

Abstract
Background:
Chronic obstructive pulmonary disease (COPD) and diabetes mellitus (DM) are common and under diagnosed medical conditions in India. Prevalence of these chronic diseases are high both in rural and urban areas. However, exact prevalence of DM in Indian COPD patients in unclear. Co-morbid conditions like DM have great impact on the outcome of COPD in the form of severity, exacerbations, morbidity and mortality. Hence the present study objective was to screen COPD patients for DM.
Results:
A total of 1662 patients with COPD (Males = 1264, Female = 398) with mean age 58 ± 9.6 were screened for DM. Patients with known history of DM were 353 (21.24%) and were enrolled as Known DM cases. Remaining 1309 (78.76%) patients whose DM status was unclear were screened by random blood sugar (RBS). One-hundred and seventy-one subjects had RBS > 110 mg/dl. About 73 (4.39%) subjects had fasting blood sugar (FBS) > 126 mg/dl. They were considered as Newly Diagnosed DM cases. Total number of DM cases in the study including new and known was 426 (25.63%). Number of patients with deranged FBS (FBS between 110 mg/dl to126 mg/dl) was 84 (5.05%). Among the DM patients with COPD 168 (10.11%) had poor glycemic control with HbA1c > 8. Prevalence of DM in present study was 25.63%.
Conclusion:
Prevalence of DM in COPD patients in the present study is 25.63% when actively screened in tertiary care hospital. It is feasible and imperative to screen all COPD patients for DM in all health care facilities routinely.
Keywords: COPD, diabetes mellitus, prevalence, screening
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) and diabetes mellitus (DM) are common and under diagnosed medical conditions in India. COPD is a progressive, partially reversible airflow obstructive condition and is a growing public health problem globally. In its advanced stage, the disease causes severe disabilities and poor quality of life.1,2,3,4 It was predicted that COPD will be the third leading cause of death worldwide by 2020 with Asian countries having three times the number of patients than the rest of the world.5,6,7 If the mortality from co-morbid conditions like DM associated with COPD is taken into account, then this disease poses an even greater impact on health outcomes.
COPD may be considered as a novel risk factor for new onset type 2 DM (T2DM) via multiple pathophysiological alterations such as inflammation, oxidative stress, insulin resistance, weight gain and alterations in metabolism of adipokines.8 The risk appears to exist regardless of the severity of COPD. T2DM is particularly common medical disorder and a leading cause of morbidity and mortality worldwide. Disturbances in glucose metabolism are more frequent in COPD patients than in non COPD individuals. Similarly, almost half of all COPD patients suffer from other medical problems frequently linked to diabetes, such as elevated blood pressure and higher levels of cholesterol. The combination of these medical problems is sometimes referred to as "metabolic syndrome" and is considered a cause for various cardiovascular complications in COPD patients.9 Similarly, many studies have found that DM causes an accelerated decline in lung functions as compared to non-diabetics. Additionally, uncontrolled diabetes is linked to worsen the outcomes (longer hospital stay and risk of death) in people that suffer from an exacerbation of COPD.8
The prevalence of COPD in India according to various studies is 3.67% (4.46% among males and 2.86% in females). The estimated burden of COPD in India is about 15 million cases (males and females contributing to 9.02 and 5.75 million, respectively). These figures may however underestimate the true burden since questionnaire based prevalence rates tend to underestimate the true spirometry-based prevalence of COPD.10 There is also an accelerated epidemic of DM in India in last 50-60 years with national adult prevalence of 8.3%.11 In terms of absolute numbers and given the size of population, India is the country, burdened with highest number of COPD and DM cases. However, exact prevalence of DM in COPD patients in Indian population is unclear. Hence the present study objective was to screen COPD patients for DM.
