

Abstract
Objective:
This study was designed to compare the efficacy of crystallized phenol method with Limberg flap in pilonidal sinus treatment.
Material and Methods:
Patients with a diagnosis of pilonidal sinus disease treated with surgical excision + Limberg rhomboid flap technique and crystallized phenol method between 2010–2011 in the Şevket Yılmaz Training and Research Hospital, Department of General Surgery were evaluated retrospectively. Patients’ age, sex, length of hospital stay, complications and recurrence rates were evaluated.
Results:
Eighty eight percent of patients were male and mean age was 26.84±6.41 in the Limberg group, and 24.72±5.00 in the crystallized phenol group. Sinus orifice locations and nature, and duration of symptoms before surgery were similar in the two groups. Length of hospital stay in the Limberg group was 1.46±0.61 days; whereas all patients in the crystallized phenol group were discharged on the same day. Infection, hematoma, wound dehiscence, and cosmetic problems were significantly higher in the Limberg group. There was no difference between the two groups in terms of recurrence and seroma formation.
Conclusion:
The less invasive method of crystallized phenol application may be an alternative approach to rhomboid excision and Limberg flap in patients with non-complicated pilonidal sinus disease, yielding acceptable recurrence rates.
Keywords: Pilonidal sinus disease, surgery, minimally invasive, flap, crystallized phenol
INTRODUCTION
Pilonidal sinus disease (PSD) usually affects young adults and is twice more common in men than women. Its incidence throughout the whole population is reported as 6 in 100,000 (1). In recent studies, acquired factors are blamed for etiopathogenesis of the disease (2, 3). Although there are many different opinions regarding the surgical treatment of pilonidal sinus disease in the literature, the common issues are that surgery should be simple and easily applicable, that the hospital length of stay should be short, with less postoperative wound care and pain, low recurrence rates and short period to return to daily activities (4–6). That is why various surgical techniques like sinotomy, marsupialization, Karydakis, oblique primary repair and flap techniques have been applied and compared for many years (7–11).
The purpose of flap techniques is to flatten deep natal cleft and thus prevent relapse (5). Recurrence, postoperative wound dehiscence and postoperative infection has been found to be higher in primary repair as compared to Limberg flap technique. In terms of patient satisfaction, flap surgery was shown to be superior to primary repair (12, 13). In a meta-analysis, flap and oblique repair was indicated as superior to primary repair, but there was no difference between flap and oblique repair. Flap surgery was accepted as over-treatment (5). In recent years, studies advocating that primary repair can be performed with acceptable complications have been presented (14).
Phenol application is defined as a conservative method in the treatment of pilonidal sinus and is the first choice of treatment in some clinics. Phenol is a monosubstituted aromatic hydrocarbon and has acidic properties. It has antiseptic, anesthetic and potent sclerosing properties. It is in the state of white crystalline solid at room temperature, while it can shift to liquid form at higher temperatures (4, 15). In the treatment of pilonidal sinus it is used as liquid phenol or the crystallized form. We aimed to evaluate the results of patients treated with crystallized phenol and Limberg flap in our series.
MATERIAL AND METHODS
Among 164 cases surgically treated for pilonidal disease at Sevket Yilmaz Teaching and Training Hospital, Department of General Surgery between 2010 and 2011, patients in whom rhomboid excision + Limberg flap technique and crystallized phenol method had been applied were retrospectively evaluated. In order to evaluate crystallized phenol’s effect better, factors that can disrupt wound healing (recurrence, infection and complicated pilonidal sinus cases; 32 cases) were excluded from the study, leaving only uncomplicated pilonidal sinuses. Informed consent was obtained from all patients.
Among patient files who had been operated on for primary disease (72 patients who underwent Limberg flap and 60 patients who had phenol application), 50 patients were randomly selected from both groups and included in the study. Two groups were formed. The first group contained 50 cases treated by Limberg flap method and the second group included 50 cases treated with phenol crystallines. All cases were retrospectively evaluated in terms of gender and age, location of sinus pits, postoperative length of hospital stay, postoperative complications (wound dehiscence, infection, hematoma, seroma, cosmesis) and recurrence. The follow-up period was 24–30 months (mean 26 months). Evaluation of postoperative complications and recurrence as well as the cosmetic results were recorded in the outpatient follow-up. Cases which did not have outpatient follow-up and they were invited to the clinics by telephone.
