

Abstract
Among aging parents (mean age = 65, N = 139) of adults with developmental disabilities, we examined the effectiveness of multiple forms of coping with caregiver burden. As expected, accommodative strategies of adapting to stress (secondary engagement), used frequently in later life, buffered the impact of caregiver burden, whereas disengagement and distraction strategies exacerbated the effects of burden on depression symptoms. Most effects were similar for mothers and fathers, and all coping strategies, including active strategies to reduce stress (primary engagement), had greater effects for the parents with co-resident children. Vulnerability to caregiver burden was greatest when the aging parents with co-resident children used disengagement and distraction coping, but those who used engagement coping were resilient.
Keywords: developmental disabilities, coping, aging parents, depression symptoms
Parents are primary sources of support and caregiving for children with developmental disabilities, and this caregiving role continues throughout the child’s life. As such, there is an emerging group of aging parents who have raised a child with a disability and now provide care and assistance to their offspring in adulthood (Seltzer, Greenberg, & Krauss, 1995). These parents retain ongoing responsibilities that can range from occasional oversight to continuing to have the child live at home and giving daily assistance with life tasks (Krauss & Seltzer, 1993). The long-term burden of caregiving places the parents at risk for poor physical and mental health as they enter old age (Seltzer, Floyd, Song, Greenberg, & Hong, 2011). Thus, coping with caregiver burden is a lifelong challenge for these parents. The purpose of the present study is to understand how the use of various strategies for coping with stress alters the effects of caregiver burden for parents in midto-late life.
Coping consists of the cognitive and behavioral strategies that are employed to manage challenging demands. When effective, they can reduce the toll taken by both acute stressors (Lazarus & Folkman, 1984) and chronic strains (Pearlin, Menaghan, Lieberman, & Mullan, 1981). When coping strategies are ineffective or inappropriate for the circumstances; however, they fail to reduce stress and might even exacerbate distress. Coping strategies are often classified into categories depending on whether the strategy is intended to change the stressor and solve the problem, or to reduce the individual’s negative emotions caused by the strain. Common labels for these classifications are problem-focused versus emotion-focused coping, or active versus passive strategies. There has been considerable debate as to the classification of strategies within these categories, and inconsistent findings about whether and under what circumstances each type of coping is relatively more effective (Conner-Smith & Flachsbart, 2007).
These inconsistencies have emerged as well in studies of coping for parents of children with disabilities. For example, Kim, Greenberg, Seltzer, and Krauss (2003) studied mothers in mid-to-later life who had a child with an intellectual disability, and classified problem-focused coping strategies to include planning and taking action along with cognitive tactics such as positive reinterpretation of the situation, while emotion-focused coping strategies included behavioral and mental disengagement as well as venting emotions. In the Kim et al. (2003) study, the use of problem-focused strategies predicted longitudinal declines in depression over 3 years, whereas the use of emotion-focused strategies predicted increases in depression over time. Alternative findings emerged in a review by Hastings and Beck (2004) of interventions designed to reduce stress for parents of children with intellectual disability. These authors considered problem-focused strategies to include activities such as the use of behavioral management and problem-solving skills, and emotion-focused coping strategies to include relaxation and obtaining respite. In contrast to the Kim et al. (2003) findings, the authors concluded that the evidence supports both forms of coping as beneficial in reducing parents’ stress. The difference in findings might be due to the different types of coping responses included in problem- and emotion-focused coping.
Another potential source of the disagreement between these reports concerns differences in the life course stage of the families studied. For aging parents of individuals with disabilities, the use and effectiveness of coping strategies need to be considered in the context of life course changes associated with aging. Notably, for older individuals, coping involves accommodating to the challenges associated with aging that cannot be readily solved. Accommodation is accomplished by shifting priorities to better match the circumstances (Brandtstädter & Renner, 1990). Instead of trying to directly change the problem, these strategies involve modifying the meaning of the problem to reduce its perceived threat (Pearlin et al., 1981). They are consistent with Folkman’s (1997) meaning-based coping, which includes positive reappraisal of the event and revising goals, along with other strategies that support positive psychological states. Accordingly, Seltzer, Greenberg, Floyd, and Hong (2004) showed that accommodative coping was relevant for parents of children with disabilities during midlife, and its use was associated with relatively low levels of depression. Because solvable problems become less common than intractable circumstances in aging (Pearlin & Skaff, 1995), it is likely that accommodative coping will be particularly important as parents of children with disabilities transition to old age.
