

Abstract
Introduction
Inhaled nitric oxide (iNO) is an important therapy for acute respiratory distress syndrome (ARDS), pulmonary hypertension and pediatric hypoxemic respiratory failure. Safety concerns regarding iNO and renal dysfunction have been reported; however, there are currently no systematic reviews on this issue. Our objective was to evaluate published randomized controlled trials (RCTs) to ascertain the risk of renal dysfunction associated with iNO therapy in patients with and without ARDS.
Methods
A systematic review of databases was performed to identify RCTs which compared iNO with controls up to September 2014. Effect estimates for risk ratio (RR) of acute kidney injury (AKI) were pooled using a random-effects model.
Results
Ten RCTs involving 1363 participants were included. Inhaled nitric oxide significantly increased the risk of AKI compared with controls (RR, 1.4, 95%CI, 1.06 to 1.83, p = 0.02). In the stratified analysis, a high cumulative-dose of iNO significantly increased the risk of AKI (RR, 1.52, 95%CI, 1.14 to 2.02, p = 0.004), whereas medium and low cumulative-doses did not (RR, 0.64, 95%CI, 0.23 to 1.81 and RR, 0.56, 95%CI, 0.11 to 2.86 respectively). In subgroup analysis by study population, an increased risk of AKI was observed in patients with ARDS (RR, 1.55, 95%CI, 1.15 to 2.09, p = 0.005) but not in those without (RR, 0.90, 95%CI, 0.49 to 1.67, p = 0.75).
Conclusions
The available data show that iNO therapy may increase the risk of renal dysfunction, especially with prolonged use and in patients with ARDS. The risk in pediatric population is unknown owing to limited data. We suggest monitoring renal function during iNO therapy, and that future trials of iNO should evaluate renal safety.
Electronic supplementary material
The online version of this article (doi:10.1186/s13054-015-0880-2) contains supplementary material, which is available to authorized users.
Introduction
Nitric oxide was first reported to be an endogenous vasodilator in 1987 [1]. Soon after this discovery, inhaled nitric oxide (iNO) was applied to treat pulmonary hypertension and various pulmonary diseases [2,3]. Previous studies and clinical trials have shown that iNO possesses the therapeutic effects of selective pulmonary vasodilatation without causing systemic hypotension, and an effect on improving ventilation-perfusion mismatch [3,4]. Currently, iNO has been an important treatment modality for pulmonary hypertension, acute respiratory distress syndrome (ARDS), and pediatric hypoxemic respiratory failure [5-7].
Cumulative data from physiological studies and clinical trials suggest that iNO therapy has a good safety profile [8-10], and that its potential adverse effects, including methemoglobinemia, inhibition of platelet aggregation and systemic vasodilatation, are usually clinically insignificant [8,11,12]. However, a safety concern about renal dysfunction for nitric oxide inhalation was reported in a meta-analysis designed to evaluate the efficacy of iNO in ARDS [13]. This finding contradicts earlier evidence that iNO has favorable effects on renal and splanchnic perfusion [8]. In addition, this adverse effect, as a class effect of iNO therapy, was not observed in non-ARDS populations. These contrasting findings warrant further investigation to clarify the association between iNO and the risk of renal dysfunction in patients with and without ARDS. Therefore, we conducted this systematic review and meta-analysis to ascertain the risk of acute kidney injury (AKI) in iNO therapy and to investigate whether the risk varies among different patient populations.
Materials and methods
Search strategy
This systematic review was conducted using an a priori published protocol submitted to the PROSPERO website (Registration number CRD42013005731) and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria [14]. No institutional review board approval or consents were needed for this systematic review because it evaluated published studies. We searched MEDLINE via the NCBI Entrez system and Cochrane Central Register of Controlled Trials up to 25 September 2014. Bibliographies of retrieved studies and recent review articles were also screened to identify additional trials. Both keywords and MeSH terms searches were used to identify relevant citations. The search terms were “inhaled nitric oxide” AND “randomized controlled trial”, and MeSH terms were “Nitric Oxide/therapeutic use” [Mesh] AND “Randomized Controlled Trial” [Publication Type]. There were no language restrictions. Details of our search strategy are shown in the online appendix (see Additional file 1). The eligible studies were parallel randomized controlled trials (RCTs) comparing patients who did and did not receive iNO therapy. The exclusion criteria included crossover trials and studies not reporting AKI in the results.
Study selection and data extraction
Two investigators (SYR and TMH) screened studies for inclusion and independently extracted data from the included studies. Any disagreements were resolved by discussion. A standardized recording form was used for data extraction.
Assessment of risk of bias
Quality assessment of these studies was done using the Cochrane Collaboration tool for assessing the risk of bias [15]. We assessed the risk of bias associated with random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessments, incomplete outcome data, selective outcome reporting, and other bias. Two investigators (SYR and TMH) independently assessed the risk of bias in the individual studies, and discrepancies were resolved by consensus.
