

Abstract
Male breast cancer accounts for 1% of all breast malignancies and 0.1% of all male cancer death. Like Paget's disease, DCIS is a rare form of male breast malignancy. We report a 69-year-male presenting with 3 years history of subtle of nipple symptoms and normal breast imaging. Punch biopsy of nipple established the diagnosis of Paget's disease and subsequent histology of mastectomy specimen revealed underlying DCIS.
INTRODUCTION
In 1974 Sir James Paget described the clinical entity, now known as Paget's disease as an eczematous change in the nipple preceding an underlying mammary carcinoma’. Paget's disease accounts for 1–4% of all breast malignancy, the most of them are associated with underlying invasive breast cancer.
CASE REPORT
We present the case of 69-year-old male, referred to the breast clinic with symptoms of intermittent change of colour and burning sensation of right nipple for 3 years duration. On clinical examination the nipple looked erythematous with eczematous crust formation; examinations of both breasts and axillae were unremarkable. The patient denied family history of breast cancer, there were no obvious risk factors nor any BRCA mutation found in subsequent genetic test but there was an interesting coincidence of his wife having treatment for breast cancer (DCIS) 6 months earlier.
Investigation: bilateral mammogram and ultrasound of right breast were essentially normal. Punch biopsy of right nipple showed Paget's disease with epidermal infiltration by malignant cells that were positive for Cytokeratin 7, oestrogen and progesterone receptors.
Treatment: right mastectomy and sentinel node biopsy were carried out. The patient made uneventful recovery and at first annual follow-up he was disease free and symptom free with unremarkable left surveillance mammogram.
Histology: consistent with non-invasive Paget's disease of the nipplè (Fig. 1), associated with 11 mm focus of underlying high-grade DCIS of solid and micropapillary type (Fig. 2). There was no invasive disease. Sentinel node biopsy was clear.
Figure 1:
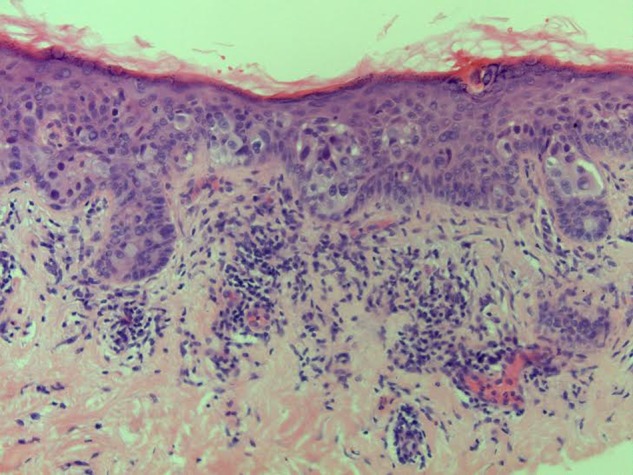
Non-invasive Paget's disease.
Figure 2:
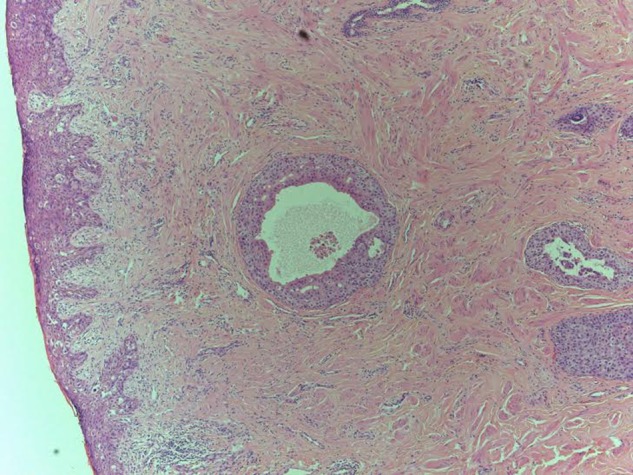
11 mm focus high-grade DCIS solid and micropapillary type.
DISCUSSION
Paget's disease of male breast is extremely rare. Until 1996 only 32 cases were reported world wide [1].