Similarly, recent formulations about coping suggest that more refined distinctions need to be made than simply problem- and emotion-focused strategies. Notably, a hierarchical structural model of coping proposed by Conner-Smith and Flachsbart (2007) is well suited to understanding parental coping under the condition of ongoing caregiving demands. The hierarchical model is summarized in Figure 1. The authors used factor analysis and theoretical considerations to distinguish two higher-order action categories of engagement and disengagement coping, which are efforts to address the problem or avoid the problem, respectively. Engagement coping is further divided into primary and secondary engagement strategies. Primary engagement strategies are approach-oriented responses directed toward the stressor, including engaging in problem solving, implementing solutions, and staying organized and on task. Thus, primary engagement consists of activities frequently classified as problem-focused, active coping. Secondary engagement strategies are also active forms of engaging with the problem, but focus on adjusting oneself to the stressful situation to create a better fit between the self and the environment. These strategies include cognitive reframing to identify benefits or humor in the situation, and acceptance in the form of understanding and learning to live with one’s limitations (Connor-Smith & Flachsbart, 2007). Thus, secondary engagement is consistent with accommodative forms of coping.
Figure 1.

Hierarchical structural model of coping.
In contrast to both forms of engagement coping, disengagement strategies are coping activities that distance one from all aspects of the stressful environment. They are forms of escape from the stressful situation or from one’s emotions associated with the stressful circumstances, and include techniques such as withdrawal, wishful thinking, and avoidance. These strategies combine emotion-focused with passive forms of coping, and are thought to be ineffective in managing stress in the long run. Interestingly, it is not clear how another form of escape, distraction coping, fits into this framework, particularly in the context of managing chronic caregiving demands. In the short-run, distraction might be an effective means of managing negative affect if it inhibits attention to negative internal states, such as depression (Nolen-Hoeksema & Morrow, 1993) and as a result promotes the use of effective engagement coping. However, distraction might simply be another form of escape that interferes with adopting more effective ways of reducing stress.
Because the majority of research on aging parents of children with disabilities has focused on mothers only (e.g., Kim et al., 2003; Seltzer et al., 2004), there is little information about caregiver burden and coping for fathers. Among younger parents of children with disabilities, mothers are more involved in caregiving than fathers (Parks & Pilisuk, 1991), and are more vulnerable to stress and susceptible to negative psychological impacts (e.g., Gray, 2003). Differences in how women and men cope with stress generally, with men emphasizing problem-focused and women emphasizing emotion-focused strategies (Thoits, 1995), might also account for differential vulnerability to caregiver burden. However, in a sample of aging parents of children with disabilities, Essex, Seltzer, and Krauss (1999) found that mothers used more problem-focused coping than fathers, they did not use more emotion-focused coping, and the use of problem-focused versus emotion-focused coping buffered stress only for the mothers. The situation of parenting offspring with disabilities in the context of aging might have unique implications for burden and coping that need additional research attention.
The importance of effective coping for aging parents likely depends on the extent to which the parents continue to have direct responsibility for the care of their sons and daughters with disabilities. Notably, parents who have an offspring with intellectual and developmental disabilities who co-resides with them during the early years of old age report poorer functioning than parents without co-resident offspring in several domains, including social isolation, depression, and poorer health, daily functioning, and health related quality of life (Seltzer et al., 2011). If these outcomes are the consequence of the cumulative stress of parenting a child with disabilities, the ability to cope with this stress should be most critical for the parents with co-resident offspring.
The purpose of the present study is to examine the effects of different styles of coping on the relationship between caregiver burden and psychological functioning in aging parents of adult children with developmental disabilities. The study extends earlier research by considering coping by accommodation as separate from active engagement strategies and avoidant strategies. It also examines parents from a population-based study who were not recruited based on their child’s disability and, thus, lack the self-selection biases common in research on families and disabilities. To evaluate the impact of coping, we focused on depression symptoms because these symptoms tend to increase after age 60, at least for some people (Charles & Carstensen, 2010), and depression symptoms are elevated in parents raising children with disabilities, on average (Singer, 2006). We also investigate possible gender differences for mothers and fathers in experiencing caregiver burden and coping with it. We include sex as a main effect in all analyses and test whether it interacts with the coping variables in predicting depression symptoms. Furthermore, because having the child co-reside in the home might make caregiver burden and coping more salient, we examine co-resident status as a moderator of coping effects.
From the stress process model (Pearlin et al., 1981) and previous research in this area, we tested the following hypotheses:
Engagement coping, both primary and secondary, will buffer the negative effects of caregiver burden on depression symptoms.
Disengagement coping will exacerbate the negative effects of caregiver burden on depression symptoms.
Given the lack of prior research and the inconsistent speculation about the effects of distraction coping, we evaluated the effects of distraction independently of other forms of coping.
