

Abstract
Objective:
The incidence of and risk factors for hypocalcemia following thyroidectomy were evaluated in this study.
Material and Methods:
One hundred and ninety thyroidectomy patients were evaluated retrospectively for factors that might contribute to postoperative hypocalcemia; age, hyperthyroidism, malignancy, the extent of surgery (total/near total/subtotal thyroidectomy), cervical lymph node dissection, and incidental parathyroidectomy.
Results:
The rate of transient hypocalcemia/hypoparathyroidism was 19.47%, with a permanent hypoparathyroidism rate of 4.74%. Factors affecting the development of transient hypocalcemia were found as being operated for hyperthyroidism, and use of total thyroidectomy as the surgical method. Total thyroidectomy increased the risk of postoperative hypocalcemia by 3.16 fold. Patients undergoing operations for hyperthyroidism had a 2.3 fold increase, and those undergoing total thyroidectomy had a 3.16 fold risk of postoperative hypocalcemia.
Conclusion:
Hyperthyroidism surgery and total thyroidectomy lead to a higher risk of developing early postoperative or transient hypocalcemia. According to our results, no significant relationship could be established between any of the study parameters and persistent hypocalcemia.
Keywords: Thyroidectomy, transient hypocalcemia, permanent hypoparathyroidism, risk factors
INTRODUCTION
Thyroidectomy meaning partial or complete removal of thyroid tissue is among the most frequently performed surgical procedures in general surgery and endocrine surgery clinics. The selected surgical procedure in thyroid diseases requiring surgery should allow elimination of the disease, as well as keeping postoperative complications to a minimum (1, 2).
Hypocalcemia, whether symptomatic or not, is common after thyroid surgery. It usually occurs in the first days after surgery. In some cases, exogenous replacement therapy is needed (3). Permanent hypoparathyroidism occurs in 0.5 to 2.9% of patients undergoing bilateral subtotal resection and in 0–33% of patients undergoing total thyroidectomy (4–6). In this study, the incidence of temporary and permanent hypocalcemia following total, near total and bilateral subtotal thyroidectomy performed in our clinic during the last 3 years and the relationship of hypocalcemia with surgical, clinical and biological factors of interest were analyzed retrospectively.
MATERIAL AND METHODS
In this study, data on 195 consecutive patients who underwent total, near-total or bilateral subtotal thyroidectomy in Gaziosmanpaşa Taksim Training and Research Hospital, Department of General Surgery during January 2010–January 2013 were evaluated retrospectively. Preoperatively, all patients were asked to complete consent forms. Gaziosmanpaşa Taksim Training and Research Hospital Ethics Committee approved this study (Decision Date: 02/20/2013, Decision No: 14). Data including age, sex, complaints, hyperthyroidism, serum alkaline phosphatase (ALP) and albumin levels, secondary operations, thyroidectomy type (total, bilateral subtotal, near-total), pathological diagnosis, incidental parathyroidectomy, postoperative complaints, signs and symptoms, early and late calcium values were recorded. Five patients who did not comply with the post-operative follow-up protocol, had a concomitant thyroid and parathyroid pathology, and who had hypocalcemia due to previous thyroid surgery were excluded from the study. Free T3, T4, TSH, total calcium, albumin, phosphorus, serum levels of ALP was measured in the preoperative period. The thyroid gland was evaluated by ultrasonography (additional tomography in case of retrosternal extension), by technetium-99m scintigraphy in case of hyperthyroidism, and by fine needle aspiration biopsy for clinical and/or radiological suspicion of cancer. Patients with preoperative symptoms and signs of thyrotoxicosis have been operated after reaching euthyroid state.
The surgical procedures were classified according to Kebebew and Clark classification. The complete removal of thyroid tissue was called “total thyroidectomy”, leaving less than 2 grams of thyroid tissue on one side and contralateral total lobectomy “near-total thyroidectomy”, leaving 4–8 grams of thyroid tissue on both lobes and removal of the isthmus and if present pyramidal lobe “bilateral subtotal thyroidectomy”.
Regardless of complaints, data on postoperative respiratory distress, sound quality, Chvostek, Trousseau’s signs and other possible complications were recorded; serum total calcium levels in the 24 and 48 hours of surgery, the 7th postoperative day, 1st and 3rd month examinations and TSH and calcium values were also recorded.
