

Abstract
Background:
Ebola viral fever, a highly contagious haemorrhagic disease has today become a major public health concern in the developing countries worldwide.
Aim:
The purpose of this study was to assess knowledge among dental practitioners regarding Ebola Haemorrhagic Fever (Ebola HF) in Tricity, (Chandigarh, Panchkula and Mohali).
Materials and Methods:
A total of 500 private dental practitioners were randomly approached to participate in this cross-sectional survey. A self-structured, closed ended questionnaire was administered to each participant to record demographic and professional characteristics followed by their knowledge regarding Ebola HF. Knowledge section included questions related to communicability; symptomatology and diagnostics; at-risk individuals; prevention and treatment; and, virus characteristics of Ebola HF.
Results:
The results were expressed in percentages. Multivariable linear regression analysis was carried out to assess the association of participants's demographic and professional characteristics with the knowledge scores. Statistically significant difference was seen when mean knowledge scores were compared based on the locality and qualification of the participants (P < 0.05).
Conclusion:
Dental practitioners from urban areas with higher qualification had better knowledge yet there were notable deficiencies regarding the virus characteristics, diagnostics, elimination and treatment.
Keywords: Ebola virus disease, Ebola HF, infectious disease, knowledge, prevention
INTRODUCTION
The Ebola Haemorrhagic Fever (Ebola HF) also known as Ebola virus disease (EVD), is an acute viral haemorrhagic illness caused by Filoviridae family.1 Ebola viral fever, a highly contagious haemorrhagic disease has today become a major public health concern in the developing countries worldwide. Since 1976, there have been 885,343 suspected and laboratory confirmed cases of Ebola HF in West Africa. This part of the world is persistently confronted with this fatal disease which has an incubation period of 2-21 days (average 3-13days).2 Symptoms range from, firstly, fever and fatigue before descending into headaches, vomiting, violent diarrhoea, then multiple organ failure and massive internal bleeding.3 Ebola typically begins in remote places and can be distributed via hospitals/health care centers or within the community as it takes several infections before the disease is ascertained. The prevalence, morbidity and case fatality of chronological Ebola HF outbreaks showed the persistent resurgence in different regions in Sub-Saharan Africa.2 Ebola HF outbreaks have a case fatality rate of 50-90%, yet no specific drug or vaccine is available for people and/or animals hosts.4 As of September 6 2014, the cumulative number of cases attributed to Ebola HF in the five West African countries stands at 4293.5 New cases are still occurring as there is no standard treatment for Ebola HF.6 First time in the history of world a disease has been so dreaded that it has threatened the existence of any nation, as told by Liberian defense minister to the United Nations Security Council in Liberia where, more than 1000 person have died of Ebola HF including more than 80 health workers.7
Health care workers are at a greater risk of contacting such diseases and may also promote their transmission by occupational exposures.8 Transmission in health care settings has been associated frequently with Ebola HF outbreaks in Africa. If cases of the disease do appear, care must be taken to avoid the spread of the disease within health-care facilities. Patients must be isolated from contact with any unprotected people and hospital workers must wear protective clothing, such as masks, gloves, gowns and goggles.9
Being a highly contagious disease Ebola HF can spread to other parts of the world because of continuous movement of people in different parts of the world so it becomes necessary for the clinicians who come in contact with patients to be, aware of this highly fatal disease.
India being a developing country with high population density and various lifestyle among the folks make India prone towards any type of epidemics so also to Ebola HF. The practice of dentistry exposes dentists to a variety of microorganisms that are transmittable via blood, oral or respiratory secretions.10 Hence, dentists should have sound knowledge on the prevalent infectious diseases, their symptoms, modes of spread and methods of prevention. The purpose of this study was to assess the knowledge of dental practitioners towards Ebola HF in Tricity, India.
MATERIALS AND METHODS
This cross-sectional survey was conducted in the months of July and August 2014 in Tricity. The study protocol was approved by the institutional ethical and review committee of Swami Devi Dyal Hospital and Dental College (dated: 2014, June 2). List of private dental practitioners was obtained from the respective Indian Dental Association branches across Chandigarh, Panchkula and Mohali. From the list, a total of 500 private dental practitioners were randomly approached to participate in the survey. A written informed consent was obtained after explaining about the aims and the objectives of the study. A self-structured, closed ended questionnaire was administered to each participant in person, which took approximately 5 minutes to complete both sections. Survey reports were kept anonymous and participants’ confidentiality was assured.