Surgical procedure
Limberg flap method:
All patients were operated under spinal anesthesia in the operating room. Following rhomboid excision of pilonidal sinus, gluteal fascia incision was made and the left or right sided full-thickness flap was sutured primarily to fill the defect and a suction drain was placed.
Crystallized phenol method:
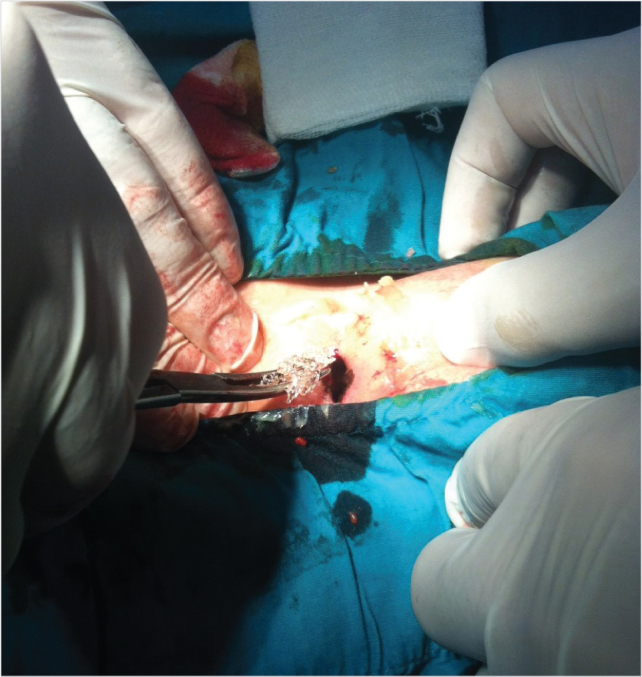
In all cases, phenol was applied under local anesthesia in the local operating room. The pit was dilated with a clamp, it was confirmed under direct vision that the sinus was not complicated and hair and debris were cleared (Figure 1, 2). The cyst epithelium was debrided (Figure 3). After protection of the pit edge with nitrofurazone ointment, crystallized phenol was filled into the sinus from the dilated sinus opening with a clamp (4, 5). The procedure was completed after dressing.
Figure 1.
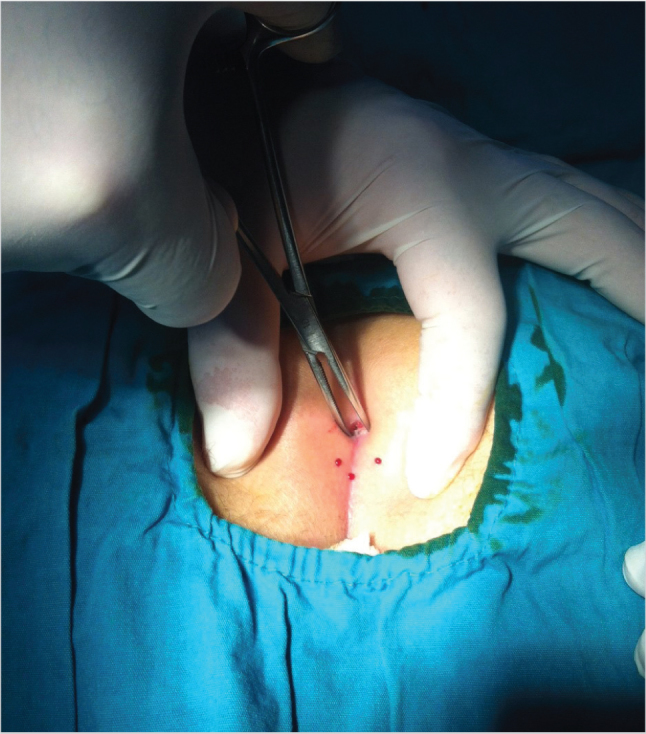
Dilatation of sinus opening with a clamp following local anesthesia
Figure 2.

Extraction of hair from the cyst
Figure 3.