Postoperative calcium values less than 8 mg/dL were accepted as “biochemical hypocalcemia”, while patients describing paresthesia in the extremities and around the mouth, with Chvostek’s and Trousseau’s signs were recorded as “symptomatic hypocalcemia”. Oral calcium and vitamin D replacement therapy was started for patients with symptoms and/or serum calcium levels below 8 mg/dL and those patients requiring replacement therapy longer than six months and/or serum PTH levels below 15 pg/mL were evaluated as “permanent hypocalcemia”.
Statistical Analysis
When retrospectively evaluating the previously mentioned data obtained from 190 patients, mean, standard deviation, rate and frequency values were used for descriptive statistics. Data analysis were performed with chi-square test (or Fischer test if chi-square test conditions cannot be achieved) and logistic regression analysis test.
RESULTS
The mean age of 190 thyroidectomy patients in our series was 46.5±13 years (14–82 years). There were 162 female (85.3%) and 28 (14.7%) male patients (Table 1). Hypocalcemia was detected in 46 patients (24.21%), 37 of them (19.47%) had transient and 9 patients (4.74%) had persistent hypocalcemia (Figure 1). Forty (24.6%) out of 162 female patients, and 4 (14.2%) out of 28 male patients experienced hypocalcemia (Fig. 2, Table 1). 101 patients (53.16%) were above 50 years old, and 89 (46.84%) were under 50 years. Symptomatic hypocalcemia was present in 30 (29.7%) patients under the age of 50, and in 16 patients aged 50 and over (18%). There were no significant differences according to age groups in the development of post-operative hypocalcemia (p=0.38) (Table 1).
Table 1.
Data stratified by groups
| Hypocalcemia (n=46, 24.1%) | Temporary hypocalcemia (n=37, 19.4%) | Permanent hypocalcemia (n=9, 4.7%) | Normocalcemia (n=144) | ||
|---|---|---|---|---|---|
| Female | 42 | 35 | 7 | 120 | p=0.184 |
| Male | 40 | 2 | 2 | 24 | |
| Hyperthyroidism | 14 | 12 | 2 | 16 | p=0.002 |
| Euthyroidism | 32 | 25 | 7 | 128 | |
| Total thyroidectomy | 42 | 34 | 8 | 104 | p=0.008 |
| Near-total thyroidectomy | 3 | 2 | 1 | 13 | |
| Bilateral subtotal thyroidectomy | 1 | 1 | 0 | 27 | |
| Cervical dissection | 3 | 2 | 1 | 8 | p=0.567 |
| Central dissection | 3 | 1 | 0 | 1 | |
| No dissection | 1 | 34 | 8 | 135 | |
| Primary surgery | 42 | 33 | 9 | 128 | p=0.415 |
| Secondary surgery | 4 | 4 | 0 | 16 | |
| Benign | 33 | 25 | 8 | 106 | p=0.803 |
| Malignant | 13 | 12 | 1 | 38 | |
| Incidental two parathyroidectomy | 2 | 2 | 0 | 2 | p=0.081 |
| Incidental single parathyroidectomy | 6 | 6 | 0 | 10 | |
| No parathyroidectomy | 38 | 29 | 9 | 132 |
Figure 1.
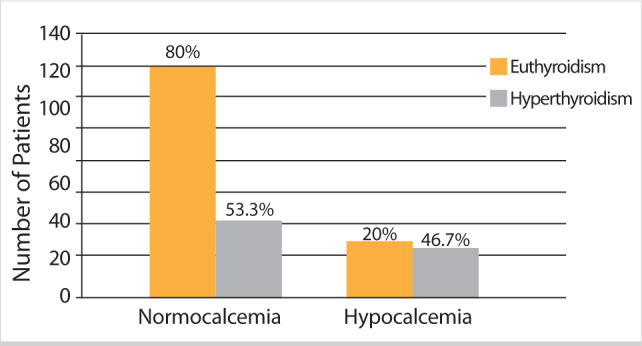
Comparison of serum calcium and thyroid hormone status
Figure 2.