The original version of the questionnaire was pilot tested in order to determine the test-retest reliability of the survey questions, fifteen private dental practitioners who completed the survey during the initial administration, completed the survey two weeks later. The respondents were also asked for feedback on clarity of the questions and whether there were difficulty in answering the question or ambiguity as to what sort of answer was required. The subjects who participated in the pilot study were not included in the final sample. Chronbach's alpha of the questionnaire was found to be acceptable (0.84). Few modifications were done to improve the understanding of the questionnaire based on the responses.
Final questionnaire consisted of two parts: Section-A, consisted of questions assessing demographic and professional characteristics like age, gender, location, qualification and years of clinical practice while Section-B included questions about knowledge of Ebola HF. Knowledge section (17 questions) included questions regarding communicability; symptomatology and diagnostics; at-risk individuals; prevention and treatment; and, virus characteristics of Ebola HF. Questions were designed after an intensive literature review by the research team. The responses to these questions were of multiple-choice type having one correct answer, including an option of “don't know” in some of questions.
Statistical analysis
The results were expressed in percentages. Multivariable linear regression analysis was carried out to assess the association of participants's demographic and professional characteristics with the knowledge scores. All significance tests were two tailed and P-value of less than 0.05 was considered to be statistically significant. All analysis were done using the Statistical Package of Social Sciences 17.0 software (SPSS Inc., Chicago, IL).
RESULTS
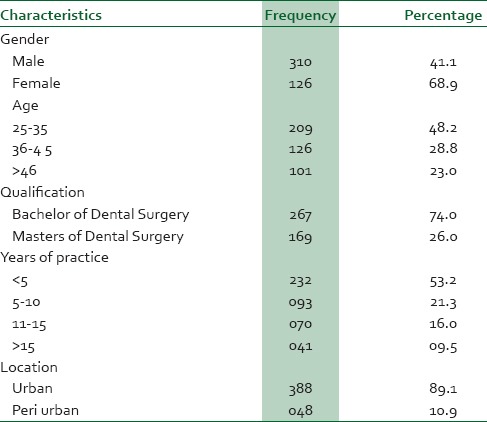
Out of the 500 dentists who were approached to participate in the survey, 436 agreed and completed the questionnaire. The socio-demographic characteristics of the sampled population are presented in Table 1. Majority of the subjects belonged to the age-group of 25-35 years (48.2%), were females (68.9%) with less than 5 years of clinical practice (53.2%), had a bachelor's degree in dentistry (74%) and belonged to urban areas (89.1%).
Table 1.
Demographic and professional characteristics of the participants of the study
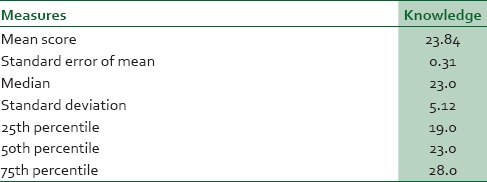
The mean (also the median) knowledge score of the respondents was 23.84 ± 5.12. The responses to the knowledge questions are depicted in Table 2.
Table 2.
Knowledge among study participants regarding Ebola HF
Ebola HF as a disease of viral origin was known to 80.9% of the participants, however, only 35.4% of the subjects were conscious of the fact that the infected person spread virus to others within 7 weeks after recovery from illness. Very few (37.1%) were aware that Fruit bats are the natural host of the Ebola organism. Majority (77.1%) were having knowledge that its outbreaks occur primarily in Central and West Africa.
Seventy eight percent were aware of fever, intense weakness, muscle pain and internal and external bleeding as the symptoms of Ebola HF. Availability of diagnostic tests during an outbreak that is PCR and ELISA were known to only 37.9%.
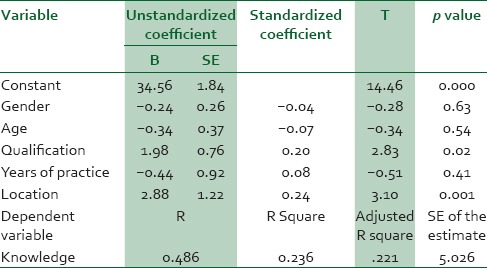
Multivariable linear regression analysis was carried out to find out the determinants of knowledge among the study participants. Of the five demographic and professional characteristics (age, gender, location, qualification and years of clinical practice) incorporated into the model, only location and qualification of the participant contributed significantly to the knowledge score indicating that participants, who are from urban areas and with a higher qualification had better knowledge (P < 0.05) [Table 3 Table 4].
