

Abstract
Introduction:
Cardiovascular disease is the commonest cause of mortality worldwide. Many risk factors predate the development of cardiovascular diseases. Adequate knowledge of risk factors for cardiovascular diseases is the first step towards effective preventive strategies to combat the cardiovascular diseases burden in any population. This study aims to determine the knowledge of workers in a Nigerian University on risk factors for cardiovascular diseases.
Materials and Methods:
A cross-sectional survey of 206 academic and non-academic staff of Ladoke Akintola University of Technology, Ogbomoso, Nigeria using the Heart Disease Fact Questionnaire (HDFQ). Demographic data were taken. The lipid profile and random blood sugar were taken. Statistical analysis was done using SPSS 17.0.
Results:
The mean age of the study participants was 45.3 ± 7.9 years. There were 96 males (46.6%). The mean HDFQ score was 48.6%. Only 41 (19.9%) of participants were assessed to have good knowledge of heart disease risk factors. Majority, 101 (49.0%) had poor knowledge while 64 (31.2%) had fair knowledge of heart disease risk factors. There was no significant difference between prevalence of CV risk factors between those with good or fair or low level of knowledge. Most participants did not have a good level of knowledge about risk factors, prevention, treatment and association with diabetes as it relates to heart diseases.
Conclusion:
Knowledge of heart disease risk factors is low among University workers in Nigeria. Effective education on heart disease risk factors and appropriate preventive strategies are indeed important to reduce cardiovascular disease burden in Nigerian University communities.
Keywords: Heart disease, knowledge, Nigerian University, risk factors
INTRODUCTION
Heart disease is the number one cause of death worldwide accounting for about 30% of all causes of death globally in 2008. More people died from cardiovascular diseases than from any other cause in the recent years.1,2 Low and middle-income countries are disproportionately affected as more than 80% of cardiovascular disease deaths take place in these countries occurring almost equally in both men and women. The World Health Organization (WHO) estimated that 9.4 million deaths each year or 16.5% of all deaths can be attributed to high blood pressure.3,4 This include strokes and coronary heart disease.5 it has also been estimated that the number of people who will die from cardiovascular diseases mainly from heart disease and strokes will increase to reach 23.3 million by 2030 and cardiovascular diseases is projected to remain the leading cause of death globally.6
However, most cardiovascular diseases are preceded by CV risk factors and a major preventive strategy is to address CV risk factors such as tobacco use, unhealthy diet and obesity, physical inactivity, high blood pressure diabetes and dyslipidaemia.5,7 Effectively tackling these risk factors indicates that these risk factors are picked and modified early in the course of the disease progression.8 The individual or population awareness about these risk factors are therefore essential in adequate prevention.9 The INTERHEART study showed a consistency in the relationship between cardiovascular diseases and risk factors among Blacks and Whites in Africa.10 These risk factors are being reported in increasing prevalence across almost all parts of Africa.11,12,13 Yet there are very few data on the awareness of heart disease risk factors among the population.14
The knowledge of heart disease risk factors is essential to make informed decision that will result in reduction in overall cardiovascular risk of an individual. In the Health Belief Model (HBM), a person must feel susceptible to a disease in order to motivate a change in behaviour.15 Adequate knowledge and perception of risk are therefore important in stimulating behavioural change towards a better health. This study aimed to determine the level of awareness and level of knowledge of heart disease risk factors among adult University workers in Nigeria.
MATERIALS AND METHODS
This was part of another study on the prevalence of cardiovascular risk factors among University workers in Ladoke Akintola University of Technology, Ogbomoso, Nigeria. It was a cross-sectional descriptive study, The Heart Disease Fact Questionnaire (HDFQ) was used.
Two-hundred and six adult staff including academic and non-academic staff of the Ladoke Akintola University of Technology, Ogbomoso, Nigeria were randomly selected from all faculties and units of the University. Apart from the other part of the study which has been described elsewhere, the HDFQ Questionnaire was administered to each participant. The HDFQ Questionnaire is a 25-item measure of heart disease knowledge.16,17 which evaluates for knowledge of risk factors for heart disease, the link between diabetes and heart disease and how to reduce the risk for heart disease. Respondents were asked to mark one of the options including ‘True’, ‘false’ or ‘I don’t know’. Scores are calculated in percentages by summing the total number of correct answers with a higher score indication a higher knowledge. Participants with score of <50% were classified as low level of knowledge while those whose score were between 50 and 69% were classified as moderate level of knowledge and those with HDFQ score>70% as good level of knowledge. Questions that <70% of the respondents answered correctly was deemed unsatisfactory. The HDFQ Questionnaire has been used in other population with reliable test-retest reliability, internal consistency and satisfactory discriminant validity.18
The demographic parameters were taken using a pretested data sheet. Information obtained includes age, gender, highest level of education, systolic and diastolic blood pressure, weight, height, waist circumference and marital status. Laboratory parameters taken include random blood sugar, lipid profile (including triglycerides, total cholesterol, high density lipoprotein cholesterol and low density lipoprotein- cholesterol) were taken.
