

Abstract
Background:
Trauma remains a leading cause of maxillofacial injury globally. Changing etiological factors and patterns of maxillofacial injury continue to be reported and are largely modulated by socio-geographic and environmental factors. It is important to have an in-depth understanding of the pattern and etiology in a particular region before effective preventive measures can be developed.
Aim:
The aim was to evaluate the patterns, etiological factors, and management of maxillofacial injuries in Ogun state, Nigeria.
Materials and Methods:
A prospective descriptive cohort study of all consecutive patients that presented with maxillofacial injuries at our center between January and December 2013. Information about demographic data, types of maxillofacial and associated injury, etiology of injury, treatment received and complications were collected and analyzed.
Results:
Seventy patients presented with maxillofacial injury during the study period with a male to female ratio of 4:1. The age range was 9 months to 60 years with a mean of 30.11 ± standard deviation 14.97 years. Majority of the facial fractures were due to motorcycle related crashes. There were 57.1% mandibular fractures and 55.7% middle third fractures. Closed reduction with maxillo-mandibular fixation was the major method of treatment of facial fractures. Postoperative complications were observed in 11.4% of patients.
Conclusion:
Road traffic crashes (RTCs) remain the leading etiological factor of maxillofacial injuries in our center. Enforcement of stricter traffic regulations and possibly replacement of motorcycles with tricycles for commercial transportation may help to reduce the incidence of RTCs.
Keywords: Etiological factors, management, maxillofacial injuries, pattern, road traffic crashes
INTRODUCTION
Trauma remains a major health burden worldwide despite the various preventive measures that have been developed.[1] The major burden of trauma estimated at about 90% is borne by middle and low-income countries.[2] During the trauma; the maxillofacial region is highly vulnerable to injury either in isolation or in combination with other systems because of its exposure.[3]
The changing etiological factors and patterns of maxillofacial injuries reported from different regions at different times is largely modulated by prevailing socioeconomic, cultural, environmental and legislative factors, as well as location of the trauma center.[4,5,6] Recently, published literature shows that assault and inter-personal violence (IPV) are beginning to overtake road traffic crashes (RTCs) as the leading cause of maxillofacial injuries in the developed countries.[5,7,8] On the other hand, RTCs continues to be indicted as the leading cause of maxillofacial injuries from developing countries, although, significant changes in the etiology, mechanism and patterns of injury are being reported.[4,6,8,9] Over the last two decades, the increase in the use of motorcycles[9] as a mode of commercial transportation in developing countries including Nigeria has significantly affected the pattern of maxillofacial injuries.[9,10]
Studies have shown significant reduction in maxillofacial injuries in states where preventive measures have been effectively implemented.[5,11] A clear understanding of the mechanisms of injury from other studies will help evaluate the effectiveness of current safety and preventive measures, and also the pave way for newer innovations in this area. This information could also be used as a guide to the development and future funding of public health preventive programs.[12]
This study aims to prospectively evaluate the patterns, etiological factors, severity, management and the outcomes of maxillofacial trauma at a tertiary maxillofacial center.
MATERIALS AND METHODS
This was a prospective descriptive cohort study of consecutive patients with maxillofacial injuries that presented and were managed at our center between January and December 2013.
Data collected relates to patients’ demography, the mechanisms of injuries, patterns of trauma, soft tissue and bony structural classification, associated systemic injuries, treatment, length of hospital stay, associated complications and outcomes. These data were collected using a well-designed data sheet before entering into the database for analysis. All patients were initially managed according to the advanced trauma life support protocols. The hospital Ethics Committee approved the study.
The causes of the reported injuries were classified based on their mechanisms into RTCs, falls, assault, gunshot and sports related. Information relating to the use of seatbelts/helmets at the time of the incident was also obtained where applicable. Anatomic locations of mandibular fractures were classified according to Ivy and Curtis[13] system while maxillary fractures were classified using the Le fort[14] system.
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 17.0 for Windows (SPSS, Chicago IL, USA). Data were presented using descriptive statistics.
