

Abstract
Foreign bodies are often encountered by oral and maxillofacial surgeons and may present a diagnostic challenge, due to many factors such as nature of foreign body material, the size of the object, difficult access and a close anatomical relationship of the foreign body to vital structures. There are foreign bodies like glass pieces, plastic materials, wooden pieces are not seen in routine radiographs and often misdiagnosed. To reduce the chances of complications presence of foreign body in the patients head and neck region must be thoroughly investigated by the surgeon. Penetrating injuries by blunt object is rare finding in maxillofacial region. Here we present an unusual case of penetrating injury by a large machine bolt (15.0 cm) in a 7 year old child, embedded on left side of face.
Keywords: Maxillofacial injuries, Foreign bodies, Penetrating injury
Introduction
Management of foreign bodies in maxillofacial region is challenging task for trauma surgeon [1] because of factors such as the size of the object, the difficult access and a close anatomical relationship of the foreign body to vital structures [2]. They are usually a result of war injuries or operations. The foreign body removal is delayed in approximately one-third of all cases; because they are initially radio logically missed or misdiagnosed. Occasionally, foreign bodies may be retained for some time unless causing persistent and distressing symptoms [3]. The foreign body can often modify the regional anatomy. Tissue can be damaged by gun-shot wounds, or altered by scaring after an operation that resulted in an iatrogenic foreign body [2]. Inflammatory response in the tissues around a foreign body may add the difficulties [4]. There are many ways of detecting and localizing foreign bodies. Plain radiographs, computed tomograms (CT), magnetic resonance images (MRI) and ultrasound may be used, depending on their site and composition [1, 5]. The foreign body removal in the facial region implies on danger of damaging important anatomical structures. Even if it’s known the exact position from imaging data, the accurate reproduction of its position in the patient’s body can be difficult if the foreign body is not adjacent to a definitive anatomical landmark. The search for a foreign body in a larger area rather than at a definite position increases the risk of damage to adjacent structures [4].
The purpose of this report is to present a case of a foreign body in a patient’s facial region caused by impaction of large bolt attached to a machine during an accident that calls the attention of the importance of surgeon’s skill and knowledge in order to proceed for a correct treatment plan and seek help from other specialist if needed.
Case Report
A female patient aged 7 years reported to the Department of oral & maxillofacial surgery with profuse bleeding from oral and nasal cavity. On inspection a bolt about 15.0 cm long was embedded lateral to left ala of nose and on palpation intraorally it was projecting in oral cavity from posterior nasal aperture of opposite side just medial to maxillary tuberosity in oropharynx (Fig. 1). Patients relatives gave history that patient along with his entire family was travelling in a tractor-trolly that had a heavy machine that was used for farming. While on their way the tractor met with an accident with opposite side fast running truck. Due to sudden head on collision the machine slipped backward and hit the face of the child. The screws that were used for clamping the machine on floor entered left side of face and patient had profuse bleeding from nasal and oral cavity following traumatic injury. The patient was separated from the machine by unscrewing the bolt by the attendant of the patient. Immediately patient was taken to nearby hospital for first aid. After first aid the patient was referred to higher maxillofacial centre for further treatment. When patient reached to emergency unit of our hospital, patient received tetanus prophylaxis, blood sample was taken and IV line was maintained. On clinical examination there were no sign of facial fracture except penetrating injury. Patients radio graphical (PA view skull and true lateral view of face) and hematological investigations were carried out. Blood investigations revealed low hemoglobin concentration (6.5 mg%), so blood transfusion was started immediately and then patient was shifted to operation theatre for retrieval of bolt under general anesthesia. The postero anterior and lateral oblique radiographs revealed a bolt about 5.3 cm long being embedded (Fig. 2). There was injury to anterolateral wall of left maxillary sinus. During retrieval of bolt there was profuse bleeding from posterior nasal aperture which might be due to injury to descending palatine artery or pterygoid plexus. The bleeding was controlled by hot saline pack. After the foreign body’s removal, the soft tissues were explored, washed copiously, small pieces of bone removed and wound was sutured in planes (Fig. 3, 4). The patient received broad spectrum antibiotics for 7 days. Patient recovered post operatively without any subjective symptoms. Since the patient was from distant rural area, did not report back for follow up.
Fig. 1.

Front & Left lateral photograph of patient demonstrating embedded machine bolt
Fig. 2.
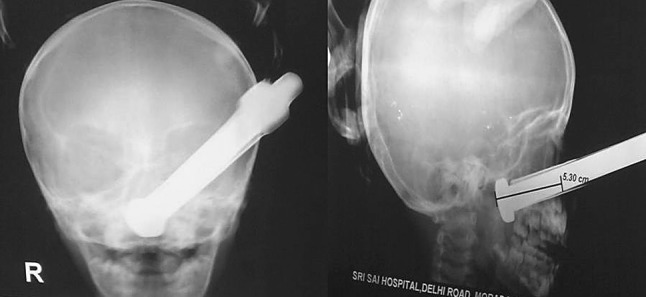
PA View skull & True lateral view demonstrating the direction and extent of penetration (orbital rim intact)
Fig. 3.

Post operative photograph of patient after suture with nasal pack
Fig. 4.