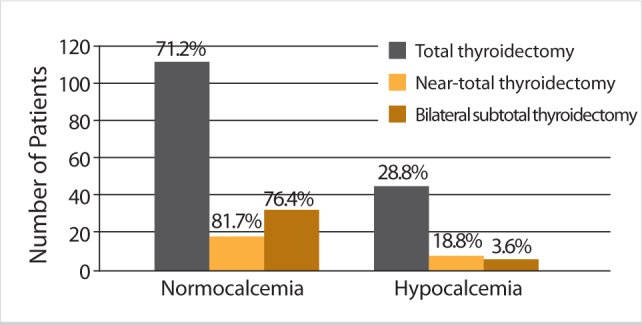
Comparison of serum calcium and surgical technique
Out of 190 thyroidectomy patients, 30 were hyperthyroid (15.8%), and 160 were euthyroid (84.2%); hypocalcemia was detected in 14 patients (46.6%) with hyperthyroidism and 32 (20%) euthyroid patients. In the group that developed early hypocalcemia, the rate of hyperthyroidism was significantly higher than the group that did not have hypocalcemia (odds ratio: 3.5) (95% CI: 1.55 to 7.91) (p=0.002). The rate of hyperthyroidism in the group that developed permanent hypocalcemia were not significantly different from both the group with transient hypocalcemia and the group that did not develop hypocalcemia (p=0.11) (Figure 1, Table 1).
One hundred-forty-six patients underwent (76.8%) total thyroidectomy, 16 (8.4%) near total thyroidectomy, and 28 (14.7%) bilateral subtotal thyroidectomy (Table 1). Early postoperative hypocalcemia was detected in one patient with bilateral subtotal thyroidectomy (3.5%), in 3 patients with near-total thyroidectomy (18.7%), and in 42 patients with total thyroidectomy (28.76%). The group with total thyroidectomy was found to be significantly different in terms of early postoperative hypocalcemia as compared to other groups (Odds ratio: 4.03) (95% CI: 1.36 to 11.99) (p=0.001). There was no significant difference between the three groups in terms of permanent hypocalcemia (Fig. 2, Table 1).
Thirteen patients (6.84%) received either central (2 patients) or modified radical (11 patients) lymph node dissection, 4 (30.8%) of those patients developed postoperative hypocalcemia, 1 of which was permanent (Table 1). The early postoperative hypocalcemia rate in the group that did not undergo lymph node dissection was 23.7%, when patients with lymph node dissection was compared to those who did not, there was no significant difference in terms of temporary or permanent hypocalcemia development (p=0.567).
One hundred sixty-seven patients (87.9%) underwent their first thyroid surgery, whereas 23 (12.1%) were operated for the second time. Eleven of these 23 patients who underwent surgery for the second time had multinodular goiter, 10 for carcinomas, 2 were operated due to recurrence of toxic multinodular goitre. Early postoperative hypocalcemia was detected in 42 of the patients who had their first thyroid surgery (25.15%), and in 4 patients (17.4%) who had been operated for the second time. Out of these 4 patients one had been operated for carcinoma, one for recurrent multi-nodular goiter, and 2 due to recurrent toxic multinodular goitre. Two out of 2 patients who were re-operated for recurrent toxic multinodular goitre developed transient hypocalcemia. When patients with primary surgery were compared to those with second surgeries, the two groups were not significantly different in terms of postoperative hypocalcemia (p=0.415) (Table 1).
According to pathology reports 139 of the patients had benign (73.2%), and 51 had malignant (26.8%) disease. Early postoperative hypocalcemia was detected in 13 patients (25.5%) with malignancy, and 33 (23.74%) patients with benign disease (Table 1). In terms of development of postoperative hypocalcemia, patients with malignant pathology and those with benign pathology did not show a significant difference between the two groups (p=0.8).
Hypocalcemia was identified in eight (40%) patients among20 (10.5%), with incidentally detected parathyroidectomy on pathology reports (Table 1). Incidental parathyroidectomy rate was 8.3% in normocalcemic patients, while this rate was 21.6% in patients with transient hypocalcemia. Incidental parathyroidectomy was not observed in any patients with permanent hypocalcemia. Incidental parathyroidectomy of two parathyroid glands was found in 4 patients, 2 (50%) of these patients had transient hypocalcemia, the rate of transient hypocalcemia was determined as 17.1% in patients without any parathyroid gland removal and a significant difference between these groups was not found due to very low number of cases (p=0.081).
DISCUSSION
Hypocalcemia following thyroid surgery is one of the main concerns for a surgeon, when severe it can lead to serious complications, with requirement of intravenous calcium replacement to relieve clinical symptoms (7).
Although in most patients hypocalcemia recovers spontaneously, permanent hypocalcemia may be seen when the parathyroid glands are permanently damaged (8–10). In untreated patients with permanent hypoparathyroidism, serious complications such as cataracts, calcification of the basal ganglia and cerebellum, and papilla edema might develop (11–13). Therefore, postoperative calcium levels should be measured. In our patients serum levels of total calcium was determined before surgery, and the first and second days after surgery, if symptoms of hypocalcemia developed in patients calcium and PTH levels were measured immediately. These patients had their calcium levels checked daily until discharge, followed by weekly measurements of calcium and phosphorus in the out-patient clinics.