Curettage of cyst epithelium
Statistical Analysis
The statistical analyzes were performed using SPSS (Statistical Package for the Social Sciences ver. 10.0, SPSS Inc, Chicago, Illinois, USA) computer program. Continuous variables were expressed as mean±standard deviation. Categorical variables were expressed as percentage (%). Parametric variables showing a normal distribution between groups were compared by Student t test and parametric variables that did not show normal distribution between groups were compared by Mann-Withney U test. Chi-square and Fisher’s exact chi-square tests were used for comparison of categorical variables. For all statistical analyzes p<0.05 was accepted as significant.
RESULTS
Eighty eight percent of the patients were male (n=46 males in Limberg group, and n=42crystallized phenol group) and the mean age of Limberg group was 26.84±6.41, and of crystalline phenol group was 24.72±5.00. There were no significant differences between the two groups in terms of age or gender (p>0.05). Similarly, there were no significant differences between the two groups in terms of location of sinus pit, presence of single or multiple pits (p>0.05). The preoperative duration of the symptoms was 12.62±10.14 months in the Limberg group and was 9.76±5.73 months in the crystallized phenol group and there was no statistically significant difference between the two groups (Table 1).
Table 1.
Demographic properties, length of complaint and hospital stay, recurrence and postoperative complications in Limberg flep and crystallized phenol treatment
| Limberg Flep | Crystallized Phenol | p value | |
|---|---|---|---|
| Gender M/F | 46/4 (92%M) | 42/8 (84%M) | 0,21 |
| Age (years) | 26,84±6,41 | 24,72±5,00 | 0,06 |
| According to location | |||
| Midline single: 14 (28%) | 19(%38) | ||
| Midline multiple: 28 (56%) | 25 (%50) | 0,54 | |
| Lateral: 8 (16%) | 6 (%12) | ||
| Duration of preoperative complaints (months) | 12,62±10,14 | 9,76±5,73 | 0,08 |
| Length of hospital stay (days) | 1,46±0,61 | 0 | <0,001 |
| Infection | 17 (%34) | 4 (%8) | 0,001 |
| Hematoma | 12 (%24) | 2 (%4) | 0,004 |
| Seroma | 3 (%6) | 0 (%0) | 0,07 |
| Wound dehiscence | 4 (%8) | 0(%0) | 0,04 |
| Cosmetic complaints | 8 (%16) | 0 (%0) | 0,003 |
| Recurrence | 4 (%8) | 6 (%12) | 0,50 |
The length of hospital stay was 1.46±0.61 days in the Limberg group whereas all cases were discharged on the same day in the crystalline phenol group (p<0.001) (Table 1).
Groups were evaluated in terms of postoperative complications. Infection, hematoma and wound dehiscence was significantly lower in the crystallized phenol group as compared to Limberg group (p<0.05), whereas in terms of seroma formation there was no significant difference between the groups (p>0.05). Wound dehiscence was observed in four patients in the first group, there were no dehiscence in the second group (p=0.04) (Table 1).
During twenty-six months of follow-up, there were 4 (8%) recurrences in the Limberg group and six (12%) recurrences in the crystallized phenol. The groups did not show a statistically significant difference in terms of recurrence (p>0.05). Cosmetically crystallized phenol group was perceived to be better (p=0.003) (Table 1).
DISCUSSION
Treatment of pilonidal sinus disease contains many different techniques from simple drainage to complicated flaps (8–10, 13). The treatment may vary with the disease condition and the surgeon’s experience. The most appropriate treatment should offer the least recurrence and postoperative complication rate with the highest patient satisfaction (13). The type of anesthesia, cost and time to return to daily life are important factors for the ideal PSD treatment (16). In a Cochrane study published in 2011 where pilonidal sinus surgery with primary intent was compared to secondary intention, secondary healing is shown to result in less recurrence than all primary repairs, with the highest recurrence being in the midline repair (primary repair). The time to return to work is shorter in all primary repairs; secondary healing requires a longer period of dressings and is therefore more costly (17). The tissue defect in phenol application is less, it can be administered under local anesthesia, and the duration of hospitalization is short, so the cost is low (4, 18). Maurice and Greenwood first described phenol treatment in 1964 (19). Liquid and crystallized phenol application has been used to treat pilonidal sinus in various studies. When applying this technique either with liquid or with crystallized phenol, the pit should be dilated and debris and hair within the sinus must be removed and granulation tissue should be debrided (4, 15, 16). It has been advocated that in crystallized phenol application the sinus pit is dilated more with better removal of hair within the sinus and thus obtaining more successful results than liquid phenol thus obtained better results have been described (20).
