

Abstract
Cannabis is the most commonly used illicit drug worldwide. With debate surrounding the legalization and control of use, investigating its health risks has become a pressing area of research. One established association is that between cannabis use and schizophrenia, a debilitating psychiatric disorder affecting approximately 1% of the population over their lifetime. Although considerable evidence implicates cannabis use as a component cause of schizophrenia, it remains unclear whether this is entirely due to cannabis directly raising risk of psychosis, or whether the same genes that increases psychosis risk may also increase risk of cannabis use.
In a sample of 2,082 healthy individuals, we show an association between an individual’s burden of schizophrenia risk alleles and use of cannabis. This was significant both for comparing those who have ever vs. never used cannabis (p=2.6×10−4), and for quantity of use within users (p=3.0×10−3). While directly predicting only a small amount of the variance in cannabis use, these findings suggest that part of the association between schizophrenia and cannabis is due to a shared genetic aetiology. This form of gene-environment correlation is an important consideration when calculating the impact of environmental risk factors, including cannabis use.
Introduction
During the last quarter of the 20th century cannabis use has increased to become the most widely used illicit drug in the world1. It is well established that cannabis use is much higher amongst schizophrenic patients than in the general population2. Cannabis intoxication can lead to an acute transient psychotic episode and produce short-term exacerbations of pre-existing psychotic symptoms3–5, an association that has been confirmed through the experimental administration of tetrahydrocannabinol (THC)6, 7. Meta-analyses of prospective studies have found that cannabis use increases the likelihood of developing a psychotic illness by a factor of roughly two8–11. A dose response effect has been demonstrated12–14, and use in adolescence has been associated with the greatest risk15. Given the large health burden from schizophrenia and other psychotic disorders16, the view that cannabis use is a component cause of schizophrenia has heavily influenced discussion over the legislation surrounding cannabis use.
However, the relationship between schizophrenia and cannabis use may be more complicated than it initially seems. Despite a clear association between the two, the possibility of reverse causation has not been entirely excluded. Some small studies have suggested that it is in fact psychosis that is a risk factor for cannabis use, as those on a psychotic spectrum are more likely to experiment with drugs17, 18. The strongest evidence comes from Ferdinand et al. who found that the association was bidirectional, as cannabis naïve children with prodromal psychotic episodes had greater incidence of later cannabis use19. However, a similarly sized study failed to replicate this finding20. There is also possibility of attempts at self-medication, as it has been suggested that cannabis use can reduce negative and affective symptoms in patients with an established psychotic disorder21–23.
The issue is further complicated by tentative evidence for interactions between cannabis use and genetic risk variants for schizophrenia24. Schizophrenia is known to be highly heritable with up to 80% of the variance explained by additive genetic effects25, and as sample sizes have increased a growing number of genetic risk variants have been identified26, 27. Interactions between risk variants and cannabis use might explain why some individuals experience psychosis while others do not. However, cannabis use itself has been reported to be heritable28–30, though no genetic risk variants have been identified31. It is unclear to what extent the heritability of cannabis use results from shared heritability with other behavioural phenotypes such as schizophrenia predicting its use.
Here we test for such genetic overlap directly, and aim to discern the direction of causation between cannabis use and schizophrenia. Within a sample of 2,082 healthy individuals, we tested to see if polygenic risk profiles for schizophrenia predict cannabis use. Polygenic risk profiles reflect the cumulative burden of risk alleles carried by an individual as identified in a previous genome-wide association study (GWAS)32, here of 13,833 schizophrenia cases and 18,310 controls27. Such an association with cannabis use would suggest that those genetically predisposed to schizophrenia use cannabis more frequently. This would mean that the association between schizophrenia and cannabis use is not simply one of an environmental risk factor, but rather involves gene-environment correlation as individuals choose and shape their own environment based on their own innate preferences.
Materials and Methods
The data used in this study come from the Australian Twin Registry. Data were obtained from two studies in which twins and their families participated in semi-structured diagnostic telephone interviews aimed primarily at assessing psychiatric health. Informed consent was obtained from all participants.
