

Abstract
Background
Despite the global significance of betel quid chewing and the associated health risks, there have been no studies assessing chewers' intention to quit. Given the difficulties associated with quitting betel quid and the serious health consequences of chewing, it is important for researchers to develop interventions aimed at helping chewers quit. Betel quid chewers experience similar patterns of dependence and withdrawal symptoms as tobacco smokers, and the use of both substances causes serious adverse health effects. Therefore, it is possible that intention to quit betel quid and tobacco would also be similar. If similarities were found, researchers could look to existing tobacco cessation interventions to inform the development of betel quid cessation interventions. In the current study we sought to understand chewers' intention to quit and how it compares to smokers' intention to quit cigarettes.
Methods
A total of 351 adult betel quid chewers from Guam were compared against 1,555 adult tobacco users from Hawaii. These comparisons were made possible because of the deliberate use of identical questionnaire items (mutatis mutandis) for betel quid chewing and cigarette smoking.
Results
Smokers reported higher levels of wanting to quit, intending to quit, and wishing they have never started in the first place compared to chewers (p's < .0001). There were no differences across groups with regard to having a plan for how to quit and when to quit, with half of the samples reporting not having a plan for how or when to quit.
Conclusion
Both smokers and chewers want to quit and intend to quit, but do not have plans of when or how to quit. A deeper understanding of chewers' intention to quit and its similarities to smokers' intention to quit could be used to inform the development of betel quid cessation interventions.
Keywords: Areca nut, betel quid, intention to quit, betel nut, tobacco
Introduction
Betel quid is the fourth most commonly consumed psychoactive substance worldwide after alcohol, nicotine and caffeine [1, 2]. It is chewed by at least 10% of the world's population (600 million people)[3]. Chewed mainly in South Asia, Southeast Asia, and the Pacific islands, betel quid has long played an important cultural role, particularly with religious ceremonies. Most commonly, betel quid refers to the combination of areca nut (the seed of the palmaceous Areca catechu tree), piper betel leaf (a common vine), slaked lime (calcium hydroxide), and tobacco, though the combination of ingredients differ by region, country, ethnicity, and personal preference [4, 5]. In Guam, the term “betel nut” informally refers to the areca nut, however, it can also refer to the areca nut chewed alone or as a betel quid including piper betel leaf, slaked lime, tobacco, and other ingredients such as spices (e.g., clove). In the current study, we use the term “betel quid” to refer to any preparation of chewed areca nut, including the nut alone and all admixtures involving betel leaf, slaked lime, tobacco, and other ingredients.
Chewing betel quid is associated with a number of health issues, including oral cancer and precancerous conditions such as leukoplakia and oral submucous fibrosis [6]. Betel quid is now classifed as a Group 1 carcinogen by the International Agency for Research on Cancer [7, 8]. Despite the prevalence of betel quid chewing and the serious health risks betel quid poses to chewers, research on betel quid has been limited to epidemiological and biological investigations [9, 10]. Similar to tobacco, betel quid has been associated with both stimulant and anxiolytic effects which has been linked to esclation of use and dependency [11-15]. Although betel quid usage is often confounded by concurrent tobacco use [8, 16, 17], betel quid users have also reported experiencing withdrawal symptoms that are similar to nicotine withdrawal [11]. Given the difficulties associated with quitting betel quid and the serious health conquences of chewing, it is important for resarchers to develop interventions aimed at helping chewers quit. We are not aware of any betel quid cessation interventions published in the literature. However, before these interventions can be developed, research on the psychological orientation towards quitting betel quid needs to be expanded [16].
Most health behavior theories, particularly expectancy-value theories, posit that intention is critical to changing behavior. Researchers have found that intention to quit smoking is a critical component for successful cessation [18], and it is often addressed in smoking cessation interventions. Given the similar patterns of dependence and withdrawal symptoms experienced by betel quid chewers and smokers, and the adverse health effects associated with both substances, it is possible that intention to quit would also be similar. If similarities were found, researchers could look to existing tobacco cessation interventions to inform the development of betel quid cessation interventions.