Aygen et al. (18) have applied crystallized phenol in 36 recurrent PSD patients who had a previous primary repair or flap procedures and reported recurrence in five (13.9%) patients during a follow-up of 54 months and out of these 2 patients responded to the same treatment, resulting in an overall success rate of 91%. Kayaalp et al. (21) have applied liquid phenol and reported a success rate of 70%. Doğru et al. (20) used repeated cycles of crystallized phenol in a series of 41 consecutive cases, and they have reported a success rate of 95.1% in 24 months follow-up. In our series, an 88% success rate has been achieved with single session application of crystallized phenol. In the literature, there are publications with a follow-up period of 1 year after surgery for pilonidal sinus, while there are also other studies indicating that the follow-up duration should be three years (5, 12). The mean follow-up period in our study was 26 months.
Flap treatment of pilonidal sinus disease, as practiced in our clinic, is mostly done under spinal anesthesia. However, in crystallized phenol application local anesthetics are used. Spinal anesthesia is a more invasive process, which has complications such as headaches and urinary retention, and it is more costly than local anesthesia; additionally it requires patient monitoring after the procedure (22). In patients who underwent crystallized phenol treatment local anesthesia was used and the patients were discharged on the same day. The mean post-operative length of hospital stay for patients with Limberg flap application was 1.40±0.61 days and this is shorter than mean duration reported in the literature (6, 15). On the other hand, the group receiving crystallized phenol was treated without hospitalization.
Recurrence was observed in 8% of patients in the Limberg group and in 12% of cases in the crystalline phenol group. This difference was not statistically significant. In terms of early complications, the rates of infection and hematoma were significantly lower in the crystallized phenol group. In the literature, especially in patients who underwent flap method, cosmetic concerns have been reported in the postoperative period (23, 24). In our study, 8 (8%) of all patients complained of an unpleasant esthetic look, they were all in the Limberg flap group.
For crystallized phenol application the pit should be dilated, the hair and debris cleaned and crystallized phenol should be inserted into the sinus with skin protection. Phenol, by some authors is applied in the form of repetitive sessions (16). In our clinics, crystallized phenol treatment is applied to patients with uncomplicated primary disease, in a single session under local anesthesia. Our study detected better cosmetic results, lower rates of infection and hematoma without significant changes in the recurrence rate by crystallized phenol treatment.
Study Limitations
Limitations of our study were its retrospective nature, relatively short follow-up period and exclusion of complicated patients. The recurrence and infection rates of crystallized phenol treatment and its results in complicated pilonidal sinus disease should be further evaluated in larger case series. In addition, these data should be re-evaluated in a larger series of patients, including additional parameters like pain scores.
CONCLUSION
The advantages of this process are the absence of any need for hospitalization, minimally invasive characteristic and quicker return to daily activities. In pilonidal sinus treatment, especially in patients with uncomplicated primary disease, we believe it would be appropriate to consider application of crystallized phenol first, reserving complicated surgical procedures for patients who do not benefit from phenol treatment.
Figure 4.

Protection of skin with nitrofurasone ointment
Figure 5.
Application of crystallized phenol into the cyst
Footnotes
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
Peer-review: Externally peer-reviewed.
Ethics Committee Approval: This study is retrospective; furthermore in that period, all the ethics committees across the country has entered a restructuring process. Thus the ethical approval has not been received.
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Author Contributions: Concept - D.T., K.A., M.P.; Design - D.T., K.A.; Supervision - D.T., U.D., F.E., M.P.; Funding - D.T., U.D., F.E.; Materials - Y.Ö.; Data Collection and/or Processing - K.A., U.D., F.E., M.P.; Analysis and/or Interpretation - D.T., Y.Ö.; Literature Review - D.T., K.A.; Writer - D.T., K.A., Y.Ö.; Critical Review - D.T., U.D., F.E., Y.Ö.