Method
Design Overview
The sample for this study was drawn from the Wisconsin Longitudinal Study (WLS), a population-based investigation that has followed a cohort of 10,317 men and women who graduated from Wisconsin high schools in 1957, and 5,823 of their siblings who were randomly selected and added to the sample in either 1975 or 1994. The WLS conducted telephone interviews and mailed surveys over 4 time points: initially in 1957 when participants were age 18, a second wave between 1975 and 1977 when participants were ages 36–38 years on average, a third wave collected between 1992 and 1994 when participants were ages 53–54 years on average, and, a fourth wave collected from 2004 to 2006 when participants were age 65–67 years on average. The present study uses data from the fourth wave when the measure of coping was first administered.
Participants
A total of 286 parents of children with developmental disabilities have been identified in the WLS. Of these, 200 parents completed an additional interview at wave 4 about the child with disabilities, and 148 of these parents also returned mailed surveys specific to this child. An additional 9 parents were missing data on either coping or depression, so the final sample for this study consists of 139 parents with complete data, 80 from the original graduate cohort and 59 from the sample of randomly selected siblings. Of the children with a disability, 63% were male and 37% were female. The parents reported that the diagnoses for the children were as follows: 44% intellectual disability, 15% cerebral palsy, 13% Down syndrome, 12% other specific developmental disability, 12% autism, and 4% brain injury. A total of 60 participants (43%) reported that the child co-resided in their homes, and among the remaining 79 participants who were not co-residents, 31% of the children lived independently, 17% were in a group living situation, 4% lived in an institution, and 4% lived with another family member. Of the 139 participants, 73 (53%) were men and 66 (47%) were women, and their mean age was 65 years (SD = 4.54). Consistent with the population of Wisconsin in the mid-20th century, all were Caucasian. The majority of participants (57%) obtained only a high school diploma, 10% obtained an associate degree, 18% obtained a bachelor’s degree, and 16% obtained a professional degree. The mean yearly family income in 2004/06 was $76,454 (SD = $77,435), and 46% of the sample reported that they were fully retired at that time. The mean Duncan’s Socioeconomic Index score for occupational status in 1992/94, when most people were still working, was 43.55 (SD = 23.19), which indicates jobs such as service workers and managers.
Procedure
Participants were identified as having a child with a developmental disability through questions asked in the 2004/06 telephone interview that was administered to all participants about each of their children. Specifically, parents were asked, “Does your child have a developmental disability, such as autism, cerebral palsy, epilepsy…?”, or intellectual disability. If so, the specific diagnosis was obtained. If the parent was uncertain about the presence of a disability or about the specific diagnosis, but indicated that the child had difficulties in school or had epilepsy or seizures, a series of follow-up questions was administered that asked about below average intelligence and ability to perform self-care. If the parent confirmed these problems, the parent was included in the sample. These participants were then given additional measures, administered in a telephone interview and mailed survey, to investigate the experiences of raising a child with a disability. The sample for the present report was restricted to only those participants who had completed all measures used in the analyses and also had contact face-to-face or by phone with their child at least once in the past year, to eliminate parents with no involvement with the child. The great majority of parents, including those who did not co-reside with the child, had at least weekly contact, and were involved in providing care for at least one activity of daily living.
Measures
Coping Orientations to Problems Experienced (COPE)
Coping was measured by an adapted version of the Coping Orientations to Problems Experienced scale (Carver, Scheier, & Weintraub, 1989). Participants were instructed to endorse a series of statements based on what they generally do when experiencing a difficult or stressful event. They responded to a series of 18 statements describing various coping strategies using a 4-point scale, where 1 = “I usually do not do this at all,” 2 = “I usually do this a little bit,” 3 = “I usually do this a medium amount,” and 4 = “I usually do this a lot.” The 18 items were assigned to the categories of coping according to the Connor-Smith and Flachsbart (2007) model. The agreement on the category assignment for two independent judges was 90%. Primary engagement coping (4 items; e.g., “I try to come up with a strategy about what to do”) and secondary engagement coping (4 items; e.g., “I look for something good in what is happening” or “I learn to live with it”) were treated as separate variables. Disengagement coping included activities that involved avoidance, denial, or wishful thinking (4 items; e.g., “I give up trying to deal with it” or “I refuse to believe that it has happened”). Distraction (2 items; e.g., “I turn to work or other activities to take my mind off of things”) was examined separately. The COPE measure has been used extensively in previous research, and scores have demonstrated adequate convergent validity with other measures of coping (Clark, Bormann, Cropanzano, & James, 1995). In the present study, the 4-item scales showed good internal consistency for brief scales, with primary engagement coping alpha = .87, secondary engagement coping alpha = .70, and disengagement coping alpha = .67, and with item-total correlations ranging between r = .35 and r = .77. The two items measuring distraction were correlated r = .35.