RESULTS
A total of 70 patients presented with 79 maxillofacial fractures, 49 soft tissues and 32 concomitant systemic injuries during the study period. The mean age was 30.11 years (9 months–60 years, standard deviation = 14.97). The peak age of incidence was in the 3rd decade of life (n = 20, 28.6%). Males accounted for 80% of the patients in this study with a male to female ratio of 4:1. RTCs accounted for 70% of the reported cases of the injuries. The distribution of the etiological factors is shown in Table 1. Twenty-two (31.4%) of the patients had isolated mandibular fracture, 11 (15.7%) had isolated middle-third fractures while 9 (12.9%) had combined middle third and mandibular fractures. In all there were 40 (57.1%) mandibular fractures and 39 (55.7%) middle-third fractures. With regards to mandibular fractures, the body (20%) was the most common site while the ramus and symphysis (1.4% each) were least affected. In the middle third, zygomatic bone fracture (18.6%) was the commonest while naso-orbito-ethmoidal complex fracture (1.4%) accounted for the least fracture seen in this study. Fifty-two (74.3%) patients sustained associated soft tissue injuries, and these were lacerations in 70% of the cases. Other associated systemic injuries were recorded in 26 (37.1%) patients with orthopedic injuries accounting for the majority of the cases. The patterns and the distributions of the injuries are shown in Figure 1.
Table 1.
Etiological factors of maxillofacial injuries

Figure 1.
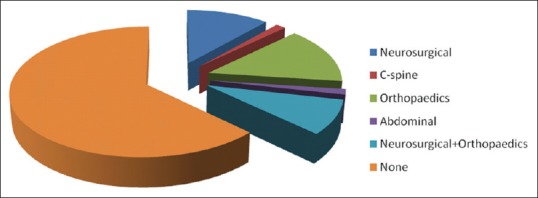
Distribution of associated systemic injuries
Only 8.6% and 4.3% of the patients that sustained injuries from vehicular and motorcycle road traffic crashes were seatbelt restrained and used crash helmets at the time of the accident respectively.
Majority of the patients (98.6%) denied being under the influence of alcohol at the time of the crash.
In this study, closed reduction with maxillo-mandibular fixation was the major method of treatment of facial fractures (35.7%) and only 2 (2.9%) patients were managed by an open reduction with internal fixation. Figure 2 shows the distribution of the treatment modalities offered. There were delays in accessing definitive treatment by 11.4% of the patients.
Figure 2.

Distribution of maxillofacial injuries
These delays were mainly due to the lack of funds for accessing healthcare (4.3%) and logistic delay in accessing the operating theatre space (4.3%).
Figure 3 shows the related complications following maxillofacial injuries.
Figure 3.

Distribution of associated complications
DISCUSSION
Epidemiological differences in the patterns and occurrence of maxillofacial injuries have been well reported as a result of socio-economic, cultural, legislative and environmental influences.[4,5,6] However, despite the changing patterns, global epidemiological surveys have revealed that some aspects of the facial fracture patterns remain similar among the various nations.[15] The results of this study are largely in agreement with those of previous reports, particularly regarding age incidence and gender distribution of patients. In this study, male predominance is comparable with previous studies.[6,15] However, the gender ratio in the present study is much lower compared to the 23:1 reported in a previous study from the northern part of Nigeria.[16] Females in the southern part of Nigeria participate more in social, public, work and sports related activities than their northern counterparts who are restricted for cultural and religious reasons and may not be as vulnerable to trauma.[6] Our findings of the highest frequency of injuries in the 3rd and 4th decades of life is in agreement with those reported elsewhere.[9,17] This is attributed to the fact that this age group is the most active phase of life.
Road traffic crashes accounted for the majority (70%) of maxillofacial injuries in this study, similar to previous reports.[4,6,9,15,17] RTCs remain the leading cause of trauma in the developing world because of non-observance and lack of strict enforcement of speed limits, use of restraining seatbelts and wearing of protective crash helmets. Furthermore, several roads are in bad repair, vehicles are poorly maintained and have minimal safety features.[18] Conversely, in several developed countries, there is a downward trend of RTCs related maxillofacial injuries with IPV and assault becoming the leading etiological factors. This decrease has been attributed to strict enforcement of protective measures and various traffic legislations.