MATERIALS AND METHODS
This was a cross sectional study of patients diagnosed with COPD as per Global Initiative for chronic obstructive lung disease (GOLD) criteria 2013, carried out at the Inpatient and outpatient departments of Pulmonary medicine, Internal Medicine and Endocrinology sections at a tertiary care hospital, Belgaum, Karnataka, India, from Jan 2013 to April 2014.
A total of 1662 COPD patients, aged less than 40 years, attending inpatient and outpatient departments of Pulmonary Medicine, Internal Medicine and Endocrinology sections at a tertiary care hospital were enrolled for the study after meeting the inclusion criteria. Patient were excluded from the study if they had pulmonary conditions other than COPD (e.g. TB, HIV infection), connective tissue disorders, chronic renal failure, chronic liver disease, malignancies on long term steroid or cytotoxic drug therapy, chronic alcoholics. The information of the same was obtained from detailed history, clinical examination, chest radiography and medications used by the patient currently or previously. Informed consent was obtained from all study participants for investigations needed and purpose of the study.
Baseline data was recorded which included level of education, age, sex, years of exposure to cigarette/bidi smoking and biomass fuel, BMI and respiratory symptoms including previous spirometry reports. All subjects underwent spirometry testing for airflow limitation and were classified as mild, moderate, severe and very severe accordingly as per GOLD guidelines.1 The screening and diagnosis of DM followed national guidelines, which stipulated that a fasting blood glucose (FBG) is used with cut-off thresholds in line with those recommended by WHO. In brief, FBG >126 mg/dl indicates DM; FBG from 110 mg/dl to <126 mg/dl indicates impaired fasting glucose; FBG <110 mg/dl is normal.12 The patients already known to have DM were directly enrolled in the study as "Known DM" cases with COPD. Patients whose diabetes status was unclear underwent random blood sugar (RBS) testing, and if was more than 126 mg/dl, the subjects were further evaluated with fasting blood sugar (FBS) and post prandial blood sugar (PPBS). If FBS was more than 126 mg/dl or PPBS more than 200 mg/dl the subjects were confirmed as having DM after which they were classified as new DM cases with COPD. All the participants underwent glycosylated haemoglobin (HbA1c) evaluation.
RESULTS
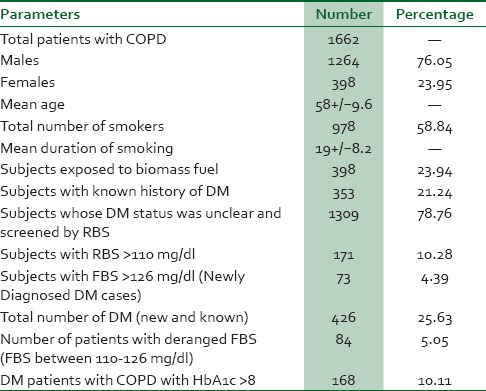
A total of 1662 patients with COPD (Males = 1264, Female = 398) with mean age 58 ± 9.6 were screened for DM. Total number of smokers in the study were 978 and patients with history of exposure to biomass fuel were 398. Patients with known history of DM were 353 (21.24%) and were enrolled as "Known DM" cases. Remaining 1309 (78.76%) patients whose DM status was unclear were screened by RBS. Subjects with RBS > 110 mg/dl were 171. They were further evaluated for FBS. About 73 (4.39%) subjects had FBS >126 mg/dl. They were considered as "Newly Diagnosed DM" cases. Total number of DM cases in the study including new and known was 426 (25.63%). Number of patients with deranged FBS (FBS between 110-126 mg/dl) was 84 (5.05%). Among the DM patients with COPD 168 (10.11%) had poor glycaemic control with HbA1c >8 [Table 1].
Table 1.