Statistical analysis was performed with the aid of the Statistical Package for Social Sciences SPSS 17.0 (Chicago Ill). Data were summarised using means and standard deviation for quantitative variables and frequencies and percentages for qualitative variables. Relationship between continuous variables was tested using the Analysis of Variance while the Pearson Chi-Square test was used to test for relationship between qualitative/nominal variables. P < 0.05 was taken as statistically significant. Ethical approval was obtained from the Institutional Ethical Research Board.
RESULTS
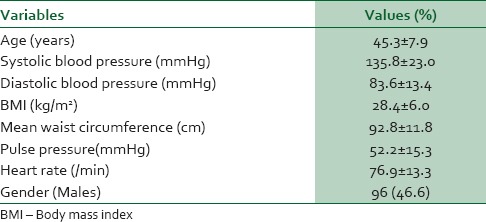
The mean age of the study participants was 45.3 ± 7.9 years. There were 96 males (46.6%) and 110 female participants (53.6%). The mean body mass index was 28.4 ± 6.0 kg/m2. The mean systolic and diastolic blood pressures were 135.8 ± 23.0 mmHg and 83.6 ± 13.4 mmHg respectively. The mean waist circumference was 92.8 ± 11.8 cm. Seventy-nine (38.3%) of the participants had body mass index >30 kg/m2. This is as in Table 1.
Table 1.
Demographic characteristics of study participants
The HDFQ scores were used to determine the level of knowledge of heart disease. Those with HDFQ score >70% were assessed to have good knowledge, those with score between 50 and 69% were said to have moderate knowledge and those with score <50% as low level of knowledge. About half of all the participants had low level of knowledge 49.0% compared to 31.1% with moderate level of knowledge and 19.9% with good level of knowledge. Table 2 shows that there was no statistically significant difference between those with low, moderate or high level of knowledge as it regards highest level of education. There was also no significant difference between those with different level of knowledge as it is associated with prevalence of hypertension, family history of hypertension and obesity. There was no significantly difference between age and level of knowledge among study participants.
Table 2.
Demographic characteristics of those with a high HDFQ score compared to low HDFQ score
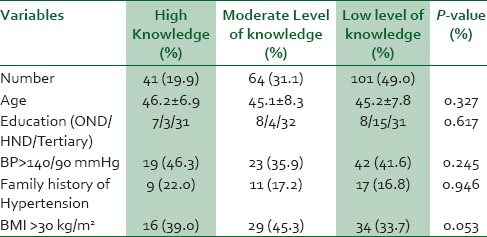
Table 3 shows the response of the participants to the questions in the Heart disease fact Questionnaire in this study. Among the questions which showed the greatest consistency with the highest rate of agreement include knowing that smoking is a risk factor for heart disease ad that treating elevated blood pressure can lead to reduction the risk of developing heart disease. These were the only two questions where participants scored >70% and the participants showed a good level of knowledge as it relates to risk factor for heart disease.
Table 3.