Depression Symptoms
Depression symptoms were measured with Radloff’s (1977) Center for Epidemiologic Studies—Depression (CES-D) Scale. Respondents reported the number of days in the past week (0–7 days) in which they experienced each of 20 depression symptoms. The reports were converted to a 4-point scale where 0 = never, 1 = 1 to 2 days, 2 = 3 to 4 days, and 3 = 5 to 7 days, so that the summed total scores matched the conventional scoring of the CES-D. A total score of 16 or higher indicates an elevated risk for clinical depression (Radloff, 1977). The CES-D has been widely used and is shown to be a reliable measure of depression for multiple samples of older adults (e.g.; Foelker & Shewchuk, 1992; Kim, et al., 2003). For the current sample, alpha = .90.
Caregiver Burden
A standardized measure of caregiver burden was administered—the Zarit Burden Scale (Zarit, Reever, & Bach-Peterson, 1980). It included one additional item about worries about future care, which is relevant to caregiving for the child with disabilities. Participants responded to 30 items (27 negative items and 3 positive items) assessing the personal strains of caregiving based on a 3-point scale ranging from 1 = “not at all” to 3 = “extremely.” Examples of items are “I feel that my son/daughter is dependent,” “I feel uncomfortable when I have friends over because of my child,” and “I feel that I don’t have enough money to support my child in addition to the rest of our expenses.” Scores for the 3 positive items were summed and subtracted from the sum of the 27 negative items. Therefore, total burden scores could range from 18 (lowest degree of burden) to 78 (highest degree of burden). The Zarit Burden Scale has demonstrated good reliability in a sample of mothers of children with disabilities, yielding alphas between .82 and .84 (Kim et al., 2003). Support for construct validity comes from a study of family caregivers (Mean age = 59.5 years) in which lower burden scores were related to a greater sense of personal efficacy (Zeiss, Gallagher-Thompson, Lovett, Rose, & McKibbin, 1999). In the present sample, the 30-item scale yielded alpha = .89.
Results
Sample Characteristics
There were no significant sex differences for background characteristics, including the respondent’s age, family income, or education, t(137) = 0.72 to 1.38, ns. Two-way Sex × Co-residence status ANOVAs with all of the study variables produced only one significant sex effect for CES-D scores, F(1, 135) = 4.10, p < .05, in which the mothers reported more depression symptoms, M = 9.53 (SD = 8.81), than did the fathers, M = 7.35 (SD = 6.24). There were no significant mean differences across the sexes on any of the other variables, including burden, primary engagement coping, secondary engagement coping, disengagement coping, and distraction, F(1, 135) = 0.01 to 2.72, all ns. There also were no mean differences on any of the variables associated with co-residence status, and no significant Sex × Co-residence interactions, F(1, 135) = 0.01 to 3.12, all ns. Overall, the caregiver burden scores ranged from 18 to 63, M = 29.7, SD = 8.47. The CES-D scores for depression symptoms ranged from 0 to 46, M = 8.38, SD = 7.62, and 14% of the participants (n = 19) had scores that exceeded the cutoff of 16, indicative of possible clinical depression.
Coping as a Moderator of Stress on Depression
The hypotheses about coping as a moderator proposed that the use of primary engagement and secondary engagement coping would buffer the effects of stress and, thus reduce the association between caregiver burden and depression, whereas disengagement coping would exacerbate the negative effects of stress on depression. The effects of distraction coping were also explored. To evaluate these effects, a multiple regression analysis was conducted with depression symptoms as the dependent variable, and burden, all four coping variables, and the Burden × Coping interactions as predictors. The main effects were entered in the regression model in the first step, along with sex of the parent and co-residence status to control for these factors. The two-way interaction terms between forms of coping and burden were entered in the second step to test for moderation.
The results of the regression analysis are summarized in Table 1. In the first step, the main effects accounted for 42% of the variance in depression symptoms, F(7, 131) = 13.57, p < .001. The regression coefficients indicated significant main effects for predicting greater depression symptoms from high levels of burden, and from the use of disengagement coping and distraction coping. There also was a nonsignificant trend in which primary engagement coping was associated with lower levels of depression symptoms (see Table 1).
Table 1.
Prediction of Depression Symptoms from Burden and Coping Strategies
| B (SE) | β | B (SE) | β | |
|---|---|---|---|---|
| Step 1 | ||||
| Constant | 6.65 (.85) | 6.59 (.85) | ||
| Sex of parent | 3.08 (1.04) | .20* | 3.18 (1.02) | .21** |
| Co-reside with child | .53 (1.05) | .04 | .07 (1.05) | .01 |
| Burden | .37 (.06) | .41*** | .39 (.06) | .44*** |
| Primary engagement coping | −.47 (.25) | −.17a | −.42 (.25) | −.16 a |
| Secondary engagement coping | −.11 (.29) | −.03 | −.06 (.28) | −.02 |
| Disengagement coping | 1.02 (.29) | .25*** | .88 (.30) | .21** |
| Distraction coping | 1.10 (.34) | .22** | .96 (.34) | .19** |
| R 2 | .42** | |||
| Step 2 | ||||
| Primary engage × Burden | −.04 (.02) | −.12 | ||
| Secondary engage × Burden | −.05 (.03) | −.15* | ||
| Disengagement × Burden | .09 (.03) | .19** | ||
| Distraction × Burden | .12 (.04) | .19** | ||
| Δ R 2 | .05* |
p < .10
p < .05,
p < .01,
p < .001.