In the current study, we compare intention to quit among two adult samples: betel quid chewers in Guam and tobacco smokers in Hawaii. Using identical measures, we assess differences in intention to quit, and whether intention to quit is associated with use, dependence, and quit attempt measures. We predicted that betel quid and tobacco users would have similar distributions of intention to quit, although the precise degree of intention would differ between the two types of users. Because betel quid chewing is a socially accepted habit and the health risks associated with chewing are less widely known, we hypothesized that smokers would endorse higher levels of intention to quit. We further hypothesized that higher levels of intention to quit among smokers and chewers would be associated with more quit attempts and lower levels of use and dependence.
Methods
Participants and Procedure
Sample of Chewers
Participants were recruited via newspaper advertisements, flyers, and community events in Guam. To determine chewing status, potential participants were asked a series of questions at the initial screening. For the current study, participants were eligible to participate if they: (a) were 18 years or older, (b) read English, (c) self-identified as chewers, and (d) reported areca nut and betel quit chewing within the past 7 days. Informed consent was obtained prior to participation in the study. Surveys were distributed through the mail and in person at community events in Guam, along with a stamped and addressed return envelope. Upon receipt of completed questionnaires, participants were mailed $25 in gift cards. The research protocol for this study followed the human subject protection protocol approved by the University of Hawaii at Manoa Institutional Review Board.
Sample of Smokers
Adult participants were recruited from the community through local newspaper advertisements in Hawaii as part of a larger intervention study. Smokers were eligible to participate if they: (a) were 18 years or older, (b) read English, (c) had mailing addresses, (d) were self-identified as smokers of at least three cigarettes per day, (e) smoked at least 100 cigarettes in their lifetime, and (f) were residents of the state of Hawaii. Smokers who met all three of the following criteria at the time of the initial screening were not eligible to participate: (a) had a quit attempt lasting 24 hours or longer within the past year, (b) were planning to quit smoking in the next 30 days, and (c) were trying to quit “right now.” These exclusion criteria were theoretically relevant to the larger intervention study. Prior to participation in the study, informed consent was obtained. Surveys were distributed through the mail along with a stamped and addressed return envelope. Following receipt of completed questionnaires, participants were mailed $25 in gift cards. The research protocol for this study followed the human subject protection protocol approved by the University of Hawaii at Manoa Institutional Review Board.
Measures
Interest and intention to quit or cut down
Five items were employed: (a) “Do you want to quit (smoking/chewing betel nut or betel quid)?” (b) “Do you intend to quit (smoking/chewing betel nut or betel quid)?” (c) “Do you have a plan for how to quit (smoking/chewing betel nut or betel quid)?” (d) “Do you wish you had never started (smoking/chewing betel nut or betel quid) in the first place?” (e) Do you have a plan for when you will stop (smoking/chewing betel nut or betel quid)?” Response options for these five items were: “(1) No, definitely not,” “(2) No, probably not,” “(3) Don't know/undecided,” “(4) Yes, probably,” and “(5) Yes, definitely.”
Use variables
Participants were asked to report their mean daily use rate, the number of years used, and the number of times they have made a 24-hour or longer quit attempt in their lifetime. Response options were open-ended. Participants were asked if they smoked or chewed daily. Response options were dichotomous (0 = No, 1 = Yes).
Dependence Scales
The Fagerstrom Test for Nicotine Dependence [19] was employed as a measure of nicotine dependence among smokers. The Betel Quid Dependence Scale (BQDS) [20, 21] was used as a measure of betel quid dependence among chewers. The BQDS is a 16-item scale designed to match the diagnostic criteria of Substance Dependence in DSM-IV [22]. Items included a dichotomous outcome (0 = No to 1 = Yes). The total score ranged from 0 to 16. Both dependence scales were coded to range from zero to one so that each score represented the proportion of items endorsed (e.g., a score of .50 would mean that half of items were endorsed), which allowed for comparisons across measures.
