic-surgical procedure reduced the risk of nerve damage and pathological fracture of the mandible.
Keywords: Orthodontic extrusion, Third molar, Marsupialization, Dentigerous cyst
A dentigerous cyst is often detected as a localized swelling of the alveolar bone, and associated with an impacted tooth. A painless and progressive enlargement of the jaw is usually revealed from the history of the patient. This may cause destruction of the bone, displacement of adjacent teeth, resorption of their roots [1], and pathological fractures. Marsupialization therapy is suggested to prevent the complications associated with a large odontogenic cyst, and to promote the spontaneous eruption of the involved tooth within the cyst. However, tooth eruption does not always occur spontaneously after marsupialization [2].
Orthodontic traction of the impacted tooth has been performed after marsupialization of a large cyst [3]. When the third molar is deeply impacted within the cyst cavity, this combined orthodontic-surgical procedure may reduce the risk of damage to the inferior alveolar nerve. This approach may facilitate the extraction and may also reduce the possibility of pathological fractures [4].
In this case report, we present the treatment of a deeply impacted third molar associated with a dentigerous cyst with orthodontic extraction combined with marsupialization therapy. This orthodontic-surgical procedure reduced the risk of nerve damage and the risk of pathological fracture in the mandible.
Case Report
A healthy 33-year-old woman was referred to our clinic in April, 2010 for treatment of a large radiolucent lesion associated with a deeply impacted mandibular third molar. Panoramic radiograph showed a close proximity between mandibular third molar and mandibular canal, and also a large cyst (Fig. 1).
Fig. 1.
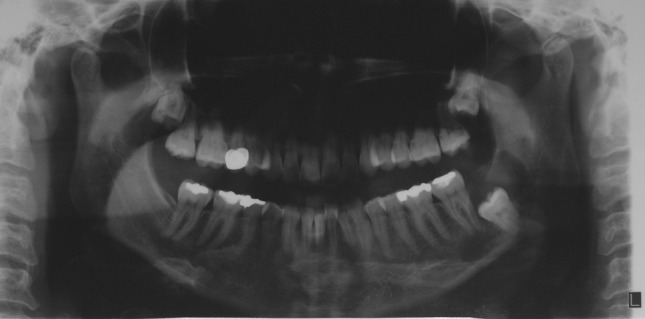
Preoperative panoramic radiography shows the deeply impacted third molar related with dentigerous cyst
Considering the high risk of mandibular nerve damage, and mandibular fracture, the enucleation of cyst with the extraction of tooth was not preferred. After consultation with the orthodontist, a combined surgical-orthodontic treatment including the extrusion of the tooth to a ‘safe vertical position’ and marsupialization of the cyst were planned.
Under local anesthesia, a window was created distally to the second molar, and the crown of impacted third molar was exposed. Posterior teeth adjacent to the third molar were bonded with fixed orthodontic appliances and 0.16 × 0.22 inch rectangular stainless steel arch wire was placed passively. The teeth were then figurated to provide a stable anchorage (Fig. 2). Then a button was bonded to the buccal surface of the third molar (Fig. 3). To apply extrusive force to the third molar a spring was designed and placed in the auxiliary tube of the second molar. Extrusive force was applied with elastic thread between the spring and the third molar button. The biopsy specimen revealed dentigerous cyst.
Fig. 2.

Preoperative intraoral appearance after lower left posterior teeth were bonded with fixed orthodontic appliances
Fig. 3.

Intraoperative appearance shows the bonded button to the buccal surface of the tooth
The movement of the third molar and decreasing of size of the cyst was observed every month, and evaluated with panoramic radiography. The extrusive force was reactivated if needed (Fig. 4).
Fig. 4.
Panoramic radiography, 1 month after the first surgery
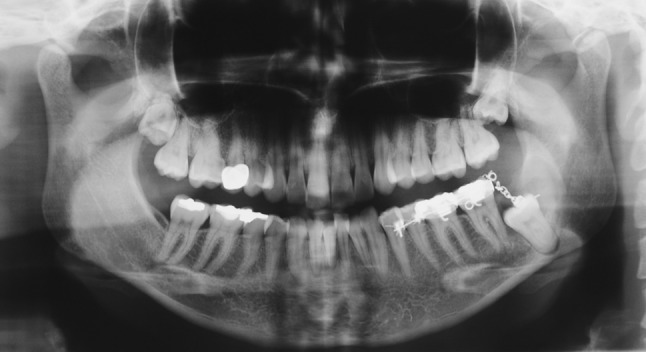
After 4 months, panoramic radiography showed a sufficient extrusion of the tooth and shrinkage of the cyst (Fig. 5). Because the crown of the second molar became an obstacle on the eruption pathway, the orthodontic extrusion failed at the cervical level of the second molar. Therefore, a second surgical operation was performed to extract the tooth and enucleate the cyst under local anesthesia. Healing was uneventful, and clinical and radiographic examinations showed good results 3 months after the extraction (Fig. 6).
Fig. 5.

Panoramic radiography before the second surgery shows a sufficient extrusion of tooth and shrinkage of the cyst
Fig. 6.