In this study, postoperative transient hypocalcemia was calculated as 19.47%. Several studies report this ratio to be between 1.6% and 40% (14, 15). Rates of permanent hypocalcemia after thyroid surgery are reported to be 0.6 to 4.7% in various studies (14, 16, 17). In our study, the 4.7% rate of permanent hypocalcemia is consistent with the literature.
The mechanism of hypocalcemia after thyroidectomy is not precisely disclosed, although it is accepted to be multifactorial; factors like surgical technique, not being able to preserve the parathyroids (parathyroid injury, edema, infarction, ischemia), incidental parathyroidectomy, extent of thyroidectomy, hyperthyroidism, malignancy, secondary thyroid procedures, lymph node dissection can be considered as etiologic factors (14, 15).
Entrapment of calcium in the bones in hyperthyroidism can cause a decrease in serum calcium. When normal parathyroid function is proven, this “hungry bone syndrome” is accepted as the most likely cause of hypocalcemia (18). Wingert et al. (19) have shown that the risk of transient hypocalcemia after thyroid surgery is 20 times higher in Basedow-Graves’ disease than other diseases. In our study, 14 of 30 patients with hyperthyroidism (46.7%) developed hypocalcemia. In our series, the rate of hypocalcemia after hyperthyroidism surgery was 2.3 times higher than non-toxic goiter surgery. The presence of hyperthyroidism was detected as one of the independent factors to effect the development of postoperative hypocalcemia.
Halsted (20) first defined capsular dissection technique, and recently some authors, mainly Norman Thompson and Leigh Delbridge (21, 22), have emphasized this method. In this technique, the inferior thyroid artery is not ligated, and in order to avoid injury to the vessels of the parathyroid gland its tertiary branches are individually ligated in the thyroid capsule. Parathyroid glands are released together with their vessels on the thyroid capsule. Intraoperative trauma to the parathyroids during exposure or unnoticed removal of the parathyroid glands can disrupt parathyroid functions (23, 24).
The extent of thyroidectomy has a significant relationship with the frequency of postoperative hypoparathyroidism. In decreasing order, the incidence of hypocalcemia is in the form of total thyroidectomy, subtotal thyroidectomy and hemithyroidectomy (25). Dissection carried around the parathyroid glands, and in particular, efforts to isolate the RLN in this region can lead to venous congestion and edema. In addition, ligation of thyroid veins is among the causes of venous stasis. Venous stasis and edema, even for a while, slows down parathyroid function and may cause a temporary hypoparathyroidism continuing up to a week or more after surgery.
Erbil et al. (26) reported in a prospective clinical study that hypoparathyroidism rate in patients who underwent near-total thyroidectomy (9%) are lower than patients who underwent total thyroidectomy (26%). In this study, it is emphasized that near-total thyroidectomy may be preferable in benign thyroid diseases in order to reduce the complication of hypoparathyroidism. In our study, the extent of thyroidectomy was found as an independent risk factor for the development of early postoperative hypocalcemia. In our study, early hypocalcemia rate after total thyroidectomy was 28.76%, while it was 18.75% in near-total thyroidectomy, and was 3.6% in bilateral subtotal thyroidectomy.
In our study of 4 (30.8%) patients out of 13 who underwent lymph node dissection were found to have hypocalcemia. One of them was permanent. This ratio was 23.7% in patients without dissection. Although this finding is statistically insignificant, the small number of cases suggests that this should be confirmed by a study containing a higher number of cases.
The rate of inadvertently removed parathyroid is reported to be 5–10% (27, 28). Although a single functioning parathyroid is reported to be sufficient for maintenance of calcium balance, publications stating that at least two of the glands should be removed to result in temporary or permanent hypoparathyroidism due to incidental parathyroidectomy are also present (16, 29, 30). In our study, the rate of incidental parathyroidectomy was found to be 10.5%. Incidental parathyroidectomy rate was 8.3% in normocalcemic patients, while it was 21.6% in patients with transient hypocalcemia. Incidental parathyroidectomy was not detected in any patient who developed permanent hypocalcemia. 50% of patients (in 2 of 4 patients) with incidental parathyroidectomy of two glands developed transient hypocalcemia, whereas transient hypocalcemia was seen in 17.1% of patients without removal of any parathyroid gland. Although there was no significant difference between the groups, we believe that the small number of patients in our study has an effect on these results.