Frequency of answers given to different questions in the heart disease frequency questionnaire by the participants
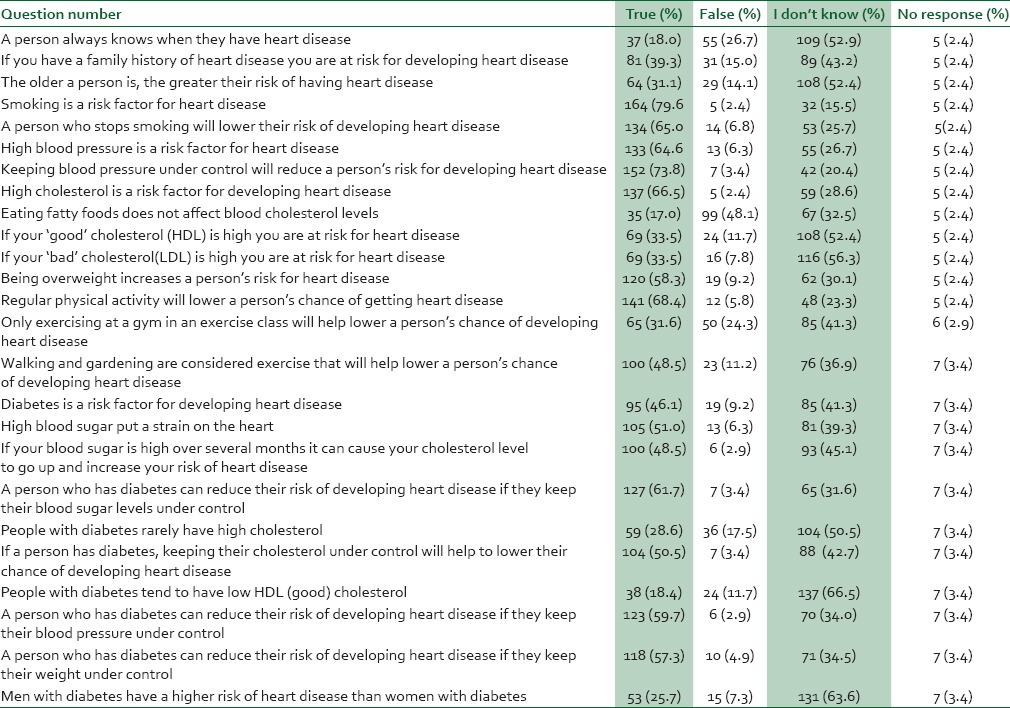
As in Table 3, the participants showed a moderate level of knowledge as it regards three facts: Firstly, that a person who stops smoking will lower their risk of developing heart disease. Secondly, that high blood pressure is a risk factor for heart disease and thirdly that high blood cholesterol is a risk factor for heart disease. Other questions which showed moderate consistency in the level of knowledge include being overweight increases the chance of someone developing heart disease, diabetes is a risk factor for heart disease and the fact that subject with diabetes can reduce their risk of heart disease if they control their blood pressure, cholesterol, weight and blood sugar. Among those facts with consistent low level of knowledge in the participants include the fact that diabetes have low HDL, the people with heart disease always knows about it and the fact that eating fatty foods affect blood cholesterol level. This is shown in Table 3.
DISCUSSION
The major outcome of this study revealed that majority of the participants in this study had poor knowledge of heart disease risk factors even though they work in the University community. Only about a fifth had a very good level of knowledge of heart disease risk factors among the study participants. There was no relationship among age, gender or education level and the level of knowledge of heart disease risk factor as estimated with the HDFQ score. We also found no significant difference between those with high level of knowledge in the mean value of total cholesterol, systolic and diastolic blood pressure, triglycerides, low density lipoprotein and body mass index. Other researchers have shown that age and gender were associated with level of knowledge.19
Although, this is one of the first set of evidence for low knowledge of heart disease risk factors using the HDFQ Questionnaire, other studies have shown an inappropriately low level of knowledge of coronary heart disease using other instruments among University staff.14
Similarly, Wagner et al. showed that knowledge of heart disease risk factors was low even among Spanish speakers with diabetes in a survey of diabetic subjects from Puerto Rico.18 The mean level of knowledge is even lower among other similar population.
This study also showed that HDFQ scores were not in any way related to some demographic factors such as age, gender or presence of cardiovascular diseases. The pattern of cardiovascular disease was also not significantly related to the pattern of cardiovascular risk factors among the participants in this study. Much curiously is the fact that the level of education did not significantly associated with the level of knowledge of cardiovascular risk factors as many people with higher degrees including academic staff had limited knowledge about risk factors for heart diseases in this study. This is contrary to the study by Wagner who showed that those with a high-school certificate were much likely to have a higher HDFQ score than those without a high-school certificate.19 In that study also, those with a bank account were also much likely to a have a higher HDFQ score than those without a bank account and this is likely to be related to their level of education and socio-economic status. We did not assess the highest income in this study but it can be assumed that all participants were not likely to be less than in the middle class considering the many opportunities for distinctive salary scale, emolument and allowances and other opportunities available to University workers.