Parameters and percentage values
DISCUSSION
All studies conducted agree in predicting that both the morbidity and mortality burden of COPD is rising. By 2020, COPD is projected to cause over 6 million deaths annually worldwide, thus becoming the third leading cause of death in the world.1 The general ageing of the world's population is reinforcing this trend, partly due to the fact that the prevalence is higher in age-groups. Our general understanding of the disease has greatly improved over the past 10 years. Epidemiological studies and large clinical trials have helped us to understand the importance of comorbidities.13,14 Greater understanding of the pathophysiology of COPD, focused on the concept of systemic inflammation, has also helped to explain the high frequency of major co morbidities (cardiovascular, skeletal and metabolic conditions like DM) in addition to coexisting conditions that one would naturally expect due to the patients’ advanced age and due to shared risk factors.
The present study is first of its kind, in which COPD patients are actively screened for DM in a tertiary care hospital in India. The prevalence of DM in our study was 25.63% which is in line with various studies reported from other countries. The prevalence of DM in COPD patients varies between different studies. 10.3% in a population of grade 2/3 COPD patients in a rehabilitation centre according to Crisafulli et al.,14 12.6-14.5% in an all-stage COPD population according to Mannino et al.,15 12.2% with an increased risk in active smokers according to Feary et al.16 However the high prevalence of DM in the current study could be due to the fact that most of the patients age was more than 50 years with history of smoking or exposure to biomass fuel for more than 10 years. Average duration of smoking in the study population was 19 ± 8.2. Most of these were bidi smokers containing raw unfiltered tobacco.
Systemic inflammation [with elevated markers such as C-reactive protein (CRP), tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6)] plays an important role in both, the progression of COPD and the development of insulin resistance. Smoking is one cause of inflammation.16,17 Smokers have a two-fold higher risk of developing DM than nonsmokers. A recent review of the literature established the complex link between smoking and obesity in the development of co-morbidities, involving an enzyme cascade that originates in adipose tissue considered a site for production of cytokines (TNF-a, IL-6, etc), while adiponectin decreases with increased adiposity. This increases insulin resistance, circulating free radicals and oxidative stress, exacerbating the initial pulmonary inflammation. Adipose tissue stimulation is promoted by tissue hypoxia, smoking and the degree of bronchial obstruction.18,19,20,21
Severity of systemic inflammation is a direct measure of severity of COPD. In our study more than two-third of the subjects had moderate to severe COPD who had DM, which is in agreement with many cohort studies which have demonstrated that moderate to severe COPD increases the risk of DM (OR 1.4 and 1.5, respectively).15 In a large cohort of females, Song et al.,22 showed that the presence of asthma or COPD was associated with risk of developing T2DM, suggesting that airway inflammation contributes to the pathophysiology of diabetes. Conversely, in a US cohort, the relative risk of developing COPD was higher (HR 1.22) in patients with diabetes than in non-diabetics.23 It is well known fact that DM significantly affects the outcome of COPD including time to first hospitalisation and 5-years mortality rates.15 According to the Emerging Risk Factors Collaboration, the HR for COPD-related death was 1.27 as compared to subjects without diabetes.24 Another study showed that an increase in blood glucose of 1 mmol/L increases the risk of death by 15%.25 Parrapil et al. and Baker et al., confirmed an increased risk of death (OR 1.93) and hospital stays were 10.3% longer for patients with diabetes hospitalized for COPD exacerbation.26,27
An important observation in the present study was that about 4.39% of COPD patients were newly diagnosed as having DM. This is very significant finding as large number of COPD patients in our country are usually not screened for DM. Also significant number of patients with COPD in our country receive high dose of inhaled corticosteroids for severe cases and systemic corticosteroids during exacerbations.
The present study is exceptional as it could detect as many as 5% of COPD patients who did not have DM but had deranged FBS (110-126 mg/dl). This could add to the pool of high risk patients developing DM in future when exposed to the stress of COPD and exacerbations. Among the known and new DM patients, 39.43% of patients in our study had poor DM control with HbA1c more than 8.