Paget's disease usually occurs in 5th and 6th decade of life [2].The time from first symptom to treatment is 12–14 months. Misdiagnosis as eczema, treatment with topical steroid and coupled with normal imaging are the most common reasons for delay ([1] The case that we are reporting has long history. Interestingly the patient did present to a breast clinic with same symptom 3 years earlier. He was reassured and discharged after normal breast imaging without a biopsy of the nipple.
The pathogenesis of Paget's disease is disputed. The epidermotropic hypothesis proposes that Paget's cells arise from the terminal lobular ductal unit and migrate towards the epidermis, this is supported by the common link between Paget's cells and an underlying breast cancer or DCIS. An alternative hypothesis is the intraepidermal transformation theory where malignant Keratocyte are thought to arise from the areolar epidermis.
The usual presenting features are change in nipple colour with burning sensation, itching, erythema, scale formation and eczematous lesion starting in the nipple and spreading to areola and at later stage ulceration develops with destruction of the nipple and areola.
Pigmented Paget's disease of male breast is rare and only few cases have been reported and should be included in differential diagnosis of any pigmented lesion of the nipple [3, 4]; other conditions included in differential diagnosis are eczema, dermatitis and Bowens disease. Paget's disease usually starts in the nipple and spreads to areolar region while eczema and dermatitis starts in the areola, in the latter there may be presence of similar skin lesions in other parts of the body, responding to topical steroid. Punch biopsy of the nipple with histochemical stains will confirm diagnosis of Paget's disease. Paget's cells stain positive for CK7, CAM-5.2, AE1/AE3 and S100 but do not express HMB-45 and high-molecular-weight keratins, which helps differentiate from melanomas [5, 6].
MRI has much higher sensitivity in diagnosing underlying cancer than mammogram and ultrasound [7, 8].
There is no evidence that Paget's disease behaves differently in males versus females but 5-year survival rate is quite low in males; 20–30% in males versus 30–50% in females [3], this may be because of delay in diagnosis.
The standard treatment of male Paget's disease is mastectomy and sentinel node biopsy, adjuvant therapy and further axillary surgery will be in line with final histology, Sentinel node biopsy and receptors status.
There are three learning points from this case:
Paget's disease may present with subtle signs and symptoms which may not progress significantly for long time.
Breast imaging mammogram and ultrasound may be normal.
It is prudent to undertake punch biopsy of the nipple in a patient, presenting with any nipple issue regardless of breast imaging.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1.Desai DC, Brenan EJ, Carp NZ. Paget's disease of the male breast. Am Surg 1996;62:1068–72. [PubMed] [Google Scholar]
- 2.O'Sullivan ST, McGreal GT. Paget's disease of male breast without underlying breast carcinoma. J Clin Pathol 1994;47:851–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nakamara S, Hashimoto Y, Yokoo H. Pigmented Paget's disease of the male breast; report of a case. Dermatology 2001;202:134–7. [DOI] [PubMed] [Google Scholar]
- 4.Perez A, Sanchez JL, Colon AL. Pigmented mammary Paget's disease in a man. Bol Assoc Med PR 2003;95:36–9. [PubMed] [Google Scholar]
- 5.Smith KJ, Tuur S, Corvellette D. Lupton GP Cytokeratin 7 staining in mammary and extamammary Paget's disease. Mod Pathol 1997;10:1069–74. [PubMed] [Google Scholar]
- 6.Hitchcock A, Topham S, Bell J, Gullick W. Routine diagnosis of mammary Paget's disease. A modern approach. Am J Surg Pathol 1992;16:58–60. [DOI] [PubMed] [Google Scholar]
- 7.Friedman EP, Hall-Craggs MA, Mumtaz H. Breast MR and appearance of the normal and abnormal nipple. Clin Radiol 1997;52:854–61. [DOI] [PubMed] [Google Scholar]
- 8.Moris EA. Breast cancer imaging with MRI. Radiol Clin North Am 2002;40:443–66. [DOI] [PubMed] [Google Scholar]