

Abstract
Osteosarcoma (OS) is the most common nonhematolymphoid primary bone malignancy characterized by osteoid or new bone formation. Lungs and bones are the most common sites of metastases. We report a case where unusual sites of the soft tissue recurrence from OS were detected on restaging fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography scan done post 6 years of disease free interval.
Keywords: Osteosarcoma, fluorine-18 fluorodeoxyglucose, positron emission tomography/computed tomography
INTRODUCTION
Osteosarcoma (OS) is an aggressive primary bone malignancy with a high propensity for pulmonary and skeletal metastases. Metastases at other sites are rare. Unlike other malignancies such as carcinoma breast, colorectal, head and neck malignancies, lymphoma, and melanoma where the role of fluorine-18 fluorodeoxyglucose (F-18 FDG) positron emission tomography/computed tomography (PET/CT) for restaging evaluation is established, the role is yet not defined in cases of OS. In this case, we wish to demonstrate the ability of F-18 FDG PET/CT scan to detect unusual sites of disease recurrence.
CASE REPORT
A 26-year-old young gentleman, a diagnosed case of OS of right femur was treated with neoadjuvant chemotherapy followed by wide excision of the mass with prosthesis insertion. Histopathology revealed no residual viable tumor (100% necrosis). Proximal and distal bony and soft tissue cut margins were free of tumor. The patient had a disease free interval of 6 years following which he presented with a lump over the anterior abdominal wall. Fine-needle aspiration cytology of the lump was suggestive of disease recurrence [Figure 1]. Restaging F-18 FDG PET/CT revealed metastatic deposit in right paraspinal muscle at the level of C1 vertebra, muscle deposit in right arm, subcutaneous nodules in anterior abdominal wall, right lateral chest wall, left arm, serosal deposit over ascending colon and pancreatic deposit in addition to the pulmonary and bone metastases. No evidence of active disease was noted in the periprosthetic region at the operated site [Figure 2]. The patient was started on metronomic chemotherapy.
Figure 1.
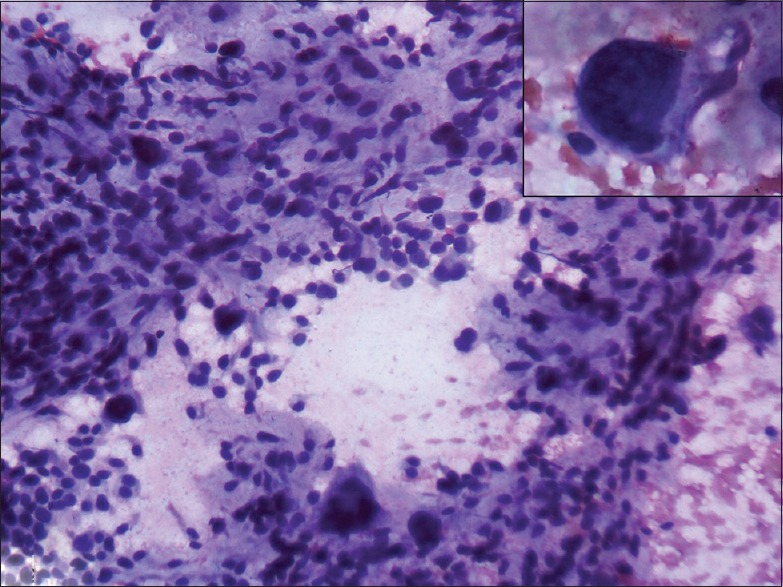
Fine-needle aspiration cytology of the anterior abdominal wall lump - H and E stained slides revealed hypercellular smear showing markedly pleomorphic/ sarcomatous cells including giant cells amidst stroma consistent with osteogenic sarcoma (×200). Insert: A large sarcomatous cell with a pleomorphic nucleus and moderate cytoplasm (×100)
Figure 2.