Panoramic radiography, 3 months after the extraction
Discussion
Dentigerous cysts are the most common type of developmental odontogenic cysts. By definition, a dentigerous cyst is attached to the enamel–cementum junction of the tooth cervix and encloses the crown of the unerupted tooth, most commonly third molars and maxillary canines. This cyst can achieve significant size, but rarely, causes pathologic fracture of the jaw [5].
Several treatment options have been suggested including complete enucleation and marsupialization. Marsupialization is a conservative surgical approach for the treatment of a dentigerous cyst that decreases the risk of jaw fractures and nerve damage [6]. When preservation of the impacted teeth is planned, marsupialization is a rather conservative treatment option [7], and has the advantage of promoting spontaneous eruption of the involved tooth within the cyst [2]. However, patients aged over 10 years would not be expected to have spontaneous eruption of an impacted tooth, indicating the need for orthodontic treatment to guide occlusion or surgical removal of the entire cyst with the impacted tooth [8]. Considering the age of the patient, and deep location of the impacted third molar at the base of the mandible in association with the inferior alveolar nerve, orthodontic extrusion combined with marsupialization is thought to be the appropriate treatment for our case. Extrusion of the tooth and shrinkage of the cyst was observed after 4 months. Although the orthodontic extrusion failed at the cervical level of the second molar crown due to inclination of eruption pathway, a sufficient extrusion was achieved eliminating the risk of nerve damage and pathological fracture of the mandible. Therefore, a second surgical operation was performed to extract the tooth and enucleate the cyst under local anesthesia. Healing was uneventful, and clinical and radiographic examinations showed good results 3 months after the extraction.
The advantages of a combined orthodontic and surgical extraction of an impacted third molar are those which can be performed under local anesthesia, and is a conservative method for soft and hard tissues. Furthermore, it does not entail the risk of mandibular fracture and decreases the risk of injuring inferior alveolar nerve. In the presented case here, pathological fracture did not occur after the extraction of tooth. Transient paresthesia occurred and improved rapidly.
Combined orthodontic-surgical technique has a few minor disadvantages. The procedure requires two surgical operations, and is contraindicated if the tooth is ankylosed [9]. It may be time-consuming, and requires the selection of co-operative patient. Besides, the orthodontic appliances can be uncomfortable for the patients [9, 10]. In our case, the appliance irritated the adjacent mucosa causing pain, however the use of a periodontal pack eliminated the discomfort.
In conclusion, treatment of a deeply impacted third molar associated with a large dentigerous cyst may develop complications such as mandibular fractures and nerve injury. These complications should be considered before the treatment plan is determined. Combined orthodontic and surgical therapy is a safe method for the cases which have a deeply impacted third molar associated with a cystic lesion.
References
- 1.Lucas RB. Pathology of tumours of the oral tissues. London: Churchill Livingstone; 1984. [Google Scholar]
- 2.Hyomoto M, Kawakami M, Inoue M, Kirita T. Clinical conditions for eruption of maxillary canines and mandibular premolars associated with dentigerous cysts. Am J Orthod Dentofac Orthop. 2003;124:515–520. doi: 10.1016/j.ajodo.2003.04.001. [DOI] [PubMed] [Google Scholar]
- 3.Clauser C, Zuccati G, Barone R, Villano A. Simplified surgical-orthodontic treatment of a dentigerous cyst. J Clin Orthod. 1994;28:103–106. [PubMed] [Google Scholar]
- 4.Checchi L, Alessandri Bonetti G, Pelliccioni G. Removal of high risk impacted mandibular third molars utilizing a combine surgical-orthodontic approach. J Am Dent Assoc. 1996;127:1214–1217. doi: 10.14219/jada.archive.1996.0413. [DOI] [PubMed] [Google Scholar]
- 5.Regezi JA. Oral pathology—clinical pathologic correlations. Philadelphia: Elsevier Science; 2003. [Google Scholar]
- 6.Pogrel MA. Treatment of keratocysts: the case for decompression and marsupialization. J Oral Maxillofac Surg. 2005;63:1667–1673. doi: 10.1016/j.joms.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 7.Motamedi MHK, Talesh KT. Management of extensive dentigerous cysts. Br Dent J. 2005;198:203–206. doi: 10.1038/sj.bdj.4812082. [DOI] [PubMed] [Google Scholar]
- 8.Fujii R, Kawakami M, Hyomoto M, Ishida J, Kirita J. Panoramic findings for predicting eruption of mandibular premolars associated with dentigerous cyst after marsupialization. J Oral Maxillofac Surg. 2008;66:272–276. doi: 10.1016/j.joms.2007.06.652. [DOI] [PubMed] [Google Scholar]
- 9.Marchetti C, Bonetti GA, Pieri F, Checchi L. Orthodontic extraction: conservative treatment of impacted mandibular third molar associated with a dentigerous cyst. A case report. Quintessence Int. 2004;35:371–374. [PubMed] [Google Scholar]
- 10.Bonetti GA, Parenti SI, Checchi L. Orthodontic extraction of mandibular third molar to avoid nerve injury and promote periodontal healing. J Clin Periodontol. 2008;35:719–723. doi: 10.1111/j.1600-051X.2008.01286.x. [DOI] [PubMed] [Google Scholar]