

Abstract
AIMS:
To compare depression, anxiety, stress, and related factors among women and men with human immunodeficiency virus (HIV) infection.
SETTINGS AND DESIGN:
In this cross-sectional survey conducted between November and September 2013, 200 participants with HIV/acquired immune deficiency syndrome (AIDS) attending Consultation Centers.
MATERIALS AND METHODS:
Participants with HIV/AIDS were interviewed using the Depression, Anxiety and Stress Scales questionnaire (DASS21 ).
RESULTS:
There were significant associations between marital status of women and the level of depression (P < 0.05). However, the mean depression and anxiety in women are greater than men (P < 0.05), and the mean stress in men is greater than women (P < 0.05).
CONCLUSIONS:
HIV infection is related with psychiatric disorders. According to the results, women are more vulnerable to depression and anxiety and they need more care. Management of these psychiatric disorders is very important and requires innovative comprehensive approaches.
KEY WORDS: AIDS, Anxiety, depression, HIV, stress
INTRODUCTION
Human immunodeficiency virus (HIV) infection and acquired immune deficiency syndrome (AIDS) is a global epidemic that has been reported from all countries. Worldwide, the rate of infected adults is approximately thirty-seven million, 50% of which are women. It is estimated that two million and five hundred thousand children under the age of 15 are living with HIV or AIDS.[1] Although compared with many other countries, this infection arrived late in Iran, it now has an expanding growth rate throughout the population and an estimated 24,050 patients suffered from HIV infection, of which 92% are men and 8% are women.[2] The age of the infected patients is about 25 to 34 and nearly 70% of transmission cases are injection drugs users (IDUs), and the rest of them are affected by sexual intercourse, blood products, and mother-to-child transmission.[3] Also in Iran, about 69.8% of infected persons are addicted to drugs.[4]
Negative thinking and stigma in society against AIDS lead to many social issues, like physical and mental health problems in affected patients, leading to many difficulties in their useful activities and interests. Infected individuals are so vulnerable to many changes in their whole lives including reduction in self-confidence and self-esteem, decrease in daily functions and social activities, increase in sense of vulnerability, disorganized thinking, and also physical symptoms. Moreover, frequent visits to the doctor, the high cost of drugs, and also the side effects of drugs lead to the reduction of quality of life.[5]
Depression is the most common secondary complication related to HIV, AIDS and the most common psychiatric disorder in these individuals. The prevalence of depression among HIV-positive patients is about 57% and it has been reported more than 5 times of the general population. HIV-positive individuals with depression may have more painful experiences without any symptoms or physical signs.[6] Long-term studies on HIV population show significant correlations between general health, physical and work performance, and psychiatric disorders like depression, anxiety, and stress.[7]
People with HIV infection have many psychological problems, and the most common of these are depression and anxiety. These difficulties are rooted in stigma and discrimination in society. Many of those infected are ostracized and forced to become isolated. Much research in this area suggests that the labeling and stigma is associated with depression and low self-esteem. Due to stigma and discrimination, people with high-risk behaviors are reluctant to do any voluntary HIV test.[5]
Stress is the physiological response to a stressor, when the body reacts to a challenge. Stress typically describes a negative condition or a positive condition that can have an impact on the person's mental and physical well-being. Long-term or chronic stress weakens the immune system and leads to disease susceptibility and makes the body prone to depression.[8] People who suffer from a chronic disease such as HIV infection or cancer have a various range of psychiatric disorders. The risk of psychiatric disorders in individuals with HIV is 7–37% more than the normal population. Dropping out from school, unemployment, addiction to drugs and substances, stigma, and social harms are the most important risk factors in people with HIV infection for becoming depressed.[5]
The most common psychiatric disorder in AIDS patients is depression. Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feeling, and sense of well-being. Depressed people can feel sad, anxious, empty, hopeless, worried, helpless, and worthless.[9] Moreover, depression can affect physical ability and performance. Probability of depression increases since the HIV test becomes positive. Depression is associated with many symptoms including feelings of sadness, loss of interest or pleasure, sleep and appetite disturbance, lack of sexual drive, impaired attention, memory, and concentration. Mortality in depressed women is higher compared with non-depressed patients.[10]
Anxiety is an unpleasant feeling of fear, worry, and uneasiness that is often accompanied by restlessness, fatigue, problem in concentration, muscular tension, sweating, and palpitation.[11] Like depression, anxiety is a common psychiatric disorder observed in people living with HIV.[12]
Depression and anxiety may have an effect on HIV/AIDS progression, but demographic variables and CD4 cell count and immune response can also have an important role in disease progress.[13] It seems that depression plays a role in reducing the number of CD4 cells.[14] Studies disclosed that stress reduction has a beneficial impact on the clinical course of the disease.