The recent increase of commercial motorcycle transportation has also been blamed for the increase in RTCs in Nigeria.[9,10] This is also shown in the current study as half of the motor-vehicular RTCs causing maxillofacial injuries were due to motorcycle incidents. We noted that during the period of this study, no tricycle related maxillofacial injury was observed among our patients. Indeed, several governmental agencies in Nigeria have introduced the tricycle to replace commercial motorcycle transportation; to reduce the incidence of motorcycle related injuries. Global reports show a low incidence of tricycle related-crashes even in countries where it forms a major mode of commercial transportation. The low incidence of tricycle crashes is due to a number of factors; the speed that the tricycle can attain is limited, the design of three wheels gives it better stability compared to the motorcycle, the tricycle has a housing protecting the occupants unlike the motorcycle that completely exposes the driver and passenger to the environment. The motorcycle driver can easily make risky maneuverings because of its narrow design and this is less likely with a tricycle.
A rare cause of maxillofacial trauma is epileptic fits and other forms of convulsions. One of the patients in the current study sustained a deep laceration of the tongue following epileptic fits requiring suturing. A study from Nigeria reported the incidence of orofacial injuries among enclamptic patients to be 42%.[19] The low incidence reported in our study could be due to the patients presenting at other units. Alcohol abuse has been reported to be linked to maxillofacial injuries from violence in several studies, the incidence ranging between 20% and 56%.[20,21] This has been attributed to the capacity of alcohol to impair judgment and fuel violence.[5] A study from the northern part of Nigeria observed an increase in the prevalence of alcohol-related maxillofacial fractures after annual periods of religious fasting.[22] In the present study, alcohol-related maxillofacial injury only accounted for 1.4% of our cases.
In the current study, there was a slight preponderance of mandibular fractures (57.1%) compared to midface fractures (55.7%). This is in contrast to the previously published reports.[6,12] The small sample size recorded in this study might have accounted for this disparity. In the agreement with previously published data, however,[23] the body of the mandible was the most common site of fracture, closely followed by the parasymphysis. Furthermore, fractures of the body of the mandible were the most frequent fractures due to road traffic accidents while the angle was most affected due to assaults and these findings agree with previous studies.[23,24]
Considerable variations exist in the rate of systemic injuries associated with maxillofacial fractures ranging from 12% to 46%.[6,15,22] These variations are due to lack of standardized definitions and classification of such injuries worldwide. Developing countries have recorded orthopedic injuries[6,22] as the most frequent associated trauma but reports from the developed world support cranial injuries.[25] About ⅓ of the patients (37.1%) in this study sustained concomitant injuries of which orthopedic cases formed the bulk (22.9%). These differences could be a reflection of the variation in etiology, poor utilization of protective devices as well as poor pre-hospital management in our environment, leading to more non-survivable fatal craniofacial injuries arriving at the hospital.[9] Because motorcycle is the major etiology, most of the patients surviving to the hospital are more likely to sustain orthopedic injuries because they are exposed on the bike.
Open reduction and internal fixation (ORIF) is fast becoming the gold standard for management of maxillofacial fractures.[1,26] However, the closed method of fracture reduction was employed in most (38.6%) of the patients in this study, and this pattern is similar to those of previous reports from developing nations.[16,23] Only 2.9% of our patients had open reduction with trans-osseous wiring at the fronto-zygomatic region. The low rate of ORIF in this study was because of the unaffordability of such treatment in an environment where patients are responsible for the costs.
The rate of complication in our study was 11.4%, similar to a Norwegian study,[27] higher than 7.5% reported by a Chinese study[1] but much lower than the 25.26% reported in another study.[28] Most studies report infection as the commonest complication. In our study, infection and malocclusion (2.9% each) were the commonest complications, similar to the trend reported in an India study.[28] The infection in our study was mainly seen in patients that were not so compliant with the post-operative oral care instructions. This was particularly more relevant as mandibullo-maxillary fixation needed a high degree of diligence and compliance to keep a good oral hygiene and prevent infection. Some of the patients had delays in receiving treatment for financial and logistic reasons. Achieving a perfect occlusal harmony without open reduction in some old fracture cases is difficult, and this may explain the few cases of malocclusion recorded in this study.