REFERENCES
- 1.McCallum IJ, King PM, Bruce J. Healing by primary closure versus open healing after surgery for pilonidal sinus: systematic review and meta-analysis. BMJ. 2008;336:868–871. doi: 10.1136/bmj.39517.808160.BE. http://dx.doi.org/10.1136/bmj.39517.808160.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Akinci OF, Bozer M, Uzunköy A, Düzgün SA, Coşkun A. Incidence and aetiological factors in pilonidal sinus among Turkish soldiers. Eur J Surg. 1999;165:339–342. doi: 10.1080/110241599750006875. http://dx.doi.org/10.1080/110241599750006875. [DOI] [PubMed] [Google Scholar]
- 3.Chintapatla S, Safarani N, Kumar S, Haboubi N. Sacrococcygeal pilonidal sinus: historical review, pathological insight and surgical options. Tech Coloproctol. 2003;7:3–8. doi: 10.1007/s101510300001. http://dx.doi.org/10.1007/s101510300001. [DOI] [PubMed] [Google Scholar]
- 4.Dag A, Colak T, Turkmenoglu O, Sozutek A, Gundogdu R. Phenol procedure for pilonidal sinus disease and risk factors for treatment failure. Surgery. 2012;151:113–117. doi: 10.1016/j.surg.2011.07.015. http://dx.doi.org/10.1016/j.surg.2011.07.015. [DOI] [PubMed] [Google Scholar]
- 5.Petersen S, Koch R, Stelzner S, Wendlandt TP, Ludwig K. Primary closure techniques in chronic pilonidal sinus: a survey of the results of different surgical approaches. Dis Colon Rectum. 2002;45:1458–1467. doi: 10.1007/s10350-004-6451-2. http://dx.doi.org/10.1007/s10350-004-6451-2. [DOI] [PubMed] [Google Scholar]
- 6.Tavassoli A, Noorshafiee S, Nazarzadeh R. Comparison of excision with primary repair versus Limberg flap. Int J Surg. 2011;9:343–346. doi: 10.1016/j.ijsu.2011.02.009. http://dx.doi.org/10.1016/j.ijsu.2011.02.009. [DOI] [PubMed] [Google Scholar]
- 7.Yalcin S, Ergul E. A single-surgeon, single-institute experience of 59 sinotomies for sacrococcygeal pilonidal disease under local anesthesia. Bratisl Lek Listy. 2010;111:284–285. [PubMed] [Google Scholar]
- 8.Karakayali F, Karagulle E, Karabulut Z, Oksuz E, Moray G, Haberal M. Unroofing and marsupialization vs. rhomboid excision and Limberg flap in pilonidal disease: a prospective, randomized, clinical trial. Dis Colon Rectum. 2009;52:496–502. doi: 10.1007/DCR.0b013e31819a3ec0. http://dx.doi.org/10.1007/DCR.0b013e31819a3ec0. [DOI] [PubMed] [Google Scholar]
- 9.Yıldız MK, Ozkan E, Odabaşı HM, Kaya B, Eriş C, Abuoğlu HH, et al. Karydakis flap procedure in patients with sacrococcygeal pilonidal sinus disease: experience of a single centre in Istanbul. ScientificWorldJournal. 2013;2013:807027. doi: 10.1155/2013/807027. http://dx.doi.org/10.1155/2013/807027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sahasrabudhe P, Panse N, Waghmare C, Waykole P. V-y advancement flap technique in resurfacing postexcisional defect in cases with pilonidal sinus disease-study of 25 cases. Indian J Surg. 2012;74:364–370. doi: 10.1007/s12262-011-0403-6. http://dx.doi.org/10.1007/s12262-011-0403-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Can MF, Sevinç MM, Hançerlioğulları O, Yılmaz M, Yağcı G. Multicenter prospective randomized trial comparing modified Limberg flap transposition and Karydakis flap reconstruction in patients with sacrococcygeal pilonidal disease. Am J Surg. 2010;200:318–327. doi: 10.1016/j.amjsurg.2009.08.042. http://dx.doi.org/10.1016/j.amjsurg.2009.08.042. [DOI] [PubMed] [Google Scholar]