Sample 1 consisted of 6,265 individuals aged between 23 and 39 years (mean = 29.9±2.5) interviewed between 1996 and 2000. Participants were members of the young adult cohort, a volunteer panel of twins born between 1964 and 1971. The interview was based upon a modified version of the SSAGA (Semi-Structured Assessment of the Genetics of Alcoholism33). Detailed information about the sample recruitment, the study procedure, and the measures can be found elsewhere34. Sample 2 comprised 9,688 individuals aged between 18 and 91 years (mean = 46.3±11.3) interviewed between 2001 and 2005. Participants were members of the older and younger adult cohort of Australian twin pairs (born between 1895 and 1964, and between 1964 and 1971, respectively). A subset of this sample was ascertained based on large sibship size, or having a relative with nicotine or alcohol dependence. The interview used for this sample was also based upon a modified version of the SSAGA. Further details about the sample and assessment can be found in Heath et al. (2011)35.
A subset of the participants (N=1,866; 11.7%) participated in both studies, in which case we used data from the last assessment. The combined phenotypic sample consisted of 14,087 individuals, of whom 7,172 were genotyped. In both studies, twins were asked the same items about cannabis use: 1)Did you ever use marijuana?, 2) How old were you the very first time you tried marijuana (not counting the times you took it as prescribed)?, and 3) How many times in your life have you used marijuana (don’t count times when you used a drug prescribed for you, and took the prescribed dose). Ever use was measured on a dichotomous scale (ever versus never), whereas age at initiation and frequency of use were open questions. Table 1 shows the prevalence of cannabis use for individuals included in the present study.
Table 1.
Summary statistics of sample for cannabis use traits
| Users | Non-users | |
|---|---|---|
| N | 1,011 | 1,071 |
| Mean age (SE) | 41.3 (.23) | 53.0 (.37) |
| Percentage female (%) | 46.5 | 56.0 |
| Mean age at initiation (SE) | 19. 6 (.06) | - |
| Mean number of uses over life (SE) | 62.7(4.56) | - |
Genotype data were obtained using three different Illumina single nucleotide polygmorphism (SNP) genotyping platforms (317K, HumanCNV370-Quadv3,Human CNV370v1 and Human610-Quad). Standard quality control procedures were applied as outlined previously36, including checks for ancestry outliers, Hardy–Weinberg equilibrium (p<10−6), Mendelian errors, call rate, genotypic missingness (>5%), individual missingness (>5%) and minor allele frequency (<0.01). Individuals were pruned on relatedness, removing one individual from each pair with relatedness greater than 0.05, as determined from genetic data. The final sample therefore comprised 2,082 ‘unrelated’ individuals (see Table 1 for sample details).
Polygenic risk profile scores were constructed using the p-values and log10 odds ratios from the most recent large genome-wide association study of schizophrenia, a meta-analysis of the Psychiatric Genomics Consortium’s studies with additional Swedish samples totaling 13,833 cases and 18,310 controls27. SNPs were pruned for linkage disequilibrium using p-value informed clumping in PLINK37, using a cut-off of R2 =0.25 within 200kb window. The MHC region of the genome was excluded, due to its complex linkage disequilibrium structure. After linkage disequilibrium pruning 147,830 SNPs remained. Multiple scores were generated for each individual using the PLINK --score option and based on top SNPs from the schizophrenia GWAS using varying significance thresholds (p=0.0001, 0.001, 0.01. 0.05, 0.1, 0.2, 0.3, 0.4, 0.5, and 1.0). Polygenic risk profile scores were tested for association with a binary ever vs. never used cannabis and two quantitative traits for quantity of use and age at first use, in logistic and linear regressions respectively. These analyses were corrected for the first 10 ancestry-informative principal components, genotyping platform, sex, age, age squared, and sex-by-age. Analysis was performed in STATA38.
Results
After pruning, 2,082 unrelated individuals remained in our sample with both genotype and phenotype measures. Within the sample, 1,011 individuals (48.6%) had ever used cannabis, of whom 997 had data on quantity of use. Mean number of usages of cannabis over lifetime was 62.7 (95% CI 53.8–71.6), and the mean age of initiation of use was 20.1 (95% CI 19.7–20.5). Males showed higher rates of use than females, at 53.5% compared to 43.9% (p<0.001), though no difference in age at initiation. Table 1 shows the summary statistics for the samples.