Note. Regression weights at Step 2 are values when each interaction term is entered alone following the main effects.
At step two, there were significant interactions of burden with three of the four types of coping; secondary engagement, disengagement, and distraction (see Table 1). The interactions were explicated by examining the regression of depression symptoms on burden at each of three levels of the coping strategy, high (+1 SD), moderate (mean), and low (−1 SD). The regression lines are portrayed in Figure 2. The patterns supported the hypotheses that the use of secondary engagement coping would buffer the negative effect of burden on depression symptoms, whereas the use of disengagement would increase vulnerability. Distraction coping also was associated with vulnerability to burden. As shown in Figure 2, the relationship between burden and depression symptoms was weaker for parents who used high levels of secondary engagement coping than for those who used lower level of these strategies. In contrast, the relationship between burden and depression symptoms was stronger for parents who used high levels of disengagement coping and distraction coping compared to those who used these strategies less. Although the interaction was not significant for primary engagement coping, it showed a similar pattern to secondary engagement coping.
Figure 2.

Coping as a moderator of the effects of stress on depression symptoms.
Sex and Co-residence Effects
To examine whether these findings differed for mothers and fathers, or whether the effects of coping were more prominent when parents co-resided with their children with disabilities, we examined the occurrence of three-way interactions involving parent sex and co-residence. Because of the complexity of the models, the three-way interactions were tested in separate regression models for each type of coping, with the significance of the three-way interactions tested after accounting for all relevant main and two-way effects.
Sex differences
The three-way interaction involving parent sex was not significant for any of the hypothesized effects of primary engagement, secondary engagement, and disengagement coping, but was significant for distraction coping, Distraction × Burden × Sex ΔR2 = .02, Fchange(1, 131) = 4.60, p < .05, β = .18. The effects for mothers and fathers separately are portrayed in Figure 3. The effects of distraction coping showed similar patterns for the mothers and the fathers, but the interactions with caregiver burden were more pronounced for the mothers. As shown in Figure 3, the negative effects of distraction coping under high levels of burden were associated with very high levels of depression symptoms for the mothers in particular.
Figure 3.
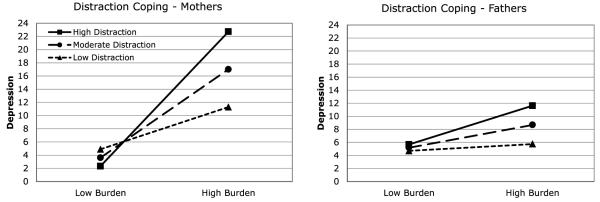
Mother/father differences in moderation by distraction coping.
Co-residence status
The three-way interactions involving co-residence status were significant for all four types of coping: Primary engagement × Burden × Co-residence ΔR2 = .03, Fchange(1, 131) = 6.59, p < .01, β = −.26, Secondary engagement × Burden × Co-residence ΔR2 = .04, Fchange(1, 131) = 7.50, p < .01, β = .33, Disengagement × Burden × Co-residence ΔR2 = .06, Fchange(1, 131) = 11.79, p < .001, β = −.36, Distraction × Burden × Co-residence ΔR2 = .02, Fchange(1, 131) = 3.75, p < .05, β = .26. The effects of co-resident status were the same in all cases; that is, the expected moderation of stress by the coping strategies was significant only for the parents who co-resided with the adult child. These findings are portrayed in Figure 4. There were clearly significant Coping × Burden (moderation) effects for the co-resident parents (β = −.35, p < .001; β = −.46, p < .001; β = .34, p < .01; β = .35, p < .01, respectively), with the frequent use of both primary and secondary engagement coping buffering the effects of high levels of burden on depression symptoms, but the frequent use of disengagement and distraction coping increasing the effects of high levels of burden on depression symptoms. In contrast, there were no moderator effects for the parents who were not co-residents (βs = −.15 to .18, NS).
Figure 4.

Co-residence as a context for coping effects.