This study revealed some major findings: Questions 1-8 in the HDFQ are related to the knowledge about cardiovascular risk factors such as smoking, hypertension, family history of heart disease, overweight, etc. Surprisingly, only in the relationship between smoking and heart disease was the level of knowledge adjudged to be good. The participant knowledge about the relationship between hypertension and heart disease was at best moderate although most people know that treating high blood pressure could result in reduction in chance to develop heart disease. The participants’ level of knowledge as it concerns its association with cholesterol fractions was abysmally low. This is despite the fact that the first risk factor to be associated with heart disease was cholesterol in the Framingham study.20 Similarly, the average level of knowledge as it relate to preventive strategies in questions 13-15 were also at best moderate. Only 48.5% of the participants agreed that walking and gardening are considered exercise that will help lower a person's chance of developing heart disease although 68.4% agreed that regular physical activity will lower a person's chance of getting heart disease. The last aspect of the HDFQ identified the level of knowledge on diabetes as it relates to heart disease. The level of knowledge is also averagely low as only about half agreed that diabetes is a risk factor for heart disease. A worse outcome was obtained when testing for knowledge of association between diabetes and cholesterol profile as it relates to heart disease. The outcome of this study shows a much lower level of knowledge as it concern level of knowledge of heart disease when compared to a similar report among African-Americans although they were a bit younger in that study.21
There appear to be a general poor level of knowledge on the main risk factors, prevention, relationship of cholesterol, diabetes and heart disease among Nigerian University workers in LAUTECH, Ogbomoso, Nigeria. Despite the surging trend in cardiovascular disease worldwide and in developing nations like Nigeria and having reported that in this environment, the commonest reason for medical admission to Teaching Hospital are cardiovascular disease,22,23,24 there is still poor level of knowledge of heart disease among University workers. An outreach programme including training on the risk factors for heart diseases, preventive strategies, treatment and association with cholesterol and diabetes is, therefore, very essential.
Africans including African-Americans have been shown to have higher rates of cardiovascular disease. They should therefore be targeted for interventions to prevent or reduce the burden of cardiovascular diseases. Therefore, increasing the level of knowledge of heart disease risk factors, prevention and treatment remain a major way to reduce the burden of cardiovascular diseases among Africans.
CONCLUSION
This outcome of this study is a call for action among University administrators in Nigeria. In order to achieve a healthy workforce and reduce incapacitation, University workers must be exposed adequately to increased cardiovascular awareness as they may be at increased risk due to low level of knowledge and awareness of heart disease risk factors among them. This poor level of knowledge is inexorably a harbinger of poor preventive modalities for cardiovascular disease among them.
Appropriate health education to increase awareness about heart disease risk factors remains the fulcrum of preventing increased cardiovascular risk among Nigerian University workers. University administrators should, therefore, design and implement massive, cost-effective long term health education for University workers to prevent cardiovascular morbidity and mortality among them in the nearest future.
ACKNOWLEDGEMENT
We wish to acknowledge the residents in cardiology unit of Department of medicine, LAUTECH Teaching Hospital, Ogbomoso, Nigeria for their assistance in data acquisition in this study.
Footnotes
Source of Support: The Authors gratefully acknowledge the financial support received from Ladoke Akintola University of Technology, Ogbomoso, Oyo State, Nigeria through Senate Research Grant LAU/SRG/13/001
Conflict of Interest: None declared.