Polygenic risk scores for schizophrenia showed positive associations for ever vs. never use of cannabis across all p-value thresholds, with the strongest association for those SNPs with p-values below 0.01 in the original schizophrenia GWAS (see Figure 1, R2=0.47%, p=2.6×10−4). Significant associations were also seen in the analysis of quantity of cannabis use for 9 of the 10 SNP cut-offs, with the top association seen for those SNPs with p≤0.05 for schizophrenia (R2=0.85%, p=0.003). No association was seen with age at initiation of use, though the association with quantity of use remained significant when number of years of usage was accounted for (results not shown).
Figure 1.

Results of polygenic risk scores for schizophrenia predicting variance explained (R2) in cannabis use as both a binary trait of ever vs. never, and as a quantitative trait of lifetime usewithin only users. Polygenic scores were created using different cut-offs for the inclusion of risk variants for schizophrenia, ranging from p=0.0001 to 1.0.
As a secondary analysis, polygenic risk score for schizophrenia risk alleles with p<0.01 (the threshold with the greatest association in the primary analysis) were examined within 990 twin pairs (608 dizygotic and 382 monozygotic) where data on cannabis use of both twins was available. Taking the mean polygenic risk score within each twin pair, an ordinal regression was performed to predict whether neither (n=272), one (n=273), or both twins (n=445) were cannabis users. After correcting for age, sex, and zygosity, a significant association was observed (p=0.001). Those twin pairs where both reported using cannabis had the greatest burden of schizophrenia risk alleles, pairs with only one user were found to have an intermediate level, and the lowest burden was found in pairs where neither twin reported use (see Figure 2).
Figure 2.
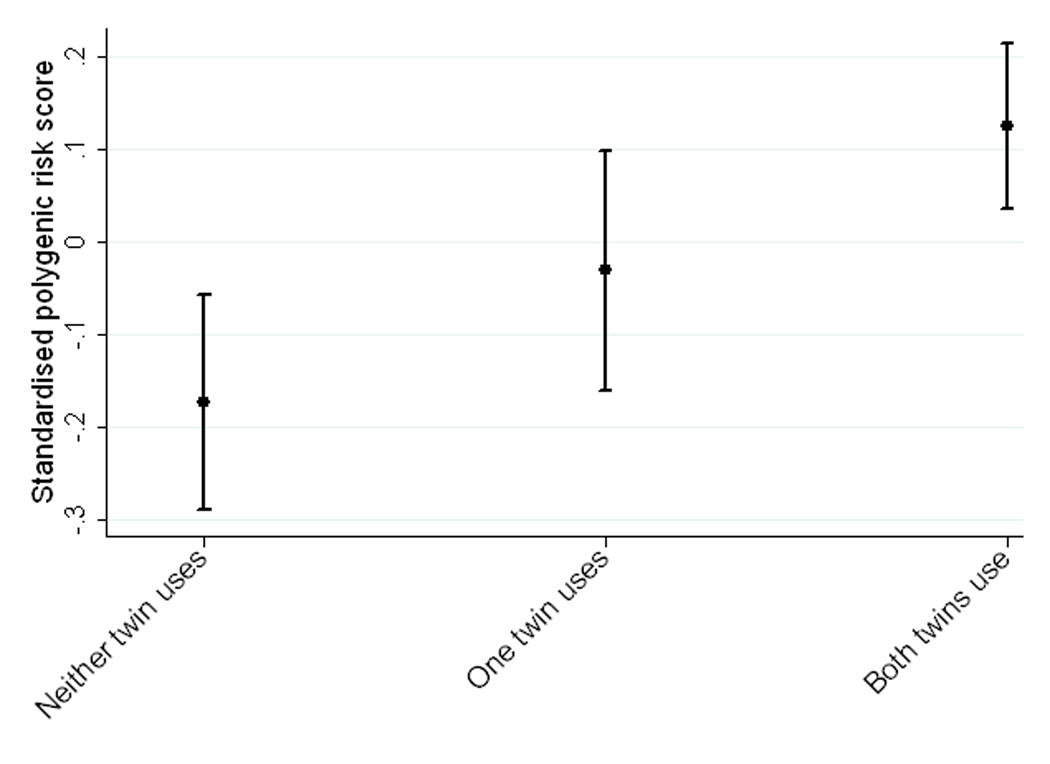
Mean standardized polygenic risk scores for pairs of twins when neither (n=272), one (n=273), or both twins (n=445) had reported use of cannabis. An ordinal regression reported a significant association (p=0.001).