Table 3.
Responses to the knowledge questions regarding Ebola HF by the participants of the study

Table 4.
Association between the demographic and professional characteristics of the participants with the knowledge scores using multivariate linear regression analysis
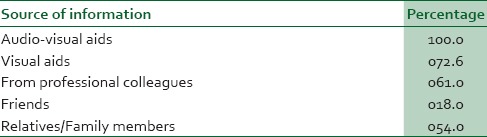
“Television” and “Newspaper” were the main sources of information followed by the “Professional colleagues”, “Relatives/family members”, “Friends” and “Radio” [Table 5].
Table 5.
Source of information about Ebola HF among the study participants
DISCUSSION
The public health significance of the disease, Ebola HF, lies not only in its potential to cause significant mortality and morbidity at community level, especially during outbreaks, but also its potential for nosocomial spread. Maintaining a high index of suspicion should only be based on adequate knowledge of the disease among the care providers. Also effective patient counselling and community campaigns can only be held out by health workers who are themselves adequately informed about the disease. It is thus important that health workers be conversant with the disease manifestations, management, prevention and also cross infection as well, that can be from a patient to dentist, from dentist to patient or from patient to patient as well.11,12
Thus this survey was carried out to provide a coherent description of dentists’ knowledge and position in this territory in regard to the Ebola HF and such an agreement is important to evaluate their effectiveness in the prevention of such infectious diseases.13
According to Centers for Disease Control and Prevention (CDC), the period of infectivity of Ebola virus begins the day before the onset of illness and can persist for up to 2-21 days after exposure to Ebola virus though 8-10 days is most common. It is of concern that in our study dentists lacked sufficient knowledge about the period of infectivity and duration of viability of the virus (35.4%).3
The results of the “knowledge level test” among the respondents to our questionnaire, (which had questions pertaining to the communicability; symptoms and diagnostics; prevention and treatment; and, virus characteristics of Ebola HF), suggest that knowledge among the dentists was fairly good (25th percentile value exceeded 55% of the highest knowledge score). However, there were some noteworthy yet disturbing gaps in knowledge at some places like for example knowledge regarding virus characteristics, infectivity period, diagnostic techniques available and virus elimination. Although WHO has provided documentation regarding Ebola HF investigation and control but only nearly half of the respondents that is 52.2% were aware of this, so dentists should need to regularly update their knowledge regarding epidemics and such diseases which will inculcate positive attitude and healthy practices in them.
In the present study the post graduate dental practitioners were found to have better knowledge scores than their graduate counterparts. This could be the reflection of regular upgradation of knowledge through scientific journals and other available electronic data which the postgraduate practitioners are well versed with since their post graduation times. It was also found that the dentists practicing in urban areas were found to have significantly higher knowledge scores than those who were practicing in peri urban areas. As more number of dental education programmes and conferences are held in urban areas, this gives advantage to urban practitioners to regularly update their knowledge about various fields including the prevention and spread of any infectious disease. These findings are in accordance with study conducted by Kaipa S et al., in Nellore, India.4
When comparison was made based on the gender, similar knowledge scores were found between the males and females which is in contradiction with the studies conducted by Kamate et al., and Leili et al.14,15 This shows that females in this region are equally interactive and as social as males and also they are equally concerned about increasing their knowledge banks.
Audio-visual aids were the most important source of information for Ebola HF followed by visual aids, family members and fellow colleagues. This could be because of increase in the number of news channels, daily broadcasting of the events pertaining to public health significance and special discussion programmes with the experts about the spread and prevention of this disease. This finding was similar to with the study conducted by and Apichaya et al, where television was the most important source of information for the public.6
The participants of this study constituted the convenient sampling so the sample may not be a representative one, however, to remove this limitation we do tried to incorporate as many as possible practitioners. Another thing to be mentioned is that only the knowledge scores have been considered here because it's a too early stage to assess the attitudes and practices in relation to Ebola HF, when very less is known about this disease. Nevertheless this study do opens new vistas for future researchers around the world, as this is one of its kind studies in dental and medical literature assessing the knowledge regarding Ebola HF.