Hypoparathyroidism rates after total thyroidectomy for carcinoma ranged from 0.6% to 25% (30–32). In these patients, because the posterior capsule is also removed with the thyroid, parathyroid glands are at high risk of injury (33, 34). In our study early postoperative hypocalcemia developed in 23.7% of patients without carcinoma, and in 13 of 51 patients (25.5%) with carcinoma. Presence of carcinoma was not found as a significant factor for the development of hypocalcemia.
In various publications, the rate of hypocalcemia after secondary surgery is reported as 2 to 10 times higher than the rate after primary surgery. Lefevre et al. (17) in their studies involving 685 patients reported a transient hypocalcemia rate of 5% and a permanent hypocalcemia rate of 2.5% after secondary thyroidectomy. Chao (35) and Menegaux (36) determined a general hypoparathyroidism rate of 6.95% and 3.6% in secondary surgeries, respectively. In our study, 23 patients (12.1%) fall into this group, and 4 (17.4%) showed postoperative transient hypocalcemia. In our study, a secondary surgical intervention was not found as a significant factor for the development of hypocalcemia.
In several studies, gender is indicated as a risk factor for surgical complications. According to Thomusch et al. (37) temporary or permanent recurrent laryngeal nerve damage, and permanent or temporary hypoparathyroidism is seen more frequently in women. in our study the number of female patients was 162, while the number of male patients was 28, with a female/male ratio of approximately 6 to 1. Postoperative transient hypocalcemia was detected in 7.1% of male patient-sand in 21.6% of female patients. Although we have found that female patients experienced transient hypocalcemia approximately three times more, there was no statistical significance between gender and the development of post-operative hypocalcemia. The small number of male patients in our study is thought to be effective on this finding.
There is conflicting information in various studies regarding the effects of age in the development of postoperative hypocalcemia (15, 38–40). In our study 101 patients (53.16%) were aged over 50, and 89 (46.84%) were under 50 years of age. Thirty (29.7%) patients under the age of 50, and 16 patients aged 50 and over (18%) had symptomatic hypocalcemia. There was no significant difference between groups in terms of postoperative hypocalcemia development.
In addition to all hypocalcemia reasons mentioned above, the importance of vitamin D levels has been known for years. In patients with low vitamin D levels, calcium released from bone stock is insufficient therefore, a calcium level that might remain asymptomatic may become symptomatic (41, 42). In the clinical study conducted by Erbil et al. (40) a 500-fold, increased risk of hypocalcemia was reported in patients who underwent total thyroidectomy with a vitamin D level of below 15 ng/mL.
Study Limitation
The limited number of cases is the most important limitation of this study.
CONCLUSION
Early postoperative hypocalcemia rate was found to be significantly higher in patients who underwent surgery due to hyperthyroidism than those without. Early postoperative hypocalcemia rate was found to be significantly higher in those who had undergone total thyroidectomy, than those treated by near total and bilateral subtotal thyroidectomy. Age, gender, secondary operation, malignancy, neck dissection and incidental parathyroidectomy were found to have no statistically significant effect on hypocalcemia. In our series, temporary (19.5%) and permanent (4.7%), hypocalcemia rates are consistent with the literature.
Footnotes
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
Peer-review: Externally peer-reviewed.
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of Gaziosmanpaşa Taksim Education and Research Hospital.
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Author Contributions: Concept - D.G., D.K.; Design - D.G., F.N.K.; Supervision - M.E.; Funding - M.L.G., E.K.; Materials - A.A.İ., E.K.; Data Collection and/or Processing - E.K., D.K., M.E.; Analysis and/or Interpretation - D.G., F.N.K.; Literature Review - M.L.G., D.K., E.K.; Writer - D.G., D.K.; Critical Review - F.N.K., M.E.