Discussion
Our results show that to some extent the association between cannabis and schizophrenia is due to a shared genetic aetiology across common variants. They suggest individuals with an increased genetic predisposition to schizophrenia are both more likely to use cannabis and to use it in greater quantities. This is not to say there is no causal relationship between use of cannabis and risk of schizophrenia, but it does establish that at least part of the association may be due to causal relationship in the opposite direction. While the variance in cannabis use explained by schizophrenia polygenic risk profiles is small, it is in line with other cross-phenotype analyses, largely due to the polygenic risk scores for schizophrenia predicting only ~7% of the variation for schizophrenia itself. Previous associations between polygenic risk scores for schizophrenia and other psychiatric illnesses, such as bipolar disorder, major depression and autism39, have shown effects of similar sizes. Further research will be needed to see if the genetic overlap observed here is specific to cannabis use or is present across illicit drug use and addiction phenotypes, data for which was not widely available in this sample. For now, these findings have important implications for the current perception of cannabis use as a risk factor for schizophrenia, and other psychotic disorders.
It is important to emphasise that the implication of schizophrenia risk alleles predicting cannabis use, if true, does not rule out the possibility of cannabis independently being a risk factor for schizophrenia. A bi-directional association between cannabis use and psychosis has previously been suggested40. Further, one caveat to interpreting the direction of causation concerns the discovery sample used to identify schizophrenia risk alleles. The schizophrenia GWAS sample will likely include many more cannabis users among cases than controls. This may lead to an excess of causal SNPs associated with cannabis use, as opposed to schizophrenia itself, identified as schizophrenia risk alleles. Only if the discovery schizophrenia sample was comprised entirely of non-cannabis users could causation be inferred without any risk of confounding. This is an important consideration as to whether polygenic risk scores over-estimate individuals’ un-modifiable genetic risk by including their genetic predisposition to modifiable environmental risk factors.
These results highlight the blurring between behavioural phenotypes and environment, and have wider implications for how we perceive supposedly environmental risks for disease. Individuals select their own environments based on their innate and learned preferences, and have their environments react to their own behaviour. Further, parents pass down both genes and environment to their children. All of these can contribute to gene-environment correlation, particularly with respect to behavioural traits. Several studies have shown that supposedly environmental risk factors such as urbanicity, religiosity, and stressful life events have heritable components to them41–43. The existence of heritability for supposedly environmental risk factors does not mean they are inevitable, only that causality is more complicated to discern. Future studies will need to explore the matching of cases and controls on environmental risk variants in order to fully disentangle causation. This can be supplemented exploring the generating of polygenic risk scores for environmental risk factors, and their role in predicting disease status. The wider availability of genetic data in richly phenotyped samples should allow for the integration of genetics into an epidemiological framework, and so the discovery of gene-environment correlations where they exist.
With ongoing debate over the legalisation of cannabis and the potential health risks it poses, understanding the association between its use and schizophrenia is a priority. It has previously been suggested that, even assuming an entirely causal relationship, the required reduction in the number of cannabis users to prevent one case of schizophrenia is in the thousands44. Our findings here highlight the possibility that this association might be bidirectional in causation, and that the risks of cannabis use could be over-estimated. This is an important subtlety to consider when calculating the economic and health impact of cannabis use.