Stigma in HIV-positive women reported much greater, and more women are at risk of depression.[5] Addicted women living with HIV have a low quality of life and suffer from mental disorders which can be correlated with poverty.[15,16] Demographic variables, drug use, social roles, and social support have important proportions for predicting the risk of detection of depression, anxiety, and stress.[17] Mortality rate in women with HIV/AIDS who suffer from chronic depression is much more than those who have less or no depression signs.[18] Stressors such as receiving a positive test result and doubt for beginning of treatment and multiple testing increases the risk of mental disorders. Due to the increased prevalence of HIV/AIDS in the country and the importance of mental health in these patients, researcher want to survey the comparison of the depression, anxiety, and stress and related factors, among women and men with HIV infection.
MATERIALS AND METHODS
This cross-sectional survey was carried out with 200 women and men referred to behavioral diseases consultation centers, between November and September 2013. The women and men were interviewed using the Depression, Anxiety, and Stress Scales questionnaire (DASS 21). This questionnaire was translated into Farsi by skillful translators and researchers are confident that its concepts were not lost in translation. We also used demographic questionnaires that contained the gender, age, educational level, marital status, numbers of children, and the way of infection. Moreover, all subjects were told that they could stop the interview at any time during the study. The data were analyzed using Statistical Package of Social Sciences (SPSS) software, version 20 (SPSS, Chicago, IL, USA). The characteristics of the participants are presented as mean ± standard deviation (SD) or number and percentage. All outcomes were compared using the variance test. Differences between variables were determined using a t test and chi square test. The significance level was set as P < 0.05.
RESULTS
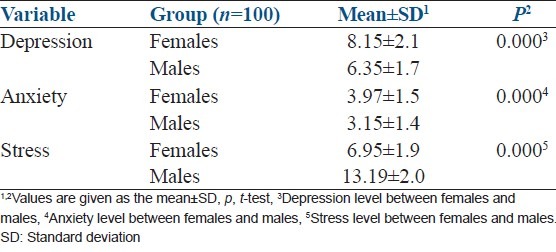
According to the study, 200 volunteers participated in this study of which 100 individuals were females and the rest were males. Their characteristics and sociodemographic are listed in Tables 1 and 2. The comparisons show that there are not significant differences between demographic characteristics and the way of infection with HIV/AIDS in participants [Table 1]. There were significant associations between marital status of women and the level of depression (P < 0.05). However, there were no correlation between marital status, age, and educational level and anxiety and stress in women participants. It seems that the mean level of depression is higher in the unmarried, widowed, and divorced women (P < 0.05). There were no significant association between marital status, age, education and depression, anxiety, and stress in men participants (P > 0.05) [Table 2]. However, the mean depression and anxiety in women are greater than men (P < 0.05), and the mean stress in men is greater than women (P < 0.05) with 95% confidence interval [Table 3].
Table 1.
Characteristics of the infected women and men1
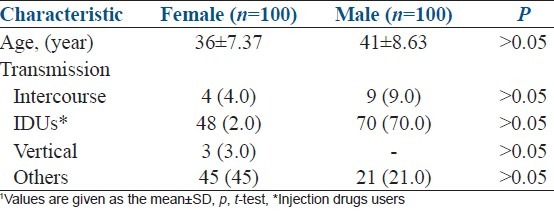
Table 2.