Outcome measures
The primary outcome of interest was AKI as defined in the individual studies regardless of the severity of injury. The secondary outcome was AKI requiring renal replacement therapy (RRT). Risk ratio (RR) was used as a measurement of association in the analysis.
Stratified analysis
Stratified analysis by study population was performed to investigate whether the risk of iNO-associated renal dysfunction varied among different patient populations. To test the dose-response relationship between iNO and the risk of renal dysfunction, stratified analysis by duration and dosage of iNO therapy was also performed.
Data synthesis
Outcome measures were pooled using a random-effects model with the inverse variance method because of anticipated heterogeneity among the included studies. We analyzed data by intention-to-treat analysis and calculated the point estimates and 95% CI of the summary effect. When one arm of a study contained no events, 0.5 was added to all cells of the two-by-two table [16]. Sensitivity analysis was performed to check the robustness of the effect estimate using different data synthesis models. The Peto method was used in the sensitivity analysis because of its advantage of a less biased estimate for summary effect in the settings of sparse data and imbalance of trial size [17]. Because the Peto method can only be used to calculate odds ratios (ORs), we also calculated ORs using a random-effects model to compare the effect sizes obtained by these two methods. Heterogeneity was explored using the Q-statistic and I2. Heterogeneity was considered low, moderate, and high according to I2 values of <25%, 25 to 50% and >50%, respectively [18]. Publication bias was evaluated by a funnel plot of standard error versus RR based on the primary outcome, and with Egger’s test [19]. For all analyses, a two-sided P-value <0.05 was considered to be statistically significant. The data were analyzed using Stata software, version 11 (StataCorp, Texas, USA).
Results
Literature search and study characteristics
Through the electronic searches and from references, 252 citations were identified. According to our predefined inclusion and exclusion criteria, 10 RCTs involving a total of 1,363 patients were included in the final analysis [12,20-28]. To calculate the risk for incident AKI, 26 patients were excluded from the analysis because they had received hemodialysis before the enrollment of trials. The number of studies evaluated at each stage of the literature review is shown in Figure 1. Quality assessment (see Additional file 2) of the included studies suggested a low risk of bias, except for one study which was published with an abstract [21].
Figure 1.
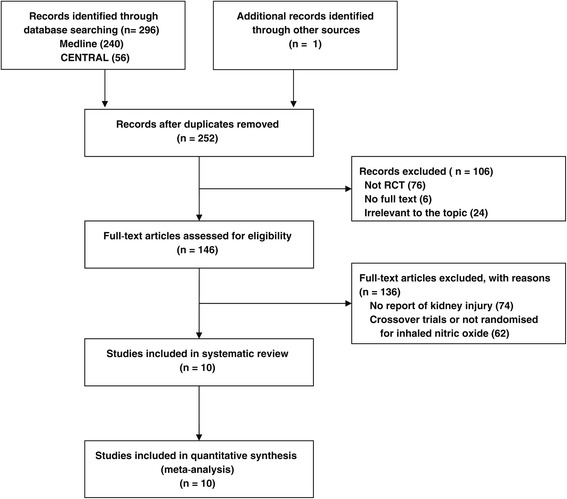
Study flow through this systematic review. RCT, randomized controlled trial.
The characteristics of the included studies are summarized in Table 1. The publication year ranged from 1998 to 2014, and included four studies on patients with ARDS, four studies on patients undergoing surgery, one study on neonates with hypoxemic respiratory failure, and one study on patients with sepsis. The administered dose and duration of iNO varied largely among these studies. In the ARDS trials, the dose of iNO shifted from a titrated dose of 1 to 40 ppm in the 1990s to a fixed dose of 5 ppm in the latest trial [12,23]. The treatment duration was longer in the ARDS studies (>7 days) than in the non-ARDS studies (≤7 days).
Table 1.