Acknowledgements
Supported by National Institutes of Health Grants AA07535, AA0758O, AA07728, AA10249, AA13320, AA13321, AA14041, AA11998, AA17688, DA012854, DA018267, DA018660, DA23668 and DA019951; by Grants from the Australian National Health and Medical Research Council (241944, 339462, 389927, 389875, 389891, 389892, 389938, 442915, 442981, 496739, 552485, 552498, 6136022, 628911, and 1047956); by Grants from the Australian Research Council (A7960034, A79906588, A79801419, DP0770096, DP0212016, and DP0343921); and by the 5th Framework Programme (FP-5) GenomEUtwin Project (QLG2-CT-2002-01254). This research was further supported by the Centre for Research Excellence on Suicide Prevention (CRESP - Australia). KJHV is supported by the Netherlands Organization for Health Research and Development, ZonMW 31160212 (NON, HEC). We thank Richard Parker, Soad Hancock, Judith Moir, Sally Rodda, Pieta-Maree Shertock, Heather Park, Jill Wood, Pam Barton, Fran Husband, Adele Somerville, Ann Eldridge, Marlene Grace, Kerrie McAloney, Lisa Bowdler, Alexandre Todorov, Steven Crooks, David Smyth, Harry Beeby, and Daniel Park. Finally, we thank the twins and their families for their participation.
Footnotes
Conflicts of Interest:
None
References
- 1.Crime UNOoDa. World Drug Report 2013. New York: United Nations; 2013. [Google Scholar]
- 2.Green B, Young R, Kavanagh D. Cannabis use and misuse prevalence among people with psychosis. Br J Psychiatry. 2005;187:306–313. doi: 10.1192/bjp.187.4.306. [DOI] [PubMed] [Google Scholar]
- 3.McGuire PK, Jones P, Harvey I, Bebbington P, Toone B, Lewis S, et al. Cannabis and acute psychosis. Schizophr Res. 1994;13(2):161–167. doi: 10.1016/0920-9964(94)90097-3. [DOI] [PubMed] [Google Scholar]
- 4.Thornicroft G. Cannabis and psychosis. Is there epidemiological evidence for an association? Br J Psychiatry. 1990;157:25–33. doi: 10.1192/bjp.157.1.25. [DOI] [PubMed] [Google Scholar]
- 5.Tien AY, Anthony JC. Epidemiological analysis of alcohol and drug use as risk factors for psychotic experiences. J Nerv Ment Dis. 1990;178(8):473–480. [PubMed] [Google Scholar]
- 6.D'Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Wu YT, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. 2004;29(8):1558–1572. doi: 10.1038/sj.npp.1300496. [DOI] [PubMed] [Google Scholar]
- 7.Morrison PD, Zois V, McKeown DA, Lee TD, Holt DW, Powell JF, et al. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. 2009;39(10):1607–1616. doi: 10.1017/S0033291709005522. [DOI] [PubMed] [Google Scholar]
- 8.van Os J, Bak M, Hanssen M, Bijl RV, de Graaf R, Verdoux H. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 2002;156(4):319–327. doi: 10.1093/aje/kwf043. [DOI] [PubMed] [Google Scholar]
- 9.Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511–2518. [PubMed] [Google Scholar]
- 10.Arseneault L, Cannon M, Witton J, Murray RM. Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry. 2004;184:110–117. doi: 10.1192/bjp.184.2.110. [DOI] [PubMed] [Google Scholar]
- 11.McGrath J, Welham J, Scott J, Varghese D, Degenhardt L, Hayatbakhsh MR, et al. Association between cannabis use and psychosis-related outcomes using sibling pair analysis in a cohort of young adults. Arch Gen Psychiatry. 2010;67(5):440–447. doi: 10.1001/archgenpsychiatry.2010.6. [DOI] [PubMed] [Google Scholar]
- 12.Zammit S, Allebeck P, Andreasson S, Lundberg I, Lewis G. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. 2002;325(7374):1199. doi: 10.1136/bmj.325.7374.1199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Henquet C, Krabbendam L, Spauwen J, Kaplan C, Lieb R, Wittchen HU, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ. 2005;330(7481):11. doi: 10.1136/bmj.38267.664086.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moore TH, Zammit S, Lingford-Hughes A, Barnes TR, Jones PB, Burke M, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319–328. doi: 10.1016/S0140-6736(07)61162-3. [DOI] [PubMed] [Google Scholar]