Discussion
The results confirm the importance of effective coping in managing caregiver burden for aging parents of adults with developmental disabilities. They particularly support the usefulness of coping by accommodation, or secondary engagement coping. As hypothesized, secondary engagement coping moderated caregiver burden in a way that was consistent with buffering the impact of stress on depression symptoms. This form of coping generally involves cognitive strategies, such as reframing, which may prevent parents from engaging in the negative thought processes that are associated with depression (Connor-Smith & Flachsbart, 2007). That is, evaluating caregiver burden in ways that shift priorities, or accepting the problems as manageable, may be important ways for parents to reduce perceived threat (Pearlin et al., 1981), thus avoiding responses such as rumination, frustration, and self-blame that can exacerbate negative, depressive affect (Hollon & Dimidjian, 2009). An earlier report found that accommodative coping was an important buffer of stress in midlife (Seltzer et al., 2004); the current findings extend this coping process to the early years of old age.
In contrast, disengagement coping clearly was ineffective for these parents. The significant main effect indicated that coping by disengagement was associated with depression symptoms for the sample as a whole, and the interactions with caregiver burden and co-residence indicated that the problem is compounded for aging parents living with adult children and experiencing considerable burden. Although disengagement coping and accommodative coping are both ways of attempting to manage negative affect associated with stress, the avoidance that characterizes disengagement likely has only short-term palliative effects. That is, whereas accommodative coping can give parents new ways to think that can replace or refute depressotypic cognitions, disengagement involves simply trying to avoid or restrict negative thinking, which is rarely effective (Hollon & Dimidjian, 2009). Some coping research has suggested that disengaging from the stressor might be an effective form of coping under some circumstances, namely when the stressors are chronic and uncontrollable (Penley, Tomaka, & Wiebe, 2002). The types of disengagement examined in previous research, however, likely incorporate some of the cognitive restructuring that we classified as secondary engagement coping. Indeed, our finding is consistent with past research with similar parents indicating that disengaging, or avoiding, as a form of coping leads to adverse psychological outcomes (Seltzer et al., 1995).
Like disengagement coping, distraction also was not an effective form of coping for these parents. The findings contrast with the notion that distraction might be a temporary method of reducing emotional pain to gain a more positive outlook and greater confidence in confronting the problem in the future (Nolen-Hoeksema & Morrow, 1993). In part, the current findings might be specific to the way in which distraction was assessed in this study. That is, the two items that measured distraction coping (“turn to work or other activities to take my mind off things” and “do something to think about it less”) emphasize using distraction to avoid the problem, and do not address the issue of returning to the problem later. Also, because almost half of the participants were retired, the option of turning to work may not have been available as a way to build confidence. Future research should examine the potential benefits of distraction when used in combination with other forms of engagement coping.
Regarding active engagement coping, the current findings provide less consistent support for positive effects for these parents, though these strategies appear to be helpful under some circumstances. Primary engagement coping only reached significance as a predictor of depression symptoms for the parents with co-resident children, where it appeared to buffer the negative effects of caregiver burden on depression symptoms. Notably, the Seltzer et al. (1995) study, which had found a buffering effect for active problem-solving coping strategies for aging parents of adult children with developmental disabilities, also studied parents who had co-resident children. In this way, the results re-affirm the importance of active engagement to directly relieve caregiver stress for aging parents.
The importance of co-residence as a context for caregiver burden and coping is strongly and consistently demonstrated in the comparisons showing expected buffering effects of effective coping for the co-resident parents only. Stress process models (e.g., Pearlin et al., 1981) propose that coping in relation to a particular form of stress becomes relevant to well-being when the stressor overtaxes an individual’s resources and is perceived as a threat to well-being. Accordingly, it is likely that caregiver burden as a stressor is highly salient for aging parents who co-reside with the child with developmental disability because they must manage the strain on a daily basis. Many of these parents may engage in compound caregiving, where they also provide care to a parent or spouse, thus exacerbating their stress (Ghosh, Greenberg, & Seltzer, 2012; Perkins and Haley, 2010). The findings vividly display the vulnerability of parents with high levels of burden who do not use the two engagement forms of coping, and instead rely on disengagement and distraction. Depression symptoms for these parents approach and exceed levels that portend clinical depression. Because this level of symptomology is associated with low energy and feelings of helplessness and hopelessness (Hollon & Dimidjian, 2009), this poor functioning likely contributes to a further buildup of caregiver burden. Clearly, these are the parents who are most in need of assistance, but might be least capable of seeking and securing effective help.