Sociodemographic data concerning the infected women and men1
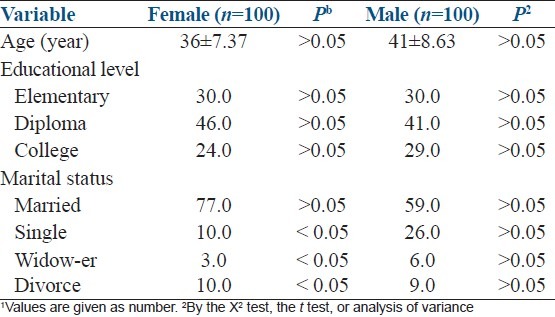
Table 3.
Comparison depression, anxiety, and stress among females and males
DISCUSSION
This cross-sectional study was conducted to investigate the comparison of the depression, anxiety, and stress and related factors, among women and men with HIV infection. The results reveal that the level of depression and anxiety are significantly greater in women than men, the level of stress is higher in men than women and this condition has correlation with other factors including marital status. It seems that the level of depression is higher in the unmarried, widowed, and divorced women (P < 0.05). However, there were no correlation between marital status, age, and educational level and anxiety and stress in women participants. It seems that the mean level of depression is higher in the unmarried, widowed, and divorced women (P < 0.05). There were no significant association between marital status, age, education and depression, anxiety, and stress in men participants (P > 0.05). Unmarried women are the most vulnerable group for the health difficulties. It seems that the strongest variable for the psychic disorder is marital status. Marriage itself does not prevent social and economical problems; however, it can act as a barrier against to external stimuli that produce stress. Husband's support is a very effective defense against stress.[5] The data reveal that three participants in women group had been infected from their HIV-positive mothers in the prenatal period. It is important to focus on the infected women for the management of some strategies including family planning, childbearing, prenatal, and postnatal care. These results show that living with HIV/AIDS can be stressful[17] and the psychosomatic symptoms like depression and anxiety are seen in these groups. Moreover, depression, anxiety, and stress can have an effect on the progression of the disease and reduce the effect of the drugs that are used for the infection.[19] Changes in health status like common cold or unexplained pain for individuals with HIV/AIDS were imagined to be an indication of an exacerbation of HIV/AIDS and hence escalated to depression.[20] Several studies have reported that the rate of depression, anxiety, and stress is seen more frequently in people with HIV/AIDS.[20] Morrison et al. reported that depressive disorder and more symptoms of depression and anxiety are higher in HIV-seropositive women than HIV-seronegative women with similar demographic characteristics.[12] We report the same and also a significant relationship among depression, anxiety, and stress and the infected persons. For most participants, the depression was worsened by stigma and labeling of disclosure, they were worried about the stigma related to HIV, with a sex worker or an injection drug user. Also, they were concerned about being rejected by their family. In addition, behavioral factors like substance abuse and risky sex can play a role in psycho-immune relationships.[19] Connecting HIV and sexual health precautions and reproduction is widespread method to provide people with economical approaches to prevention, treatment, care, and support. It seems that resorting to human rights statement and the constitution, society must consider HIV a social phenomenon, regard the infected as patients, and finally take a humanitarian stance to find a solution for this problem. Due to the rise in the number of infected women and men in the world, and also women's need for dominant care in all societies and their vulnerability to depression, it is particularly important to manage these psychosomatic disorders. HIV infection is related with psychiatric disorders. It seems that, women are more vulnerable to depression and anxiety and they need more care. Management of these psychiatric disorders is very important and requires innovative comprehensive approaches.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.UNAIDS. UNAIDS report on the global AIDS epidemic. [Last accessed on 2015 Jan 09]. Available from: http://ww.w.unaids.org/globalrepor/documents/20101123_GlobalReport_full_en.pdf .
- 2.Annual Report of HIV in Iran. [Last accessed on 2015 Jan 09]. Available from: http://www.behdasht.gov.ir .