- 15.Arseneault L, Cannon M, Poulton R, Murray R, Caspi A, Moffitt TE. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. 2002;325(7374):1212–1213. doi: 10.1136/bmj.325.7374.1212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi: 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Addington J, Duchak V. Reasons for substance use in schizophrenia. Acta Psychiatr Scand. 1997;96(5):329–333. doi: 10.1111/j.1600-0447.1997.tb09925.x. [DOI] [PubMed] [Google Scholar]
- 18.Spencer C, Castle D, Michie PT. Motivations that maintain substance use among individuals with psychotic disorders. Schizophr Bull. 2002;28(2):233–247. doi: 10.1093/oxfordjournals.schbul.a006934. [DOI] [PubMed] [Google Scholar]
- 19.Ferdinand RF, Sondeijker F, van der Ende J, Selten JP, Huizink A, Verhulst FC. Cannabis use predicts future psychotic symptoms, and vice versa. Addiction. 2005;100(5):612–618. doi: 10.1111/j.1360-0443.2005.01070.x. [DOI] [PubMed] [Google Scholar]
- 20.Fergusson DM, Horwood LJ, Ridder EM. Tests of causal linkages between cannabis use and psychotic symptoms. Addiction. 2005;100(3):354–366. doi: 10.1111/j.1360-0443.2005.01001.x. [DOI] [PubMed] [Google Scholar]
- 21.Compton MT, Furman AC, Kaslow NJ. Lower negative symptom scores among cannabis-dependent patients with schizophrenia-spectrum disorders: preliminary evidence from an African American first-episode sample. Schizophr Res. 2004;71(1):61–64. doi: 10.1016/j.schres.2004.01.005. [DOI] [PubMed] [Google Scholar]
- 22.Peralta V, Cuesta MJ. Influence of cannabis abuse on schizophrenic psychopathology. Acta Psychiatr Scand. 1992;85(2):127–130. doi: 10.1111/j.1600-0447.1992.tb01456.x. [DOI] [PubMed] [Google Scholar]
- 23.Dixon L, Haas G, Weiden PJ, Sweeney J, Frances AJ. Drug abuse in schizophrenic patients: clinical correlates and reasons for use. Am J Psychiatry. 1991;148(2):224–230. doi: 10.1176/ajp.148.2.224. [DOI] [PubMed] [Google Scholar]
- 24.Henquet C, Di Forti M, Morrison P, Kuepper R, Murray RM. Gene-environment interplay between cannabis and psychosis. Schizophr Bull. 2008;34(6):1111–1121. doi: 10.1093/schbul/sbn108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sullivan PF, Kendler KS, Neale MC. Schizophrenia as a complex trait - Evidence from a meta-analysis of twin studies. Arch Gen Psychiat. 2003;60(12):1187–1192. doi: 10.1001/archpsyc.60.12.1187. [DOI] [PubMed] [Google Scholar]
- 26.Ripke S, Sanders AR, Kendler KS, Levinson DF, Sklar P, Holmans PA, et al. Genome-wide association study identifies five new schizophrenia loci. Nat Genet. 2011;43(10):969–976. doi: 10.1038/ng.940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ripke S, O'Dushlaine C, Chambert K, Moran JL, Kahler AK, Akterin S, et al. Genome-wide association analysis identifies 13 new risk loci for schizophrenia. Nat Genet. 2013 doi: 10.1038/ng.2742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kendler KS, Schmitt E, Aggen SH, Prescott CA. Genetic and environmental influences on alcohol, caffeine, cannabis, and nicotine use from early adolescence to middle adulthood. Arch Gen Psychiatry. 2008;65(6):674–682. doi: 10.1001/archpsyc.65.6.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Agrawal A, Lynskey MT. The genetic epidemiology of cannabis use, abuse and dependence. Addiction. 2006;101(6):801–812. doi: 10.1111/j.1360-0443.2006.01399.x. [DOI] [PubMed] [Google Scholar]