REFERENCES
- 1.Bender Ö, Yüney E, Çapar H, Höbek A, Ağca B, Akat O, et al. Our total thyroidectomy experience. Endokrin Diyalog. 2004;1:15–18. [Google Scholar]
- 2.Sadler GP, Clark OH, Van Heerden JA, Farley . Thyroid and Parathyroid. In: Schwartz SI, editor. Principles of Surgery. 7th Ed. New York: Mc Graw Hill; 1999. pp. 1661–1713. [Google Scholar]
- 3.Zambudio AR, Rodríguez J, Riquelme J, Soria T, Canteras M, Parrilla P. Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann Surg. 2004;240:18–25. doi: 10.1097/01.sla.0000129357.58265.3c. http://dx.doi.org/10.1097/01.sla.0000129357.58265.3c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Usman A, Sayek İ. Parathyroids and its diaseases. In: Sayek İ, editor. Temel Cerrahi. 2. baskı. Ankara: Güneş Kitabevi; 1996. pp. 1584–1605. [Google Scholar]
- 5.Attie JN, Khafıf RA. Preservation of parathyroid glands during total thyroidectomy: improved technique utilizing microsurgery. Am J Surg. 1975;130:399–404. doi: 10.1016/0002-9610(75)90472-9. http://dx.doi.org/10.1016/0002-9610(75)90472-9. [DOI] [PubMed] [Google Scholar]
- 6.Halsted WS, Evans HM. The parathyroid glandules, their blood supply and their preservation in operation upon the thyroid gland. Ann Surg. 1907;47:489–491. doi: 10.1097/00000658-190710000-00001. http://dx.doi.org/10.1097/00000658-190710000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rebe PM, Health H. Hypocalcemic emergencies. Med Clin North Am. 1995;79:93–106. doi: 10.1016/s0025-7125(16)30086-4. [DOI] [PubMed] [Google Scholar]
- 8.Schwartz AE, Friedman EW. Preservation of the parathyroid glands in total thyroidectomy. Surg Gynecof Obster. 1987;165:327–331. [PubMed] [Google Scholar]
- 9.Olson JA, DeBenedetti MK, Baumann DS, Wells SA. Parathyroid autotransplantation during thyroidectomy: results of longterm follow-up. Ann Surg. 1996;223:472–480. doi: 10.1097/00000658-199605000-00003. http://dx.doi.org/10.1097/00000658-199605000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bellamy R, Kendall- Taylor P. ‘Unrecognized hypocalcemia diagnosed 36 years after thyroidectomy. J R Soc Med. 1995;88:690–691. doi: 10.1177/014107689508801210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Faik SA, Birken EA, Baran TD. Temporary post thyroidectomy hypocalcemia. Arch Otolaryngol Head Neck Surg. 1988;114:168–174. doi: 10.1001/archotol.1988.01860140066023. http://dx.doi.org/10.1001/archotol.1988.01860140066023. [DOI] [PubMed] [Google Scholar]
- 12.Rasmussen H. Parathyroid hormone, calcitonin and the calciferols. In: Williams RH, editor. Textbook of Endocrinology, Sthed. Philedelphia: W. B. Saunders Comp; 1974. [Google Scholar]
- 13.Debry C, Schmitt E, Senéchal G, Silisté CD, Quevauvilliers J, Renou G. Analysis of complications of thyroid surgery: recurrent paralysis et hypoparathyroidism. On a series of 588 cases. Ann Otolaryngol Chir Cervicofac. 1995;112:211–217. [PubMed] [Google Scholar]
- 14.Bergamaschi R, Becouarn G, Ronceray J, Arnaud JP. Morbidity of thyroid surgery. Am J Surg. 1998;176:71–75. doi: 10.1016/s0002-9610(98)00099-3. http://dx.doi.org/10.1016/S0002-9610(98)00099-3. [DOI] [PubMed] [Google Scholar]
- 15.Bhattacharyya N, Fried MP. Assessment of the morbidity and complications of total thyroidectomy. Arch Otolaryngol Head Neck Surg. 2002;128:389–392. doi: 10.1001/archotol.128.4.389. http://dx.doi.org/10.1001/archotol.128.4.389. [DOI] [PubMed] [Google Scholar]
- 16.Edis AJ. Prevention and management of complications associated with thyroid and paratiroid surgery. Surg Clin North Am. 1979;59:83–92. doi: 10.1016/s0039-6109(16)41735-4. [DOI] [PubMed] [Google Scholar]