India with population more than 1.27 billion has the highest number of both COPD and DM patients. In total two-third Indian population reside in rural areas and smaller towns where facilities for diagnosis of COPD are inadequate. In the past 50-60 years there has been significant change in the life style, food habits, decreased physical activity and obesity in Indian population. Consequences of which, there has been escalating epidemic of DM in both rural and urban populations. It is also worth noting that uncontrolled and undiagnosed DM in COPD patients have greater impact on the outcome of COPD in the form of severity, quality of life, exacerbations, hospital stay, health care costs and death. Screening for active DM in COPD should lead to earlier detection of DM and prompt treatment of COPD and good control of DM as well.
The strengths of the present study are that we implemented the screening within the routine system with no special budget ., allocated to support these activities. We think that because of their higher risk of DM and the fact that patients with COPD are anyway more likely to attend health facilities, the marginal costs for DM screening using a symptom-base approach with blood glucose testing are likely to be small and proved cost effective. Hence active screening of COPD patients for DM is feasible and imperative in routine health care settings. The limitation of the study is a single centre screening and further studies are suggested on larger geographical areas.
CONCLUSION
Prevalence of DM in COPD patients in present study is 25.63% when actively screened in tertiary care hospital. It is feasible and imperative to screen all COPD patients for DM in all health care facilities routinely.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. [Last accessed on 2013 Feb 15]. Available from: www.goldcopd.org .
- 2.Rennard S, Decramer M, Calverley PM, Pride NB, Soriano JB, Vermeire PA, et al. Impact of COPD in North America and Europe in 2000: Subjects’ perspective of Confronting COPD International Survey. Eur Respir J. 2002;20:799–805. doi: 10.1183/09031936.02.03242002. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. Chronic respiratory diseases. COPD: Definition. 2013. [Last accessed on 2013 Jun 15]. Available from: http://www.who.int/respiratory/copd/en/
- 4.Antwi S, Steck SE, Heidari K. Association between prevalence of chronic obstructive pulmonary disease and health-related quality of life, South Carolina, 2011. Prev Chronic Dis. 2013;10:E215. doi: 10.5888/pcd10.130192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tan WC, Ng TP. COPD in Asia: Where east meets west. Chest. 2008;133:517–27. doi: 10.1378/chest.07-1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet. 1997;349:1498–504. doi: 10.1016/S0140-6736(96)07492-2. [DOI] [PubMed] [Google Scholar]
- 7.Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: Systematic review and metaanalysis. Eur Respir J. 2006;28:523–32. doi: 10.1183/09031936.06.00124605. [DOI] [PubMed] [Google Scholar]
- 8.Rimm EB, Manson JE, Stampfer MJ, Colditz GA, Willett WC, Rosner B, et al. Cigarette smoking and the risk of diabetes in women. Am J Public Health. 1993;83:211–4. doi: 10.2105/ajph.83.2.211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cavaillès A, Brinchault-Rabin G, Dixmier A, Goupil F, Gut-Gobert C, Marchand-Adam S, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22:454–75. doi: 10.1183/09059180.00008612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mirrakhimov AE. Chronic obstructive pulmonary disease and glucose metabolism: A bitter sweet symphony. Cardiovasc Diabetol. 2012;11:132. doi: 10.1186/1475-2840-11-132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gupta D, Agarwal R, Aggarwal AN, Maturu VN, Dhooria S, Prasad KT, et al. Jindal for the COPD Guidelines Working Group. Guidelines for diagnosis and management of chronic obstructive pulmonary disease: Joint ICS/NCCP (I) recommendations. Lung India. 2013;30:228–67. doi: 10.4103/0970-2113.116248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jali MV, Mahishale VK, Hiremath MB. Bidirectional screening of tuberculosis patients for diabetes mellitus and diabetes patients for tuberculosis. Diabetes Metab J. 2013;37:291–5. doi: 10.4093/dmj.2013.37.4.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Directorate General of Health Services, India. National programme for prevention and control of cancer, diabetes, cardiovascular disease and stroke (NPCDCS) [Last accessed on 2013 Mar 10]. Available from: http://health.bih.nic.in/Docs/Guidelines-NPCDCS.pdf .