CONCLUSION
This study shows that motorcycle related crashes are the leading etiological factor of maxillofacial injuries in our center. The demographic patterns in this study mirror the one reported in the literature. The mandibular bony frame is the most fractured bone of the face in a similar version to that reported in the published series. There is an urgent need for strict enforcement of adherence to speed limits, the use of the seatbelt and the wearing of safety helmets by motorcyclists. Use of tricycles to replace commercial motorcycle transportation may help to reduce RTCs in our environment.
Footnotes
Source of Support: Nil
Conflicts of Interest: None declared.
REFERENCES
- 1.Mijiti A, Ling W, Tuerdi M, Maimaiti A, Tuerxun J, Tao YZ, et al. Epidemiological analysis of maxillofacial fractures treated at a university hospital, Xinjiang, China: A 5-year retrospective study. J Craniomaxillofac Surg. 2014;42:227–33. doi: 10.1016/j.jcms.2013.05.005. [DOI] [PubMed] [Google Scholar]
- 2.Hofman K, Primack A, Keusch G, Hrynkow S. Addressing the growing burden of trauma and injury in low-And middle-income countries. Am J Public Health. 2005;95:13–7. doi: 10.2105/AJPH.2004.039354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Madubueze CC, Chukwu CO, Omoke NI, Oyakhilome OP, Ozo C. Road traffic injuries as seen in a Nigerian teaching hospital. Int Orthop. 2011;35:743–6. doi: 10.1007/s00264-010-1080-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: A review of the literature. Head Face Med. 2005;1:7. doi: 10.1186/1746-160X-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lee K. Global trends in maxillofacial fractures. Craniomaxillofac Trauma Reconstr. 2012;5:213–22. doi: 10.1055/s-0032-1322535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ugboko VI, Odusanya SA, Fagade OO. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. A review of 442 cases. Int J Oral Maxillofac Surg. 1998;27:286–9. doi: 10.1016/s0901-5027(05)80616-2. [DOI] [PubMed] [Google Scholar]
- 7.Ström C, Nordenram A, Fischer K. Jaw fractures in the county of Kopparberg and Stockholm 1979-1988. A retrospective comparative study of frequency and cause with special reference to assault. Swed Dent J. 1991;15:285–9. [PubMed] [Google Scholar]
- 8.Ogundare BO, Bonnick A, Bayley N. Pattern of mandibular fractures in an urban major trauma center. J Oral Maxillofac Surg. 2003;61:713–8. doi: 10.1053/joms.2003.50118. [DOI] [PubMed] [Google Scholar]
- 9.Ajike SO, Adebayo ET, Amanyiewe EU, Ononiwu CN. An epidemiologic survey of maxillofacial fractures and concomitant injuries in Kaduna, Nigeria. Niger J Surg Res. 2005;7:251–5. [Google Scholar]
- 10.Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg. 2006;64:56–62. doi: 10.1016/j.joms.2005.09.027. [DOI] [PubMed] [Google Scholar]
- 11.Laski R, Ziccardi VB, Broder HL, Janal M. Facial trauma: A recurrent disease? The potential role of disease prevention. J Oral Maxillofac Surg. 2004;62:685–8. doi: 10.1016/j.joms.2003.12.008. [DOI] [PubMed] [Google Scholar]
- 12.Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: A review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:166–70. doi: 10.1016/j.tripleo.2004.01.020. [DOI] [PubMed] [Google Scholar]