In identifying the most vulnerable and most resilient parents, it is notable that the sex of the parent appeared to have little association with coping processes. The mothers did report higher levels of depression symptoms than the fathers, consistent with general trends for women and men in the population, but the lack of differences on other study variables, including burden and coping styles, and the lack of sex differences in the effects of most forms of coping, suggest that coping with caregiver burden for children with disabilities is as relevant in aging for fathers as it is for mothers. Nevertheless, the analyses did reveal one significant sex difference in the association between caregiver burden and depression symptoms, with high levels of burden associated with depression symptoms that were in the clinical range on average for mothers in particular. The burden of life-long care for a child with developmental disabilities, which is usually greater for mothers than fathers when children are younger, may undermine effective coping and make mothers particularly susceptible to low self-esteem, unhappiness, and low energy as they reach the early years of old-age. In contrast, for fathers who might have been less burdened earlier in the life course, caregiver burden later in life might be commensurate with a greater focus on family relationships at this stage, and might motivate involvement by fathers in ways that can protect them from depression symptoms. These speculations suggest that we need more information about parenting in mid- and later-life by both mothers and fathers, particularly under the circumstances of prolonged parenting responsibilities for parents of adults with disabilities.
Limitations and Future Directions
Because the sample was restricted to Caucasian participants, all of whom had graduated from high school, it is unknown whether the findings would generalize to samples that are ethnically diverse and less educated. Also, although there is empirical support for the validity of the coping questionnaire used in the current study, it likely does not capture all types of coping strategies that these parents employ when under stress. For example, it is possible that at least some parents seek emotional or tangible support as a way of coping, which was not measured here. Future research also should examine methods of coping that may boost well-being as well as reduce depression in older populations that are faced with stressful life circumstances, such as religiosity, support-seeking, or community involvement (e.g., Folkman, 1997). Knowledge of specific variables that affect the relationship between stress and well-being in older adults may allow for a better understanding of ways to enrich the lives of older parents who have been coping with the chronic stress of raising a child with a disability into adulthood.
The current study extends previous literature in the area of coping and psychological health of aging parents of children with disabilities in a few ways. First, secondary engagement coping buffers the effects of stress on depression. Second, active engagement with the stressor remains important and effective when dealing with high levels of stress even for aging parents of adult children with developmental disabilities. Third, the use of distraction as a coping strategy has effects similar to disengagement strategies, at least in the long run, which exacerbate the negative effects of stress on depression symptoms. Also, although perceived child-related burden does not necessarily vary as a function of whether the parent co-resides with the child with a disability, co-residence is associated with greater vulnerability to this stress when coping is poor. Thus, there is a need to better understand how the meaning of child-related burden changes in different living circumstances.
Acknowledgments
This research is funded by National Institutes of Health grants P01 AG021079 and P30 HD03352.
Contributor Information
Vivian E. Piazza, Georgia State University
Frank J. Floyd, University of Hawaii at Manoa, Psychology, 2530 Dole St. Sakamaki C-400, Honolulu, HI 96822-2294, USA
Marsha R. Mailick, University of Wisconsin–Madison
Jan S. Greenberg, University of Wisconsin–Madison
References
- Brandtstadter J, Renner G. Tenacious goal pursuit and flexible goal adjustment: Explication and age-related analysis of assimilative and accommodative strategies of coping. Psychology and Aging. 1990;5(1):58–67. doi: 10.1037//0882-7974.5.1.58. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology. 1989;56(2):267–283. doi: 10.1037//0022-3514.56.2.267. [DOI] [PubMed] [Google Scholar]
- Charles ST, Carstensen LL. Social and emotional aging. Annual Review of Psychology. 2009;61:383–409. doi: 10.1146/annurev.psych.093008.100448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark KK, Bormann CA, Cropanzano RS, James K. Validation evidence for three coping measures. Journal of Personality Assessment. 1995;65(3):434–455. doi: 10.1207/s15327752jpa6503_5. [DOI] [PubMed] [Google Scholar]
- Connor-Smith JK, Flachsbart C. Relations between personality and coping: A meta-analysis. Journal of Personality and Social Psychology. 2007;93:1080–1107. doi: 10.1037/0022-3514.93.6.1080. [DOI] [PubMed] [Google Scholar]