REFERENCES
- 1.Global status report on non-communicable diseases 2010. Geneva: World Health Organization; 2011. [Google Scholar]
- 2.Global atlas on cardiovascular disease prevention and control. Geneva: World Health Organization; 2011. [Google Scholar]
- 3.Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions.1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–60. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kengne AP, June-Rose McHiza Z, Amoah AG, Mbanya JC. Cardiovascular diseases and diabetes as economic and developmental challenges in Africa. Prog Cardiovasc Dis. 2013;56:302–13. doi: 10.1016/j.pcad.2013.10.011. [DOI] [PubMed] [Google Scholar]
- 6.The global burden of disease: 2004 update. Geneva: World Health Organization; 2008. [Google Scholar]
- 7.Muna WF. Comprehensive strategies for the prevention and control of diabetes and cardiovascular diseases in Africa: Future directions. Prog Cardiovasc Dis. 2013;56:363–6. doi: 10.1016/j.pcad.2013.10.012. [DOI] [PubMed] [Google Scholar]
- 8.Kadiri S. Tackling cardiovascular disease in Africa. BMJ. 2005;331:711–2. doi: 10.1136/bmj.331.7519.711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pearson TA. Education and income: Double-edged swords in the epidemiologic transition of cardiovascular disease. Ethn Dis. 2003;13:S158–63. [PubMed] [Google Scholar]
- 10.Steyn K, Sliwa K, Hawken S, Commerford P, Onen C, Damasceno A, et al. INTERHEART Investigators in Africa. Risk factors associated with myocardial infarction in Africa: the INTERHEART Africa study. Circulation. 2005;112:3554–61. doi: 10.1161/CIRCULATIONAHA.105.563452. [DOI] [PubMed] [Google Scholar]
- 11.Coleman R. Disease burden in sub-Saharan Africa. Lancet. 1998;351:1208. doi: 10.1016/S0140-6736(05)79158-3. [DOI] [PubMed] [Google Scholar]
- 12.Ogah OS, Rayner BL. Recent advances in hypertension in sub-Saharan Africa. Heart. 2013;99:1390–7. doi: 10.1136/heartjnl-2012-303227. [DOI] [PubMed] [Google Scholar]
- 13.Twagirumukiza M, De Bacquer D, Kips JG, de Backer G, Stichele RV, Van Bortel LM. Current and projected prevalence of arterial hypertension in sub-Saharan Africa by sex, age and habitat: An estimate from population studies. J Hypertens. 2011;29:1243–52. doi: 10.1097/HJH.0b013e328346995d. [DOI] [PubMed] [Google Scholar]
- 14.Ansa VO, Oyo-Ita A, Essien OE. Perception of ischaemic heart disease, knowledge of and attitude to reduction of its risk factors. East Afr Med J. 2007;84:318–23. doi: 10.4314/eamj.v84i7.9586. [DOI] [PubMed] [Google Scholar]
- 15.Jones DE, Weaver MT, Grimley D, Appel SJ, Ard J. Health Belief Model perceptions, knowledge of heart disease, and its risk facfors in educated African-American women: An exploration of the relationships of socio-economc status and age. J Natl Black Nurse Assoc. 2006;17:13–23. [PubMed] [Google Scholar]
- 16.Wagner J, Lacey K, Chyun D, Abbott G. Development of a questionnaire to measure heart disease risk knowledge in people with diabetes: The Heart Disease Facts Questionnaire. Patient Educ Couns. 2005;58:82–7. doi: 10.1016/j.pec.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 17.Lacey K, Dixon J, Chyun D. Development of the heart disease facts questionnaire. Presented at eastern Nursing Research Society 13th Annual Scientific sessions 2001; Atlantic City, Ney Jersey. [Google Scholar]
- 18.Wagner J, Abbott G, Lacey K. Knowledge of heart disease risk among Spanish speakers with diabetes: The role of interpreters in the medical encounter. Ethn Dis. 2005;15:679–84. [PubMed] [Google Scholar]
- 19.Pratt CA, Ha L, Levine SR, Pratt CB. Stroke knowledge and barriers to stroke prevention among African-Americans: Implications for health communication. J Health Commun. 2003;8:369–81. doi: 10.1080/10810730305725. [DOI] [PubMed] [Google Scholar]
- 20.Grundy SM, Balady GJ, Criqui MH, Fletcher G, Greenland P, Hiratzka LF, et al. Primary prevention of coronary heart disease: Guidance from Framingham: A statement for Healthcare professionals from the AHA task Force on Risk Reduction. American Heart Association. Circulation. 1998;97:1876–87. doi: 10.1161/01.cir.97.18.1876. [DOI] [PubMed] [Google Scholar]
- 21.Winham DM, Jones KM. Knowledge of young African American adults about heart disease: A cross sectional survey. BMC Public Health. 2011;11:248. doi: 10.1186/1471-2458-11-248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Okunola OO, Akintunde AA, Akinwusi PO. Some emerging issues in medical admission pattern in the tropics. Niger J Clin Pract. 2012;15:51–4. doi: 10.4103/1119-3077.94098. [DOI] [PubMed] [Google Scholar]
- 23.Ike SO. Prevalence of hypertension and its complication among medical admissions at the University of Nigeria teaching Hospital, Enugu (Study 2) Niger J Med. 2009;18:68–72. [PubMed] [Google Scholar]
- 24.Odenigbo CU, Oguejiofor OC. Pattern of medical admissions at the Federal medical centre, Asaba-a two year review. Niger J Clin Pract. 2009;12:395–7. [PubMed] [Google Scholar]