- 30.Verweij KJ, Zietsch BP, Lynskey MT, Medland SE, Neale MC, Martin NG, et al. Genetic and environmental influences on cannabis use initiation and problematic use: a meta-analysis of twin studies. Addiction. 2010;105(3):417–430. doi: 10.1111/j.1360-0443.2009.02831.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Verweij KJ, Vinkhuyzen AA, Benyamin B, Lynskey MT, Quaye L, Agrawal A, et al. The genetic aetiology of cannabis use initiation: a meta-analysis of genome-wide association studies and a SNP-based heritability estimation. Addict Biol. 2013;18(5):846–850. doi: 10.1111/j.1369-1600.2012.00478.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Purcell SM, Wray NR, Stone JL, Visscher PM, O'Donovan MC, Sullivan PF, et al. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature. 2009;460(7256):748–752. doi: 10.1038/nature08185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bucholz KK, Heath AC, Madden PA. Transitions in drinking in adolescent females: evidence from the Missouri adolescent female twin study. Alcohol Clin Exp Res. 2000;24(6):914–923. [PubMed] [Google Scholar]
- 34.Knopik VS, Heath AC, Madden PA, Bucholz KK, Slutske WS, Nelson EC, et al. Genetic effects on alcohol dependence risk: re-evaluating the importance of psychiatric and other heritable risk factors. Psychol Med. 2004;34(8):1519–1530. doi: 10.1017/s0033291704002922. [DOI] [PubMed] [Google Scholar]
- 35.Heath AC, Whitfield JB, Martin NG, Pergadia ML, Goate AM, Lind PA, et al. A quantitative-trait genome-wide association study of alcoholism risk in the community: findings and implications. Biol Psychiatry. 2011;70(6):513–518. doi: 10.1016/j.biopsych.2011.02.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Medland SE, Nyholt DR, Painter JN, McEvoy BP, McRae AF, Zhu G, et al. Common variants in the trichohyalin gene are associated with straight hair in Europeans. Am J Hum Genet. 2009;85(5):750–755. doi: 10.1016/j.ajhg.2009.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MAR, Bender D, et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81(3):559–575. doi: 10.1086/519795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.StataCorp. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP; 2011. [Google Scholar]
- 39.Smoller JW, Craddock N, Kendler K, Lee PH, Neale BM, Nurnberger JI, et al. Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet. 2013;381(9875):1371–1379. doi: 10.1016/S0140-6736(12)62129-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Foti DJ, Kotov R, Guey LT, Bromet EJ. Cannabis use and the course of schizophrenia: 10-year follow-up after first hospitalization. Am J Psychiatry. 2010;167(8):987–993. doi: 10.1176/appi.ajp.2010.09020189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Power RA, Wingenbach T, Cohen-Woods S, Uher R, Ng MY, Butler AW, et al. Estimating the heritability of reporting stressful life events captured by common genetic variants. Psychol Med. 2012:1–7. doi: 10.1017/S0033291712002589. [DOI] [PubMed] [Google Scholar]
- 42.Whitfield JB, Zhu G, Heath AC, Martin NG. Choice of residential location: chance, family influences, or genes? Twin Res Hum Genet. 2005;8(1):22–26. doi: 10.1375/1832427053435391. [DOI] [PubMed] [Google Scholar]
- 43.Winter T, Kaprio J, Viken RJ, Karvonen S, Rose RJ. Individual differences in adolescent religiosity in Finland: familial effects are modified by sex and region of residence. Twin Res. 1999;2(2):108–114. doi: 10.1375/136905299320565979. [DOI] [PubMed] [Google Scholar]
- 44.Hickman M, Vickerman P, Macleod J, Lewis G, Zammit S, Kirkbride J, et al. If cannabis caused schizophrenia--how many cannabis users may need to be prevented in order to prevent one case of schizophrenia? England and Wales calculations. Addiction. 2009;104(11):1856–1861. doi: 10.1111/j.1360-0443.2009.02736.x. [DOI] [PubMed] [Google Scholar]