- 12.Mahdy T. Surgical treatment of the pilonidal disease: primary closure or flap reconstruction after excision. Dis Colon Rectum. 2008;51:1816–1822. doi: 10.1007/s10350-008-9436-8. http://dx.doi.org/10.1007/s10350-008-9436-8. [DOI] [PubMed] [Google Scholar]
- 13.Hosam R, Yasser A, Waleed A, Ibrahim A, Mokhtar F, Mohammed F. Rhomboid flap versus primary closure after excision of sacrococcıgeal pilonidal sinus (a prospective randomized study) EJS. 2010;29:4. [Google Scholar]
- 14.Kaya B, Uctum Y, Simsek A, Kutanis R. Primary closure in the treatment of pilonidal disease. An easy and effective method. Kolon Rektum Hast Derg. 2010;20:59–65. [Google Scholar]
- 15.Gülpınar K, Pampal A, Ozis SE, Kuzu MA. Non-operative therapy for pilonidal sinus in adolescence: crystallised phenol application, “report of a case”. BMJ Case Rep. 2013;2013 doi: 10.1136/bcr-2012-008382. pii: bcr2012008382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ölmez A, Kayaalp C, Aydın C. Treatment of pilonidal disease by combination of pit excision and phenol application. Tech Coloproctol. 2013;17:201–206. doi: 10.1007/s10151-012-0903-9. http://dx.doi.org/10.1007/s10151-012-0903-9. [DOI] [PubMed] [Google Scholar]
- 17.AL-Khamis A, McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Review. 2010:CD006213. doi: 10.1002/14651858.CD006213.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Aygen E, Arslan K, Dogru O, Basbug M, Camci C. Crystallized phenol in nonoperative treatment of previously operated, recurrent pilonidal disease. Dis Colon Rectum. 2010;53:932–935. doi: 10.1007/DCR.0b013e3181d8283b. http://dx.doi.org/10.1007/DCR.0b013e3181d8283b. [DOI] [PubMed] [Google Scholar]
- 19.Maurice BA, Greenwood RK. A conservative treatment of pilonidal sinus. Br J Surg. 1964;51:510–512. doi: 10.1002/bjs.1800510711. http://dx.doi.org/10.1002/bjs.1800510711. [DOI] [PubMed] [Google Scholar]
- 20.Doğru O, Camcı C, Aygen E, Girgin M, Topuz O. Pilonidal sinus treated with crystallized phenol: an eight-year experience. Dis Colon Rectum. 2004;47:1934–1938. doi: 10.1007/s10350-004-0720-y. http://dx.doi.org/10.1007/s10350-004-0720-y. [DOI] [PubMed] [Google Scholar]
- 21.Kayaalp C, Ölmez A, Aydın C, Pişkin T, Kahraman L. Investigation of a one-time phenol application for pilonidal disease. Med Princ Pract. 2010;19:212–215. doi: 10.1159/000285291. http://dx.doi.org/10.1159/000285291. [DOI] [PubMed] [Google Scholar]
- 22.Sungurtekin H, Sungurtekin U, Erdem E. Local anesthesia and midazolam versus spinal anesthesia in ambulatory pilonidal surgery. J Clin Anesth. 2003;15:201–205. doi: 10.1016/s0952-8180(03)00032-1. http://dx.doi.org/10.1016/S0952-8180(03)00032-1. [DOI] [PubMed] [Google Scholar]
- 23.Erdem E, Sungurtekin U, Nessar M. Are postoperative drains neccessary with the Limberg flep for treatment of pilonidal sinus? Dis Colon Rectum. 1998;41:1427–1431. doi: 10.1007/BF02237061. http://dx.doi.org/10.1007/BF02237061. [DOI] [PubMed] [Google Scholar]
- 24.Eryılmaz R, Şahin M, Alimoğlu O, Dasiran F. Surgical treatment of sacrococcygeal pilonidal sinus with the Limberg transposition flep. Surgery. 2003;134:745–749. doi: 10.1016/s0039-6060(03)00163-6. http://dx.doi.org/10.1016/S0039-6060(03)00163-6. [DOI] [PubMed] [Google Scholar]