- 17.Lefevre JH, Tresallet C, Leenhardt L, Jublanc C, Chigot JP, Menegaux F. Reoperative surgery for thyroid disease. Langenbecks Arch Surg. 2007;392:685–691. doi: 10.1007/s00423-007-0201-6. http://dx.doi.org/10.1007/s00423-007-0201-6. [DOI] [PubMed] [Google Scholar]
- 18.Lo CY, Lam KY. Routine parathyroid autotransplantation during thyroidectomy. Surgery. 2001;129:318. doi: 10.1067/msy.2001.111125. http://dx.doi.org/10.1067/msy.2001.111125. [DOI] [PubMed] [Google Scholar]
- 19.Wingert DJ, Friesen SR, Iliopoulos JI, Pierce GE, Thomas JH, Hermreck AS. Post-thyroidectomy hypocalcemia. Incidence and risk factors. Am J Surg. 1986;15:606–610. doi: 10.1016/0002-9610(86)90435-6. http://dx.doi.org/10.1016/0002-9610(86)90435-6. [DOI] [PubMed] [Google Scholar]
- 20.Halsted WS. The operative story of goitre: the author’s operation. Johns Hopkins Hosp Rep. 1920;19:71. [Google Scholar]
- 21.Delbridge L, Reeve TS, Khadra M, Poole AG. Total thyroidectomy: the technique of capsular dissection. Aust N Z J Surg. 1992;62:96. doi: 10.1111/j.1445-2197.1992.tb00004.x. http://dx.doi.org/10.1111/j.1445-2197.1992.tb00004.x. [DOI] [PubMed] [Google Scholar]
- 22.Thompson NW, Olsen WR, Hoffman GL. The continuing development of the technique of thyroidectomy. Surgery. 1973;73:913–927. http://dx.doi.org/10.1007/s002689900459. [PubMed] [Google Scholar]
- 23.Snell RS. Head and neck. In: Snell RS, editor. Clinical Anatomy for medical students. 4th ed. Boston: Little - Brown Comp.; 1992. pp. 717–940. Chap: 11. [Google Scholar]
- 24.Pattou F, Combemale F, Fabre S, Carnaille B, Decoulx M, Wemeau JL, et al. Hypocalcemia following thyroid surgery: incidence and prediction of outcome. World J Surg. 1998;22:718–724. doi: 10.1007/s002689900459. [DOI] [PubMed] [Google Scholar]
- 25.Faik SA. Metabolic Complications of thyroid surgery: Hypocalcemia and hypoparathyroidism; hypocalcitonemia; and hypothyroidism and hyperthyroidism. In: Faik SA, editor. Thyroid Disease, endocrinology, surgery, nuclearmedicine, and radiotherapy. 2nd ed. New York: Lippincott- Raven; [Google Scholar]
- 26.Erbil Y, Barbaros U, Salmaslioğlu A, Yanik BT, Bozbora A, Ozarmağan S. The advantage of near-total thyroidectomy to avoid postoperative hypoparathyroidism in benign multinodular goiter. Langenbecks Arch Surg. 2006;391:567–573. doi: 10.1007/s00423-006-0091-z. http://dx.doi.org/10.1007/s00423-006-0091-z. [DOI] [PubMed] [Google Scholar]
- 27.Sakorafas GH, Stafyla V, Bramis C, Kotsifopoulos N, Kolettis T, Kassaras G. Incidental parathyroidectomy during thyroid surgery: an underappreciated complication of thyroidectomy. World J Surg. 2005;29:1539–1543. doi: 10.1007/s00268-005-0032-y. http://dx.doi.org/10.1007/s00268-005-0032-y. [DOI] [PubMed] [Google Scholar]
- 28.Gourgiotis S, Moustafellos P, Dimopoulos N, Papaxoinis G, Baratsis S, Hadjiyannakis E. Inadvertent parathyroidectomy during thyroid surgery: the incidence of a complication of thyroidectomy. Langenbecks Arch Surg. 2006;391:557–560. doi: 10.1007/s00423-006-0079-8. http://dx.doi.org/10.1007/s00423-006-0079-8. [DOI] [PubMed] [Google Scholar]
- 29.Uruno T, Miyauchi A, Shimizu K, Tomoda C, Takamura Y, Ito Y, et al. A prophylactic infusion of calcium solution reduces the risk of symptomatic hypocalcemia in patients after total thyroidectomy. World J Surg. 2006;30:304–308. doi: 10.1007/s00268-005-0374-5. http://dx.doi.org/10.1007/s00268-005-0374-5. [DOI] [PubMed] [Google Scholar]