Analyses
To compare differences in intention to quit across the two samples, we used frequency and central tendency (mean/standard deviation) calculations. T-tests were used to assess mean differences in intention to quit across the two samples. To assess whether intention to quit was associated with use, dependence, and quit attempt measures, a series of linear regression analyses were run separately within each sample with intention to quit as the independent variable. Models controlled for age, gender, education, and ethnicity. All analyses were conducted in SAS 9.3 [23]. Statistical tests were two-tailed, significance was set at P<.05.
Results
Demographic and areca/tobacco use history
Table 1 provides demographic characteristics of the samples. A total of 351 adult betel quid chewers were included in the analyses. The mean age of the sample was 35.6 years old (SD = 20.9); 50.1% of the sample was male. The ethnic distribution of the sample was as follows: 34.5% Chamorro, 27.9% Chuukese, 21.7% Palauan, 6.6% Yapese, and 9.3 other (including Carolinian, Filipino, Marshallese, Pohnpeian, Hawaiian, African-American, and English). Participants reported chewing for an average of 15.3 years (SD = 12.8) and 11.9 times per day (SD = 13.7), and reported making an average of 5.2 (SD = 15.6) lifetime quit attempts. Three-quarters (75.3%) reported chewing every day, and participants scored an average of 0.51 (SD = 0.32) on the Betel Quid Dependence Scale.
Table 1. Descriptive statistics.
| Smokers | Chewers | |
|---|---|---|
| (N = 1555) | (N = 351) | |
| Age (years) | 45.2 (13.2) | 35.6 (20.9) |
| Male | 50.0 | 50.1 |
| U.S. Ethnicity | ||
| Asian | 21.2 | -- |
| Hawaiian | 30.9 | -- |
| White | 34.2 | -- |
| African American | 6.8 | -- |
| Other | 7.0 | -- |
| Guam Ethnicity | ||
| Chamorro | -- | 34.5 |
| Chuukese | -- | 27.9 |
| Palauan | -- | 21.7 |
| Yapese | -- | 6.6 |
| Other | -- | 9.3 |
| High school diploma | 89.9 | 59.3 |
| Number of years used | 26.6 (13.4) | 15.3 (12.8) |
| Use everyday | 97.2 | 75.3 |
| Number of use per day | 18.3 (11.2) | 11.9 (13.7) |
| Lifetime quit attempts | 11.5 (48.2) | 5.2 (15.6) |
| Dependence scale | 0.50 (0.24) | 0.51 (0.32) |
Notes. Values are frequencies or means (standard deviations).
A total of 1,555 adult tobacco users were included in the analyses. The mean age of the sample was 45.2 years old (SD = 13.2); 50.0% of the sample was male. The ethnic distribution of the sample was as follows: 21.2% Asian, 30.9% Hawaiian, 34.2% White, 6.8% African American, and 7.0 other (including Micronesian, Hispanic, American Indian, Indian, etc.). Participants reported smoking for an average of 26.6 years (SD = 13.4) and 18.3 times per day (SD = 11.2), and reported making an average 11.5 (SD = 48.2) lifetime quit attempts. Most (97.2%) reported smoking every day, and participants scored an average of 0.50 (SD = 0.24) on the Fagerstron Test for Nicotine Dependence.
Comparison of intention to quit across chewers and smokers
Table 2 presents results of the comparisons of intention to quit items across the two groups. Smokers reported higher mean levels of wanting to quit, intending to quit, and wishing they have never started in the first place compared to chewers (p's < .0001). There were no significant differences across groups with regard to having a plan for how to quit and when to quit, with half of the samples reporting not having a plan for how or when to quit. Similar levels of chewers and smokers reported they definitely want to quit (34.4% and 28.0% respectively) and intend to quit (27.7% and 29.4% respectively), although there were many more “don't know or undecided” chewers than smokers on these two items. Two-thirds (66.2%) of smokers reported that they definitely wish they have never started smoking in the first place, compared to 40.0% of chewers, while a fifth (20.8%) of chewers reported that they definitely did not wish they had never started in the first place compared to 8.18% of smokers. Figure 1 displays the percentages of the responses to the intention to quit items across the two groups.