Maximum intensity projected image (a) revealed multiple foci of increased fluorodeoxyglucose uptake which on correlative fused axial images corresponded to subcutaneous anterior abdominal wall deposit (b), muscle deposit in right arm (c), pancreatic deposit (d), serosal deposit over ascending colon (e), sternal (f), and pulmonary metastases (g). However, no hypermetabolic focus was noted in the periprosthetic region at the operative site
DISCUSSION
Osteosarcoma is the most common nonhematolymphoid primary bone tumor arising from malignant transformation of primitive mesenchymal cells that produce osteoid or immature new bone. The peak incidence is seen in the second decade of life with slight male preponderance. Although it can affect any bone, it has a predilection for metaphyses of long bones. The most common presentation is painful swelling, occasionally with a history of trauma. The 5-year overall survival rate for primary localized OS is about 75% compared to 25-50% in cases with lung or bone metastases. Neoadjuvant chemotherapy followed by surgical resection and adjuvant chemotherapy form the mainstay of treatment.[1] Tumor site, size, metastases at presentation, response to chemotherapy, and surgical remission are some of the known independent prognostic factors.[2]
Recurrence is commonly observed within 5 years in approximately 95% cases. However, recurrence after 5 years is very rare and seen only in 5% of cases. Lungs and bones are the common sites of disease recurrence. Recurrence at other sites is rare. The unusual sites of recurrence reported in English literature are kidney, brain, muscle, subcutaneous tissue, stomach, duodenum, and penis. Site of recurrence has a prognostic significance. Patients with pulmonary recurrence have a better prognosis as compared to those with extrapulmonary involvement.[3,4,5,6]
Fluorine-18 FDG PET/CT has established the role in staging, assessment of treatment response, and restaging of various malignancies. The whole body survey of F-18 FDG PET/CT provides a one-stop shop for evaluation of local disease as well as detecting sites of distant metastases.
In a systematic review on the role of F-18 FDG PET/CT in staging and restaging of OSs, Quartuccio el at suggested that F-18 FDG-PET and PET/CT is superior to bone scintigraphy and conventional imaging methods in detecting bone metastases; while spiral CT is superior to F-18 FDG-PET for detection of pulmonary metastases from OS. They recommended that combination of F18-FDG PET/CT with conventional imaging methods is a valuable tool for staging and restaging of OS.[7]
Though OS are known to recur at local site or involve the lungs and bone, rarely they can also involve unexpected soft tissue sites such as muscle, subcutaneous tissue, anterior abdominal wall, serosal, and pancreatic deposits, respectively, as exemplified by our case. Detection of multiple atypical sites of recurrence of OS on F-18 FDG PET/CT in a single patient after 6 years of disease free interval makes our case unique. This case further emphasizes the potential role of whole body F-18 FDG PET/CT imaging in restaging of OS and provides an impetus to conduct further prospective multicenter trials to validate the role of F-18 FDG PET/CT in restaging of OS.
CONCLUSION
Fluorine-18 FDG PET/CT has a potential role for restaging of OGS. The present case underscores the ability of F-18 FDG PET/CT to detect unusual sites of recurrence.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Arndt CA, Rose PS, Folpe AL, Laack NN. Common musculoskeletal tumors of childhood and adolescence. Mayo Clin Proc. 2012;87:475–87. doi: 10.1016/j.mayocp.2012.01.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol. 2002;20:776–90. doi: 10.1200/JCO.2002.20.3.776. [DOI] [PubMed] [Google Scholar]
- 3.Kempf-Bielack B, Bielack SS, Jürgens H, Branscheid D, Berdel WE, Exner GU, et al. Osteosarcoma relapse after combined modality therapy: An analysis of unselected patients in the Cooperative Osteosarcoma Study Group (COSS) J Clin Oncol. 2005;23:559–68. doi: 10.1200/JCO.2005.04.063. [DOI] [PubMed] [Google Scholar]
- 4.Hawkins DS, Arndt CA. Pattern of disease recurrence and prognostic factors in patients with osteosarcoma treated with contemporary chemotherapy. Cancer. 2003;98:2447–56. doi: 10.1002/cncr.11799. [DOI] [PubMed] [Google Scholar]
- 5.Kim SJ, Choi JA, Lee SH, Choi JY, Hong SH, Chung HW, et al. Imaging findings of extrapulmonary metastases of osteosarcoma. Clin Imaging. 2004;28:291–300. doi: 10.1016/S0899-7071(03)00206-7. [DOI] [PubMed] [Google Scholar]
- 6.Radhakrishnan VS, Balaji J, Lakshminarasimhan S, Karkuzhali P, Vijayasarathy K. Unusual case of extrapulmonary metastatic recurrence in a patient with osteosarcoma. J Clin Oncol. 2011;29:e3–5. doi: 10.1200/JCO.2010.29.9917. [DOI] [PubMed] [Google Scholar]
- 7.Quartuccio N, Treglia G, Salsano M, Mattoli MV, Muoio B, Piccardo A, et al. The role of Fluorine-18-Fluorodeoxyglucose positron emission tomography in staging and restaging of patients with osteosarcoma. Radiol Oncol. 2013;47:97–102. doi: 10.2478/raon-2013-0017. [DOI] [PMC free article] [PubMed] [Google Scholar]