- 13.Ivy RH, Curtis L. Fractures of the mandible, an analysis of 100 cases. Dent Cosm. 1926;68:439. [Google Scholar]
- 14.Le Fort R. Experimental study of fractures of the upper jaw. Rev Chir. 1901;23:208–359. [Google Scholar]
- 15.Mesgarzadeh AH, Shahamfar M, Azar SF, Shahamfar J. Analysis of the pattern of maxillofacial fractures in north western of Iran: A retrospective study. J Emerg Trauma Shock. 2011;4:48–52. doi: 10.4103/0974-2700.76837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Adekeye EO. Fractures of the zygomatic complex in Nigerian patients. J Oral Surg. 1980;38:596–9. [PubMed] [Google Scholar]
- 17.Fasola AO, Lawoyin JO, Obiechina AE, Arotiba JT. Inner city maxillofacial fractures due to road traffic accidents. Dent Traumatol. 2003;19:2–5. doi: 10.1034/j.1600-9657.2003.00073.x. [DOI] [PubMed] [Google Scholar]
- 18.Zargar M, Khaji A, Karbakhsh M, Zarei MR. Epidemiology study of facial injuries during a 13 month of trauma registry in Tehran. Indian J Med Sci. 2004;58:109–14. [PubMed] [Google Scholar]
- 19.Adeyemo WL, Rabiu KA, Okoturo TM, Adebanjo AA, Adewunmi AA, Adeyemi MO. Orofacial injuries associated with eclampsia in patients presenting at a Nigerian Tertiary hospital. J Obstet Gynaecol. 2012;32:54–7. doi: 10.3109/01443615.2011.613495. [DOI] [PubMed] [Google Scholar]
- 20.McDade AM, McNicol RD, Ward-Booth P, Chesworth J, Moos KF. The aetiology of maxillo-facial injuries, with special reference to the abuse of alcohol. Int J Oral Maxillofac Surg. 1982;11:152–5. doi: 10.1016/s0300-9785(82)80002-1. [DOI] [PubMed] [Google Scholar]
- 21.Sojot AJ, Meisami T, Sandor GK, Clokie CM. The epidemiology of mandibular fractures treated at the Toronto general hospital: A review of 246 cases. J Can Dent Assoc. 2001;67:640–4. [PubMed] [Google Scholar]
- 22.Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg. 2002;40:140–3. doi: 10.1054/bjom.2001.0716. [DOI] [PubMed] [Google Scholar]
- 23.Dongas P, Hall GM. Mandibular fracture patterns in Tasmania ten years of mandibular fractures: An analysis of 2137 cases. Aust Dent J. 2002;47:131–7. doi: 10.1111/j.1834-7819.2002.tb00316.x. [DOI] [PubMed] [Google Scholar]
- 24.Ansari MH. Maxillofacial fractures in Hamedan province, Iran: A retrospective study (1987-2001) J Craniomaxillofac Surg. 2004;32:28–34. doi: 10.1016/j.jcms.2003.07.010. [DOI] [PubMed] [Google Scholar]
- 25.Luce EA, Tubb TD, Moore AM. Review of 1,000 major facial fractures and associated injuries. Plast Reconstr Surg. 1979;63:26–30. doi: 10.1097/00006534-197901000-00005. [DOI] [PubMed] [Google Scholar]
- 26.Obwegeser JA. Osteosynthesis using biodegradable Poly-p-dioxanon (PDS II) in Le Fort I-osteotomy without postoperative intermaxillary fixation. J Craniomaxillofac Surg. 1994;22:129–37. doi: 10.1016/s1010-5182(05)80377-4. [DOI] [PubMed] [Google Scholar]
- 27.Torgersen S, Tornes K. Maxillofacial fractures in a Norwegian district. Int J Oral Maxillofac Surg. 1992;21:335–8. doi: 10.1016/s0901-5027(05)80756-8. [DOI] [PubMed] [Google Scholar]
- 28.Kamath RA, Bharani S, Hammannavar R, Ingle SP, Shah AG. Maxillofacial trauma in central karnataka, India: An outcome of 95 cases in a regional trauma care centre. Craniomaxillofac Trauma Reconstr. 2012;5:197–204. doi: 10.1055/s-0032-1322536. [DOI] [PMC free article] [PubMed] [Google Scholar]