Table 2. Responses (as Percentages) to Motivation to Quit Questionnaire Items for Chewers and Smokers.
| Question | No, definitely not | No, probably not | Don't know/undecided | Yes, probably | Yes, definitely | M (SD) | P-value a |
|---|---|---|---|---|---|---|---|
| Do you want to quit? | |||||||
| Smoking cigarettes | 11.25 | 9.58 | 15.49 | 29.31 | 34.38 | 3.66 (1.33) | <.0001 |
| Chewing betel nut | 15.43 | 14.00 | 26.57 | 16.00 | 28.00 | 3.27 (1.40) | |
| Do you intend to quit? | |||||||
| Smoking cigarettes | 9.47 | 9.41 | 15.91 | 35.82 | 29.38 | 3.66 (1.25) | <.0001 |
| Chewing betel nut | 13.43 | 16.00 | 24.57 | 18.29 | 27.71 | 3.31 (1.38) | |
| Do you have a plan for how to quit? | |||||||
| Smoking cigarettes | 33.16 | 21.25 | 21.76 | 14.23 | 9.59 | 2.46 (1.33) | .63 |
| Chewing betel nut | 37.36 | 19.54 | 19.83 | 10.06 | 13.22 | 2.42 (1.41) | |
| Do you wish that you had never started in the first place? | |||||||
| Smoking cigarettes | 8.18 | 5.22 | 7.54 | 12.89 | 66.17 | 4.24 (1.28) | <.0001 |
| Chewing betel nut | 20.80 | 12.82 | 12.54 | 13.96 | 39.89 | 3.39 (1.60) | |
| Do you have a specific plan about when to quit? | |||||||
| Smoking cigarettes | 32.19 | 19.42 | 29.29 | 10.97 | 8.13 | 2.43 (1.26) | .06 |
| Chewing betel nut | 36.60 | 13.26 | 23.34 | 6.92 | 19.88 | 2.60 (1.52) |
Note. Questionnaire items have been abridged to conserve space.
T-tests were used to assess mean differences in motivation to quit across the two samples.
Figure 1.
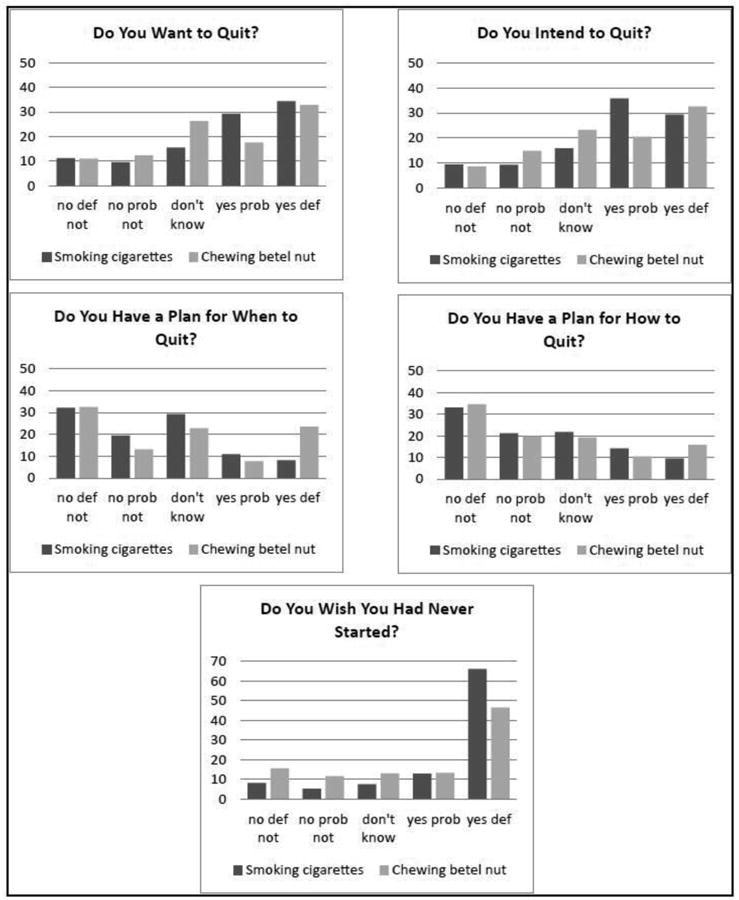
Responses (in percentages) to four measures of motivation to quit for the samples.