Measurement of bolt after removal, compared with 10 ml syringe (length 15.2 cm)
Discussion
While taking care of traumatized patient the first step is to stabilize the patient following Advance trauma life support (ATLS) protocol. Once the patient is stabilized, detailed examination of head & neck should be done, followed by proper surgical debridement of the lacerated-contused tissues. This evaluation must be based upon proper diagnostic aids such as plain radiography, CT (with axial and coronal projections), and Magnetic Resonance Imaging in selected cases [5]. The removal of the foreign bodies is often delayed due to missed diagnosis [3]. A foreign body may also remain asymptomatic for a long time and may present acute symptoms like Foreign body (FB) reactions and infections. Thus plain radiographs on right angles are enough to localize the foreign body in specific cases [1, 6]. In the above case, true lateral and post-anterior skull radiographs were taken.
The accurate reproduction of localization in a patient’s body was first successfully achieved in neurosurgery with the development of stereotactic methods [7]. These so-called navigation systems allow the registration of image space and physical space of the patient without a stereotactic frame [4]. In the last years, many authors have been indicating the use of the navigation systems for foreign body retrieval in facial region, especially when the FB is located close to vital structures [4, 8], failure of previous attempts at removal the foreign body, the presence of multiple foreign bodies, the desire to achieve a minimally invasive access [4], and to allow a quicker operation [8]. In our case we did not use navigation system because of superficial location of FB. For foreign body’s removal, general anesthesia is often desirable to allow endoscopy and insertion of various instruments [9]. Surgical treatment consists of removing the foreign body and reconstructing the damaged bone structures to restore the normal functionality and morphology of the involved region [6]. The treatment sequence involved approach, foreign body withdrawal, wound exploration, irrigation and suturing. Regarding wound contamination, literature revised recommend antibiotics and tetanus prophylaxis [9]. The reported case was managed following the same protocol. The entire foreign body was removed successfully, without any complications. Maxillofacial injuries with impacted bolt in situ are very rare. Considering the rarity, any experience reported in the literature appears significant. Cohen and Boyes [10] reported 37 cases of penetrating injuries with retained foreign bodies in the maxillofacial region. Our case with a bolt impacted about 5.3 cm, transgressing the three distinct anatomical sites i.e. maxillary sinus, nasal cavity, oral pharynx, is of a rare entity.
Acknowledgments
Conflict of interest
none.
Contributor Information
P. N. Tandon, Phone: +919837174271, Email: drpntandon@gmail.com
D. S. Gupta, Phone: +919411696393, Email: drdsgupta@gmail.com
Sunit K. Jurel, Phone: +919412365813, Email: dentistsj1105@yahoo.co.in
Shilpi Srivastava, Phone: +919410014224, Email: drshilpids@gmail.com.
Shalender Sharma, Phone: +919886467373, Email: sharma.shalender@rediffmail.com.
References
- 1.Krimmel M, Conelius CP, Stojadinovic S, Hoffman J, Reinert S. Wooden foreign bodies in facial injury: a radiological pitfall. Int J Oral Maxillofac Surg. 2001;30:445–447. doi: 10.1054/ijom.2001.0109. [DOI] [PubMed] [Google Scholar]
- 2.Holmes P-J, Miller JR, Gutta R, Louis PJ. Intraoperative imaging techniques: a guide to retrieval of foreign bodies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:614–618. doi: 10.1016/j.tripleo.2005.02.072. [DOI] [PubMed] [Google Scholar]
- 3.Cameron M, Phillips B. Snookered Facial infection secondary to occult foreign body. Int J Oral Maxillofac Surg. 2006;35:373–375. doi: 10.1016/j.ijom.2005.09.010. [DOI] [PubMed] [Google Scholar]
- 4.Eggers G, Haag C, Hassfeld S. Image-guided removal of foreign bodies. Br J Oral Maxillofac Surg. 2005;43:404–409. doi: 10.1016/j.bjoms.2005.01.016. [DOI] [PubMed] [Google Scholar]
- 5.Oikarinen KS, Nieminen TM, Makarinen H, Pythinen J. Visibility of foreign bodies in soft tissue in plain radiographs, computed tomography, magnetic resonance imaging, and ultrasound—an in vitro study. Int J Oral Maxillofac Surg. 1993;22:119–124. doi: 10.1016/S0901-5027(05)80818-5. [DOI] [PubMed] [Google Scholar]
- 6.Covelli E, Leonardi A, Indrizzi E, Amede DS, Fini G. Unknown posttraumatic foreign body in facial region. J Craniofac Surg. 2006;17(1):191–194. doi: 10.1097/01.scs.0000190347.45601.fa. [DOI] [PubMed] [Google Scholar]
- 7.Hitchcok E, Cowie R. Stereotactic removal of intracranial foreign bodies: review and case report. Injury. 1983;14:471–475. doi: 10.1016/0020-1383(83)90101-8. [DOI] [PubMed] [Google Scholar]
- 8.Siebegger M, Mischkoski RA, Schneider BT, Krug B, Klesper B, Zöller JE. Image guided surgical navigation for removal of foreign bodies in the head and neck. J Craniomaxillofac Surg. 2001;29(6):321–325. doi: 10.1054/jcms.2001.0254. [DOI] [PubMed] [Google Scholar]
- 9.Shinohara EH, Heringer L, Carvalho Júnior JP. Impacted knife injuries in the maxillofacial region: report of 2 cases. J Oral Maxillofac Surg. 2001;59(10):1221–1223. doi: 10.1053/joms.2001.26730. [DOI] [PubMed] [Google Scholar]
- 10.Cohen MA, Boyes-Varley G. Penetrating injuries to the maxillofacial region. J Oral Maxillofac Surg. 1986;44:197–202. doi: 10.1016/0278-2391(86)90108-4. [DOI] [PubMed] [Google Scholar]