CONCLUSION
The prevention of Ebola HF poses a number of challenges. It is still unknown how exactly people are infected with Ebola HF and also there are very few established primary prevention measures. When the cases appear, there is increased risk of transmission within medical and dental health care settings. Therefore, health care providers should be able to identify a case of Ebola HF and be ready to employ precautions or practical barrier nursing techniques. They should further be capable of requesting diagnostic tests or prepare samples for shipping and testing elsewhere.3
Through this study it was found that dentists’ knowledge regarding Ebola HF was fairly good. Participants from urban areas with higher qualification had better knowledge yet there were notable deficiencies regarding the virus characteristics, diagnostics, elimination and treatment. Emphasis should be given to create a perception towards public health significance of diseases as well as more number of continued dental education programmes should be carried out to disseminate the knowledge effectively regarding Ebola HF and other such highly infectious and fatal diseases.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1. [Last assessed on 2014 Sept 3]. Available from: www.cdc.gov/vhf/Ebola/pdf/fact-sheet.pdf . Tambo E.
- 2.Tambo E, Ugwu EC, Ngogang JY. Need of surveillance response systems to combat Ebola outbreaks and other emerging infectious diseases in African countries. Infect Dis Poverty. 2014;3:29. doi: 10.1186/2049-9957-3-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. [Last assessed on 2014 Sept 6]. Available from: http://www.cdc.gov/vhf/Ebola/resources/pdfs/Ebola-factsheet.pdf .
- 4.Kaipa S, Epari V, Gupta S. Knowledge and attitude towards swine influenza (2009) among dental practitioners in Nellore district of Andhra Pradesh, India. J Educ Ethics Dent. 2011;1:52–8. [Google Scholar]
- 5. [Last assessed on 2014 Sept 6]. Available from: http://crofsblogs.typepad.com/h5n1/2014/08/who-Ebola-update-cases-.html .
- 6.Apichaya S, Chaninat R, Theerin C, Supataradit B, Awapa P, Tongsreeneam N, et al. Knowledge, attitude and practice of pandemic H1N1 influenza prevention in Thailand. Online Abstract. [Last accessed on 2014 Aug 27]. Available from: http://beid.ddc.moph.go.th/th/images/news/cheraton2122_10_52/poster/Rassamee_poster01.pdf .
- 7.Reuters News Agency UN. Ebola seriously threatens Liberia's existence: Minister. Indian Express daily news paper. 2014 Sep 9; [Google Scholar]
- 8. [Last accessed on 2014 Sept 1]. Available from: https://www.osha.gov/SLTC/Ebola/control_prevention.html .
- 9. [Last accessed on 2014 Sept 4]. Available from: https://www.ndhan.gov/data/mrFacts/Ebola.pdf .
- 10.Puttaiah R, Miller K, Bedi DR, Shetty S, Almas K, Tse E, et al. Comparison of knowledge, attitudes and practice of dental safety from eight countries at the turn of the century. J Contemp Dent Pract. 2011;12:1–7. doi: 10.5005/jp-journals-10024-1001. [DOI] [PubMed] [Google Scholar]
- 11.Heir J, Ziccardi VB. Transmission of infectious disease in the dental setting. Mt Sinai J Med. 1998;65:378–82. [PubMed] [Google Scholar]
- 12. [Last accessed on 2014 Sept 9]. Available from: www.who.int/csr/disease/Ebola/en/
- 13.Di Giuseppe G, Nobile CG, Marinelli P, Angelillo IF. A survey of knowledge, attitudes, and behavior of Italian dentists toward immunization. Vaccine. 2007;25:1669–75. doi: 10.1016/j.vaccine.2006.10.056. [DOI] [PubMed] [Google Scholar]
- 14.Kamate SK, Agrawal A, Chaudhary H, Singh K, Mishra P, Asawa K. Public knowledge, attitude and behavioural changes in an Indian population during the Influenza A (H1N1) outbreak. J Infect Dev Ctries. 2009;4:7–14. doi: 10.3855/jidc.501. [DOI] [PubMed] [Google Scholar]
- 15.Farid-ul-Hasnain S, Johansson E, Krantz G. What do young adults know about the HIV/AIDS epidemic. Findings from a population based study in Karachi, Pakistan? BMC Infect Dis. 2009;9:38. doi: 10.1186/1471-2334-9-38. [DOI] [PMC free article] [PubMed] [Google Scholar]