- Essex EL, Seltzer MM, Krauss MW. Differences in coping effectiveness and well-being among aging mothers and fathers of adults with mental retardation. American Journal of Mental Retardation. 1999;104:545–563. doi: 10.1352/0895-8017(1999)104<0545:DICEAW>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Foelker GA, Shewchuk RM. Somatic complaints and the CES-D. Journal of the American Geriatrics Society. 1992;40(3):259–262. doi: 10.1111/j.1532-5415.1992.tb02079.x. [DOI] [PubMed] [Google Scholar]
- Folkman S. Positive psychological states and coping with severe stress. Social Science and Medicine. 1997;45:1207–1221. doi: 10.1016/s0277-9536(97)00040-3. [DOI] [PubMed] [Google Scholar]
- Ghosh S, Greenberg JS, Seltzer MM. Adaptation to a spouse’s disability by parents of adult children with mental illness or developmental disability. Psychiatric Services. 2012;63:1118–1124. doi: 10.1176/appi.ps.201200014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray DE. Gender and coping: The parents of children with high functioning autism. Social Science & Medicine. 2003;56(3):631–642. doi: 10.1016/s0277-9536(02)00059-x. [DOI] [PubMed] [Google Scholar]
- Hastings R, Beck AT. Practitioner review: Stress intervention for parents of children with intellectual disabilities. Journal of Child Psychology and Psychiatry. 2004;45:1338–1349. doi: 10.1111/j.1469-7610.2004.00841.x. [DOI] [PubMed] [Google Scholar]
- Hollon SD, Dimidjian S. Cognitive and behavioral treatment of depression. In: Gotlib IH, Hammen CL, editors. Handbook of depression. 2nd ed Guilford Press; New York, NY: 2009. pp. 586–603. [Google Scholar]
- Kim HW, Greenberg JS, Seltzer MM, Krauss MW. The role of coping in maintaining the psychological well-being of mothers of adults with intellectual disability and mental illness. Journal of Intellectual Disability Research. 2003;47:313–327. doi: 10.1046/j.1365-2788.2003.00493.x. [DOI] [PubMed] [Google Scholar]
- Krauss MW, Seltzer MM. Current well-being and future plans of older caregiving mothers. Irish Journal of Psychology. 1993;14:47–64. [Google Scholar]
- Lazarus RS, Folkman S. Stress, appraisal, and coping. Springer; New York: 1984. [Google Scholar]
- Mazure CM. Life stressors as risk factors in depression. Clinical Psychology: Science and Practice. 1998;5:291–313. [Google Scholar]
- Nolen-Hoeksema S, Morrow J. Effects of rumination and distraction on naturally occurring depressed mood. Cognition and Emotion. 1993;7(6):561–570. [Google Scholar]
- Parks SH, Pilisuk M. Caregiver burden: Gender and the psychological costs of caregiving. American Journal of Orthopsychiatry. 1991;61:501–509. doi: 10.1037/h0079290. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Menaghan E, Lieberman M, Mullan JT. The stress process. Journal of Health and Social Behavior. 1981;22:337–356. [PubMed] [Google Scholar]
- Pearlin LI, Skaff MM. Stressors and adaptation in late life. In: Gatz M, editor. Emerging issues in mental health and aging. American Psychological Association; Washington, DC: 1995. pp. 97–123. [Google Scholar]
- Penley JA, Tomaka J, Wiebe JS. The association of coping to physical and psychological health outcomes: A meta-analytic review. Hournal of Behavioral Medicine. 2002;25:551–603. doi: 10.1023/a:1020641400589. [DOI] [PubMed] [Google Scholar]
- Perkins EA, Haley WE. Compound caregiving: when lifelong caregivers undertake additional caregiving roles. Rehabilitation Psychology. 2010;55:409–417. doi: 10.1037/a0021521. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1(3):385–401. [Google Scholar]
- Seltzer MM, Floyd FJ, Song J, Greenberg JS, Hong J. Midlife and aging parents of adults with intellectual and developmental disabilities: Impacts of lifelong parenting. American Journal on Intellectual and Developmental Disabilities. 2011;116:479–499. doi: 10.1352/1944-7558-116.6.479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seltzer MM, Greenberg JS, Floyd FJ, Hong J. Accommodative coping and well-being of midlife parents of children with mental health problems or developmental disabilities. American Journal of Orthopsychiatry. 2004;74:187–195. doi: 10.1037/0002-9432.74.2.187. [DOI] [PubMed] [Google Scholar]
- Seltzer MM, Greenberg JS, Krauss MW. A comparison of coping strategies of aging mothers of adults with mental illness or mental retardation. Psychology and Aging. 1995;10:64–75. doi: 10.1037//0882-7974.10.1.64. [DOI] [PubMed] [Google Scholar]
- Singer GHS. Meta-analysis of comparative studies of depression in mothers of children with and without developmental disabilities. American Journal on Mental Retardation. 2006;111(3):155–169. doi: 10.1352/0895-8017(2006)111[155:MOCSOD]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Thoits PA. Identity-relevant events and psychological symptoms: A cautionary tale. Journal of Health and Social Behavior. 1995;36:72–82. [PubMed] [Google Scholar]
- Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist. 1980;20:649–655. doi: 10.1093/geront/20.6.649. [DOI] [PubMed] [Google Scholar]
- Zeiss A, Gallagher-Thompson D, Lovett S, Rose J, McKibbin C. Self-efficacy as a mediator of caregiver coping: Development and testing of an assessment model. Journal of Clinical Geropsychology. 1999;5(3):221–230. [Google Scholar]