no def not = “No, definitely not” response;
no prob not = “N′, probably not” response;
don't know = “Don't know/undecided” response;
yes prob = “Yes, probably” response;
yes def = “Yes, definitely” response
Correlates of intention to quit across chewers and smokers
Results of the multiple linear regressions are shown in Table 3. For both chewers and smokers, number of years used was negatively associated with intention to quit, and number of lifetime quit attempts made was positively associated with intention to quit (p's < .01). Number of times used per day and level of dependence were both negatively related to intention to quit among the smokers (p's < .0001). No other correlates were significantly related to intention to quit among the chewers.
Table 3. Results of multivariate regression between smokers and chewers.
| Motivation to quit | ||
|---|---|---|
|
|
||
| Smokers | Chewers | |
| Number of years used | -0.05 (0.02)** | -0.25 (0.05)*** |
| Use everyday | -0.02 (0.03) | 0.01 (0.05) |
| Number of use per day | -0.22 (0.02)*** | 0.03 (0.05) |
| Lifetime quit attempts | 0.08 (0.03)** | 0.16 (0.05)** |
| Dependence scalea | -0.20 (0.02)*** | 0.03 (0.02) |
Notes. Betas (Standard error) presented in the table. Models control for age, gender, ethnicity and education.
Dependence scales used were the BQDS for the chewers models and the FTND scale for the smokers.
p<.0001;
p<.01
Discussion
Intention is a critical component to changing people's behaivor. Despite the worldwide popularity of betel quid chewing and the associated health risks, there haven't been any studies assessing chewers' intention to quit. Understanding chewers' intention to quit betel quid can have substantial impacts on reducing cancer risk for a large portion of the global population. In the current study, we sought to understand chewers' intention to quit betel quid and how it compared to smokers' intention to quit cigarettes. A deeper understanding of chewers' intention to quit and its similarities to smokers' intention to quit could lead to the development of betel quid cessation interventions that are modeled after smoking cessation interventions.
As expected, betel quid and tobacco users were both highly motivated to quit, although the degree of intention differed between the two types of users. Smokers endorsed significantly stronger intention to quit on three of five intention measures; specifically, they were more likely to indicate that they “definitely” wanted to quit and intended to quit, compared to chewers. Smokers were also much more likely than chewers to endorse that they “definitely” wish they had never started smoking in the first place. A possible explanation for these differences could be in users' awareness of the health risks associated with each substance's use. In the United States, most smokers are aware of the negative health risks associated with smoking cigarettes; however, the negative health risks associated with chewing among Guamanians is less widely known. Unlike with cigarettes, betel quid in Guam does not come in packages with public health warnings regarding the dangers associated with chewing. Additionally, public health messages on the health risks associated with chewing betel quid are not widely disseminated in Guam. This lack of awareness of risk could explain the differences in intention observed across the samples. However, in the current study, we did not assess risk perceptions associated with betel quid chewing. Future studies should investigate whether risk perceptions are associated with intention to quit among chewers in order to inform future betel quid cessation interventions.