- 3.Anthony S, Fauci H, Clifford L. Human immunodeficiency virus disease AIDS and related disorders. In: Frederick P, editor. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw Hill Book Company; 2012. pp. 1506–87. [Google Scholar]
- 4.Razani N, Mohraz M, Kheirandish P, Malekinejad M, Malekafzali H, Mokri A, et al. HIV risk behavior among injection drug users in Tehran, Iran. Addiction. 2007;102:1472–82. doi: 10.1111/j.1360-0443.2007.01914.x. [DOI] [PubMed] [Google Scholar]
- 5.Stall R, Mills CT, Williams J, Hart T, Greenwood G, Paul J, et al. Association of Co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. Am J Public Health. 2003;93:939–42. doi: 10.2105/ajph.93.6.939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Valente SM. Depression and HIV Disease. J Assoc Nurses AIDS Care. 2003;14:41–51. doi: 10.1177/1055329002250993. [DOI] [PubMed] [Google Scholar]
- 7.Orland M, Tucker JS, Sherbourne CD, Burnam MA. A cross-lagged model of psychiatric problem and health-related quality of life among a national sample of HIV-positive adults. Med Care. 2005;43:21–7. [PubMed] [Google Scholar]
- 8.Katibaei J. Comparison of quality of life, stress and mental health of addicts and non-addicteds affected by HIV and healthy individuals. JBS. 2010;4:135–9. [Google Scholar]
- 9.Tremblay PF, King PR. State and trait anxiety coping styles and depression among psychiatric inpatients. JBS. 1994;26:505–19. [Google Scholar]
- 10.Olagunju AT, Adeyemi JD, Ogbolu RE, Campbell EA. A study on epidemiological profile of anxiety disorder among people living with HIV/AIDS in sub-Saharan Africa HIV clinic. AIDS Behav. 2012;16:2192–7. doi: 10.1007/s10461-012-0250-x. [DOI] [PubMed] [Google Scholar]
- 11.Thoits PA. Social support as coping assistance. J Consult Clin Psychol. 1986;54:419–23. doi: 10.1037//0022-006x.54.4.416. [DOI] [PubMed] [Google Scholar]
- 12.Morrison MF, Petitto JM, Ten Have T, Gettes DR, Chiappini MS, Weber AL, et al. Depressive and anxiety disorders in women with HIV infection. Am J Psychiatry. 2002;159:789–96. doi: 10.1176/appi.ajp.159.5.789. [DOI] [PubMed] [Google Scholar]
- 13.Bouhnik AD, Preau M, Vincent E, Carrieri MP, Gallais H, Lepeu G, et al. Depression and clinical progression in HIV-infected drug users treated with highly active antiretroviral therapy. Antivir Ther. 2005;10:53–61. [PubMed] [Google Scholar]
- 14.Ickovics JR, Milan S, Boland R, Schoebaum E, Schuman P, Vlahov D. Psychological resources protect health: 5-year survival and immune function among HIV-infected women from four US cities. AIDS. 2006;20:1851–60. doi: 10.1097/01.aids.0000244204.95758.15. [DOI] [PubMed] [Google Scholar]
- 15.World Health Organization. Joint United Nations Program on HIV/AIDS. Geneva, Switzerland: WHO; 2002. [Google Scholar]
- 16.UNAIDS Website. [Last accessed on 2015 Jan 09]. Available from: http://www.UNAIDS.org/2012 .
- 17.Khalatbari J, Bazarganiyan N. Comparison the depression, anxiety and stress in intravenous drug abusers, with and without HIV/AIDS. J Gilan Univ Med Sci. 2010;78:76–83. [Google Scholar]
- 18.Cook JA, Grey D, Burke J, Cohen MH, Gurman AC, Richardson JL, et al. Depressive symptoms and AIDS related mortality among a multisite cohort of HIV-positive women. Am J Public Health. 2004;94:1133–40. doi: 10.2105/ajph.94.7.1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Leserman J. Role of depression, stress, and trauma in HIV disease progression. Psychosom Med. 2008;70:539–45. doi: 10.1097/PSY.0b013e3181777a5f. [DOI] [PubMed] [Google Scholar]
- 20.Komiti A, Judd F, Grech P, Mijch A, Hoy J, Williams B, et al. Depression in people living with HIV/AIDS attending primary care and outpatient clinics. Aust New Zealand J Psychiatr. 2003;37:70–7. doi: 10.1046/j.1440-1614.2003.01118.x. [DOI] [PubMed] [Google Scholar]