- 14.Crisafulli E, Costi S, Luppi F, Cirelli G, Cilione C, Coletti O, et al. Role of comorbidities in a cohort of patients with COPD undergoing pulmonary rehabilitation. Thorax. 2008;63:487–92. doi: 10.1136/thx.2007.086371. [DOI] [PubMed] [Google Scholar]
- 15.Celli BR, Thomas NE, Anderson JA, Ferguson GT, Jenkins CR, Jones PW, et al. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: Results from the TORCH study. Am J Respir Crit Care Med. 2008;178:332–8. doi: 10.1164/rccm.200712-1869OC. [DOI] [PubMed] [Google Scholar]
- 16.Mannino DM, Thorn D, Swensen A, Hulguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962–9. doi: 10.1183/09031936.00012408. [DOI] [PubMed] [Google Scholar]
- 17.Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: A comprehensive analysis using data from primary care. Thorax. 2010;65:956–62. doi: 10.1136/thx.2009.128082. [DOI] [PubMed] [Google Scholar]
- 18.Manson JE, Ajani UA, Liu S, Nathan DM, Hennekens CH. A prospective study of cigarette smoking and the incidence of diabetes mellitus among US male physicians. Am J Med. 2000;109:538–42. doi: 10.1016/s0002-9343(00)00568-4. [DOI] [PubMed] [Google Scholar]
- 19.Shoelson SE, Lee J, Goldfine AB. Inflammation and insulin resistance. J Clin Invest. 2006;116:1793–801. doi: 10.1172/JCI29069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pradhan A. Obesity, metabolic syndrome, and type 2 diabetes: Inflammatory basis of glucose metabolic disorders. Nutr Rev. 2007;65:S152–6. doi: 10.1111/j.1753-4887.2007.tb00354.x. [DOI] [PubMed] [Google Scholar]
- 21.Fabbri LM, Luppi F, Beghé B, Rabe KF. Complex chronic comorbidities of COPD. Eur Respir J. 2008;31:204–12. doi: 10.1183/09031936.00114307. [DOI] [PubMed] [Google Scholar]
- 22.Tkacova R. Systemic inflammation in chronic obstructive pulmonary disease: May adipose tissue play a role. Review of the literature and future perspectives? Mediators Inflamm. 2010;2010:585989. doi: 10.1155/2010/585989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Song Y, Klevak A, Manson JE, Buring JE, Liu S. Asthma, chronic obstructive pulmonary disease, and type 2 diabetes in the Women's Health Study. Diabetes Res Clin Pract. 2010;90:365–71. doi: 10.1016/j.diabres.2010.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ehrlich SF, Quesenberry CP, Jr, Van Den Eeden SK, Shan J, Ferrara A. Patients diagnosed with diabetes are at increased risk for asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and pneumonia but not lung cancer. Diabetes Care. 2010;33:55–60. doi: 10.2337/dc09-0880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Emerging Risk Factors Collaboration. Seshasai SR, Kaptoge S, Thompson A, Angelantonio E, Gao P, Sarwar N, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364:829–41. doi: 10.1056/NEJMoa1008862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Baker EH, Janaway CH, Philips BJ, Brennan AL, Baines DL, Wood DM, et al. Hyperglycemia is associated with poor outcomes in patients admitted to hospital with acute exacerbations of chronic obstructive pulmonary disease. Thorax. 2006;61:284–9. doi: 10.1136/thx.2005.051029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Parappil A, Depczynski B, Collett P, Marks GB. Effect of comorbid diabetes on length of stay and risk of death in patients admitted with acute exacerbations of COPD. Respirology. 2010;15:918–22. doi: 10.1111/j.1440-1843.2010.01781.x. [DOI] [PubMed] [Google Scholar]