Another possible explanation for the observed differences in intention could be due to the fact that, unlike cigarette smoking in the U.S. which is generally met with social disapproval, betel quid is a socially accepted behavior in Guam. As a result, betel quid chewers may fear negative social repercussions associated with quitting. Thus, any tobacco cessation intervention adapted for chewers will need to have a strong social/cultural component that teaches chewers social skills for effectively dealing with peer and family pressure to chew, as well as culturally tailored training in refusal self-efficacy.
Interestingly, there were no significant differences across groups with regard to having a plan for how to quit and when to quit. In both samples, half of the respondents reported not having a plan for how or when to quit. Smokers in the sample reported having made on average 11.5 (SD=48.2) quit attempts compared to only 5.2 (SD=15.6) average quit attempts among the chewers. These results suggest that similar to smokers, chewers may be motivated to quit, but are in need of assistance in planning and carrying out a successful quit attempt. Cognitive-behavioral therapy (CBT) approaches that have been successful in promoting cessation among smokers [24], could be a potential starting point for developing betel quid cessation interventions. Additionally, given the similar withdrawal symptoms experienced by chewers and smokers, pharmacotherapies similar to those that have proven effective in aiding smoking cessation could be developed to help betel quid chewers quit chewing.
Not surprisingly, we found that higher levels of intention to quit were associated with more quit attempts and lower levels of use among both smokers and chewers. However, level of dependence was associated with intention to quit among smokers but not among chewers. Future etiologic research is needed to understand what other factors are associated with chewers' intention to quit. This type of research will be instrumental in developing betel quid cessation interventions.
The findings of the current study must be interpreted in light of several limitations. First, both samples were convenience samples. Although the samples included a broad range of chewers and smokers in terms of ethnicity, gender, and age, the results of the current study may not be representative of smokers or chewers generally. Also, the current study was cross-sectional, and as a result, we could not draw any conclusions regarding causality. However, because intention to quit could be a critical component of betel quid cessation interventions, future studies should explore whether intention to quit predicts self-initiated quit attempts in a longitudinal sample.
Researchers have found that intention to quit is an essential component for successful smoking cessation. Unfortunately, there is a dearth of research exploring betel quid chewers' pyschological orientation towards quitting. The current study is novel in that it is the first study to explore intention to quit betel quid among a sample of chewers, and compares their level of intention to a sample of cigarette smokers' intention to quit. These comparisons were made possible because of the deliberate use of identical questionnaire items (mutatis mutandis) for betel quid chewing and cigarette smoking. Cigarette smoking and betel quid chewing are different behaviors in many respects and thus we expected that the distributions of responses would be different to some extent. Further, the two samples were drawn from different populations (smokers in Hawaii and chewers in Guam), and evinced various other discrepancies such as age (the mean age for smokers was 10 years older than for chewers) and education (90% of smokers had a high school diploma versus 59% for chewers). Despite these differences in the samples, we found substantial similarities in the overall patterns of responses between smokers and chewers.
Conclusion
In the current study, we found that both smokers and chewers want to quit and intend to quit, but do not have plans of when or how to quit. Thus, based on these novel findings, we propose that the essential psychological orientation towards quitting is similar for smokers and chewers. This is an important point, because it suggests that betel quid cessation programs could be modeled after smoking cessation programs. However, additional research is needed to better understand the similarities and differences between smoking cessation and betel quid cessation. Future research should focus on other psychological and behavioral aspects of betel quid chewing and cessation such as dependence, reasons for betel quid use, and withdrawal symptoms [16]. Better understanding of these variables will aid in the development of efficacious betel quid cessation techniques.
Acknowledgments
We thank Clare Camacho-Aguon and Champ Fejeran for their assistance with participant recruitment and data entry.
Role of Funding Source: Funding for this study was provided by National Cancer Institute (NCI) Grant U54 CA143727.
The NCI had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication. M.A. Little was supported during the work on this project by a postdoctoral fellowship on NCI grant R25 CA90956.
Footnotes
Competing Interests: All authors declare that they have no conflict of interest.