- 30.Reeve T, Thompson NW. Complications of thyroid surgery: how to avoid them, how to manage them, and observations on their possible effect on the whole patient. World J Surg. 2000;24:971–975. doi: 10.1007/s002680010160. http://dx.doi.org/10.1007/s002680010160. [DOI] [PubMed] [Google Scholar]
- 31.Miccoli P, Vitti P, Rago T, Iacconi P, Bartalena L, Bogazzi F, et al. Surgical treatment of Graves’ disease: subtotal or total thyroidectomy? Surgery. 1996;120:1020–1025. doi: 10.1016/s0039-6060(96)80049-3. http://dx.doi.org/10.1016/S0039-6060(96)80049-3. [DOI] [PubMed] [Google Scholar]
- 32.Pezzullo L, Delrio P, Losito NS, Caracò C, Mozzillo N. Post-operative complications after completion thyroidectomy for differentiated thyroid cancer. Eur J Surg Oncol. 1997;23:215–218. doi: 10.1016/s0748-7983(97)92340-4. http://dx.doi.org/10.1016/S0748-7983(97)92340-4. [DOI] [PubMed] [Google Scholar]
- 33.Michie W, Duncan T, Hamer-Hodges DW, Bewsher PD, Stowers JM, Pegg CA, et al. Mechanism of hypocalcaemia after thyroidectomy for thyrotoxicosis. Lancet. 1971;1:508–514. doi: 10.1016/s0140-6736(71)91122-6. http://dx.doi.org/10.1016/S0140-6736(71)91122-6. [DOI] [PubMed] [Google Scholar]
- 34.Testini M, Rosato L, Avenia N, Basile F, Portincasa P, Piccinni G, et al. The impact of single parathyroid gland autotransplantation during thyroid surgery on postoperative hypoparathyroidism: a multicenter study. Transplant Proc. 2007;39:225–230. doi: 10.1016/j.transproceed.2006.10.192. http://dx.doi.org/10.1016/j.transproceed.2006.10.192. [DOI] [PubMed] [Google Scholar]
- 35.Chao TC, Jeng LB, Lin JD, Chen MF. Reoperative thyroid surgery. World J Surg. 1997;21:644–647. doi: 10.1007/s002689900287. http://dx.doi.org/10.1007/s002689900287. [DOI] [PubMed] [Google Scholar]
- 36.Menegaux F, Leenhardt L, Dahman M, Schmitt G, Aurengo A, Chigot JP. Repeated thyroid surgery. Indications and results. Presse Med. 1997;26:1850–1854. [PubMed] [Google Scholar]
- 37.Thomusch O, Machens A, Sekulla C, Ukkat J, Brauckhoff M, Dralle H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. Surgery. 2003;133:180–185. doi: 10.1067/msy.2003.61. http://dx.doi.org/10.1067/msy.2003.61. [DOI] [PubMed] [Google Scholar]
- 38.Sippel RS, Ozgül O, Hartig GK, Mack EA, Chen H. Risks and consequences of incidental parathyroidectomy during thyroid resection. ANZ J Surg. 2007;77:33–36. doi: 10.1111/j.1445-2197.2006.03972.x. http://dx.doi.org/10.1111/j.1445-2197.2006.03972.x. [DOI] [PubMed] [Google Scholar]
- 39.Sosa JA, Mehta PJ, Wang TS, Boudourakis L, Roman SA. A population-based study of outcomes from thyroidectomy in aging Americans: at what cost? J Am Coll Surg. 2008;206:1097–1105. doi: 10.1016/j.jamcollsurg.2007.11.023. http://dx.doi.org/10.1016/j.jamcollsurg.2007.11.023. [DOI] [PubMed] [Google Scholar]
- 40.Erbil Y, Barbaros U, Temel B, Turkoglu U, Işsever H, Bozbora A, et al. The impact of age, vitamin D(3) level, and incidental parathyroidectomy on postoperative hypocalcemia after total or near total thyroidectomy. Am J Surg. 2009;197:439–446. doi: 10.1016/j.amjsurg.2008.01.032. http://dx.doi.org/10.1016/j.amjsurg.2008.01.032. [DOI] [PubMed] [Google Scholar]
- 41.Heaney RP, Weaver CM. Calcium and vitamin D. Endocrinol Metab Clin North Am. 2003;32:181–194. doi: 10.1016/s0889-8529(02)00063-4. http://dx.doi.org/10.1016/S0889-8529(02)00063-4. [DOI] [PubMed] [Google Scholar]
- 42.Heaney RP. Vitamin D, nutritional deficiency, and the medical paradigm. J Clin Endocrinol Metab. 2003;88:5107–5108. doi: 10.1210/jc.2003-031635. http://dx.doi.org/10.1210/jc.2003-031635. [DOI] [PubMed] [Google Scholar]