Authors' Contributions: ML and PP performed statistical analyses and wrote sections of the manuscript. TH and KM designed the study and wrote sections of the manuscript. CK and GS wrote the protocol and contributed to the survey design. All authors contributed to and have approved the final manuscript.
References
- 1.Boucher BJ, Mannan N. Metabolic effects of the consumption of Areca catechu. Addict Biol. 2002;7:103–110. doi: 10.1080/13556210120091464. http://www.ncbi.nlm.nih.gov/pubmed/11900629. [DOI] [PubMed] [Google Scholar]
- 2.Warnakulasuriya S, Peters TJ. Introduction: Biology, medical and socio-economic aspects of areca nut use. Addiction Biology. 2002;7:75–76. http://onlinelibrary.wiley.com/doi/10.1080/13556210020091428/abstract. [Google Scholar]
- 3.Gupta PC, Warnakulasuriya S. Global epidemiology of areca nut usage. Addiction Biology. 2002;7:77–83. doi: 10.1080/13556210020091437. http://www.ncbi.nlm.nih.gov/pubmed/11900626. [DOI] [PubMed] [Google Scholar]
- 4.Winstock A. Areca nut-abuse liability, dependence and public health. Addict Biol. 2002;7:133–138. doi: 10.1080/13556210120091509. http://www.ncbi.nlm.nih.gov/pubmed/11900633. [DOI] [PubMed] [Google Scholar]
- 5.Iarc Working Group on the Evaluation of Carcinogenic Risks to Humans. IARC monographs on the evaluation of carcinogenic risks to humans. Lyon, France: IARC; 2004. Betel-quid and areca-nut chewing and some areca-nut derived nitrosamines. 2005/01/08. http://monographs.iarc.fr/ENG/Monographs/PDFs/index.php. [PMC free article] [PubMed] [Google Scholar]
- 6.Trivedy CR, Craig G, Warnakulasuriya S. The oral health consequences of chewing areca nut. Addiction Biology. 2002;7:115–125. doi: 10.1080/13556210120091482. http://www.ncbi.nlm.nih.gov/pubmed/11900631. [DOI] [PubMed] [Google Scholar]
- 7.Iarc. International Agency for Research on Cancer. Lyon, France: World Health Organization; 2012. A review of human carcinogens - personal habits and indoor combustions. http://monographs.iarc.fr/ENG/Monographs/PDFs/index.php. [Google Scholar]
- 8.Lin CF, Wang JD, Chen PH, Chang SJ, Yang YH, et al. Predictors of betel quid chewing behavior and cessation patterns in Taiwan aborigines. BMC Public Health. 2006a;6:271. doi: 10.1186/1471-2458-6-271. http://www.biomedcentral.com/1471-2458/6/271/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ghani WM, Razak IA, Yang YH, Talib NA, Ikeda N, et al. Factors affecting commencement and cessation of betel quid chewing behaviour in Malaysian adults. BMC Public Health. 2011;11:82. doi: 10.1186/1471-2458-11-82. http://www.ncbi.nlm.nih.gov/pubmed/21294919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee CH, Ko AM, Warnakulasuriya S, Ling TY, Sunarjo, et al. Population burden of betel quid abuse and its relation to oral premalignant disorders in South, Southeast, and East Asia: an Asian Betel-quid Consortium Study. Am J Public Health. 2012b;102:e17–24. doi: 10.2105/AJPH.2011.300521. http://www.ncbi.nlm.nih.gov/pubmed/22390524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Winstock AR, Trivedy CR, Warnakulasuriya KaaS, Peters TJ. A dependency syndrome related to areca nut use: some medical and psychological aspects among areca nut users in the Gujarat community in the UK. Addiction Biology. 2000;5:173–179. doi: 10.1080/13556210050003766. http://www.ncbi.nlm.nih.gov/pubmed/20575832. [DOI] [PubMed] [Google Scholar]
- 12.Bhat SJS, Blank MD, Balster RL, Nichter M, Nichter M. Areca nut dependence among chewers in a South Indian community who do not also use tobacco. Addiction. 2010;105:1303–1310. doi: 10.1111/j.1360-0443.2010.02952.x. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3143027/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Benegal V, Rajkumar RP, Muralidharan K. Does areca nut use lead to dependence? Drug Alcohol Depend. 2008;97:114–121. doi: 10.1016/j.drugalcdep.2008.03.016. http://www.ncbi.nlm.nih.gov/pubmed/18490113. [DOI] [PubMed] [Google Scholar]
- 14.Chandra PS, Carey MP, Carey KB, Jairam KR. Prevalence and correlates of areca nut use among psychiatric patients in India. Drug Alcohol Depend. 2003;69:311–316. doi: 10.1016/s0376-8716(02)00329-0. http://www.ncbi.nlm.nih.gov/pubmed/12633917. [DOI] [PubMed] [Google Scholar]
- 15.Mubeen K, Kumar CN, Puja R, Jigna VR, Chandrashekar H. Psychiatric morbidity among patients with oral sub-mucous fibrosis: a preliminary study. J Oral Pathol Med. 2010;39:761–764. doi: 10.1111/j.1600-0714.2010.00948.x. http://www.ncbi.nlm.nih.gov/pubmed/20923447. [DOI] [PubMed] [Google Scholar]
- 16.Lam CY, Gritz ER. Incorporating behavioral research to examine the relationship between betel quid chewing and oral cancer in Taiwan. BioMedicine. 2012;2:160–166. http://www.sciencedirect.com/science/article/pii/S2211802012000769. [Google Scholar]
- 17.Chen KT, Chen CJ, Fagot-Campagna A, Narayan KM. Tobacco, betel quid, alcohol, and illicit drug use among 13- to 35-year-olds in I-Lan, rural Taiwan: prevalence and risk factors. Am J Public Health. 2001;91:1130–1134. doi: 10.2105/ajph.91.7.1130. http://www.ncbi.nlm.nih.gov/pubmed/11441745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Balmford J, Borland R. What does it mean to want to quit? Drug Alcohol Rev. 2008;27:21–27. doi: 10.1080/09595230701710829. http://www.ncbi.nlm.nih.gov/pubmed/18034378. [DOI] [PubMed] [Google Scholar]
- 19.Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. British Journal of Addiction. 1991;86:1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. http://www.ncbi.nlm.nih.gov/pubmed/1932883. [DOI] [PubMed] [Google Scholar]
- 20.Lee CY, Chang CS, Shieh TY, Chang YY. Development and validation of a self-rating scale for betel quid chewers based on a male-prisoner population in Taiwan: The Betel Quid Dependence Scale. Drug and Alcohol Dependence. 2012a;121:18–22. doi: 10.1016/j.drugalcdep.2011.07.027. http://www.ncbi.nlm.nih.gov/pubmed/21955360. [DOI] [PubMed] [Google Scholar]
- 21.Herzog TA, Murphy KL, Little MA, Suguitan GS, Pokhrel P, et al. The Betel Quid Dependence Scale: Replication and extension in a Guamanian sample. Drug Alcohol Depend. 2014;138:154–160. doi: 10.1016/j.drugalcdep.2014.02.022. http://www.ncbi.nlm.nih.gov/pubmed/24629627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000. http://www.psych.org/practice/dsm. [Google Scholar]
- 23.Sas Institute Inc. Sas/C Online Doc Tm. Release 9.0. Cary, NC: SAS Institute; 2000. http://www.sas.com/en_us/software/enterprise-guide.html. [Google Scholar]
- 24.Perkins KA, Conklin CA, Levine MD. Cognitive-behavioral therapy for smoking cessation: a practical guidebook to the most effective treatments. New York: Routledge; 2008. http://onlinelibrary.wiley.com/doi/10.1002/pon.1360/abstract. [Google Scholar]