Details of the included randomized controlled trials
| Study (year) | Country | Study population | Protocol of iNO therapy | Mean iNO dosage | Age, years | Definition of acute kidney injury (AKI) | Number of AKI/number of cases | |
|---|---|---|---|---|---|---|---|---|
| iNO | Control | |||||||
| Dellinger (1998) [12] | USA | ARDS | 1.25, 5.0, 20.0, 40.0, or 80.0 ppm iNO for 28 days or till FiO2 < 0.5 | 21 ppm | 48 | Creatinine >2 mg/dL | 20/120 | 7/57 |
| Creatinine ≥3.5 mg/dL | 13/120 | 5/57 | ||||||
| Lundin (1999) [20] | 11 European countries | ARDS | 1 to 40 ppm iNO at the lowest effective dose for up to 30 days or until an end point was reached | 9 ppm | 57 | Creatinine >3.4 mg/dL or RRT | 28/80 | 12/74 |
| Incident RRT | 23/84 | 10/79 | ||||||
| Kinsella (1999) [22] | USA | Neonate hypoxemic respiratory failure | 5 ppm for 7 days | 5 ppm | 27 weeks | Renal failure | 2/48 | 2/32 |
| Payen (1999) [21] | Europe | ARDS | 10 ppm till PF >250, median 5 days | 10 ppm | Not reported | RRT | 33/98 | 26/105 |
| Taylor (2004) [23] | USA | ARDS | 5 ppm until 28 days, discontinuation of assisted breathing, or death | 5 ppm | 50 | Creatinine ≥3 mg/dL | 12/192 | 8/193 |
| Creatinine ≥3.5 mg/dL | 10/192 | 6/193 | ||||||
| Perrin (2006) [24] | France | Lung transplantation | 20 ppm for 12 h | 20 ppm | 35 | RRT | 1/15 | 1/15 |
| Potapov (2011) [26] | USA and Germany | Cardiac surgery | 40 ppm for 48 h | 40 ppm | 56 | RRT | 10/73 | 8/77 |
| Fernandes (2011) [25] | Brazil | Cardiac surgery | 10 ppm for 48 h | 10 ppm | 46 | Urine output <0.3 ml/kg/h | 0/14 | 1/15 |
| Lang (2014) [28] | USA | Liver transplantation | 80 ppm during the operative phase | 80 ppm | 56 | Renal dysfunction | 3/40 | 7/40 |
| Trzeciak (2014) [27] | USA | Sepsis | 40 ppm for 6 h | 40 ppm | 59 | RRT | 2/26 | 1/23 |
AKI, acute kidney injury; ARDS, acute respiratory distress syndrome; iNO, inhaled nitric oxide; FiO2: inspired oxygen fraction; PF: PaO2/FiO2 ratio; RRT: renal replacement therapy.
Reporting of renal dysfunction
Renal dysfunction in these trials was usually defined as an excess of creatinine level to a predefined level or the need for renal replacement therapy (Table 1). Among these trials, three reported the data of two different definitions of renal dysfunction. Notably, many clinical trials of iNO were excluded from this systematic review due to a lack of data on renal adverse effects, especially in the pediatric studies. Bleeding and neurological complications were the main concerns for the pediatric patients, and data on renal dysfunction were rarely reported in the safety outcomes.
Quantitative data synthesis
For the primary outcome of AKI with any severity (Figure 2), the pooled effect from 10 studies showed that iNO therapy significantly increased the risk of AKI with an RR of 1.40 (95% CI, 1.06 to 1.83, P = 0.02, I2 = 0%). The study by Payen [21] accounted for 39% of meta-analysis weight but was only published with an abstract. After omitting this influential study, the effect estimate remained similar (RR, 1.42, 95% CI, 1.003 to 2.01, P = 0.048, I2 = 0%). The statistical heterogeneity was low among the analyses.
Figure 2.
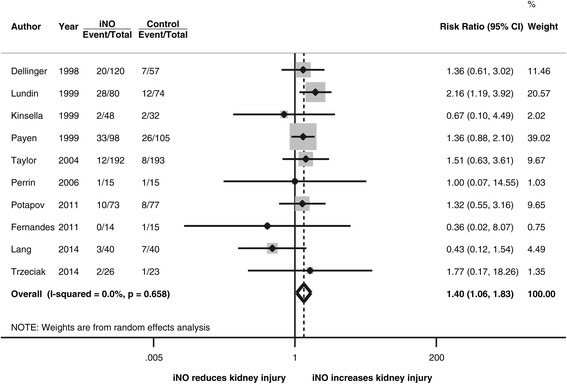
Forest plot for the risk of acute kidney injury. iNO, inhaled nitric oxide.
For the endpoint of AKI requiring renal replacement therapy (Figure 3), iNO also increased the risk with a RR of 1.51 (95% CI, 1.09 to 2.11, P = 0.01, I2 = 0%). The effect estimate became larger after we omitted the influential study by Payen (RR, 1.76, 95% CI, 1.05 to 2.93, P = 0.03, I2 = 0%).
Figure 3.
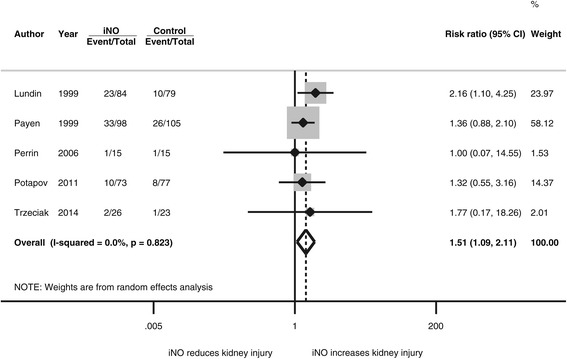
Forest plot for the risk of initiating renal replacement therapy. iNO, inhaled nitric oxide.
Due to the presence of sparse data and imbalance of trial size, sensitivity analysis was performed to evaluate the influence of data synthesis methods on the estimate of summary effect. The effect estimate by the Peto method was similar to that obtained by the primary analysis with a random-effects model (Table 2).
Table 2.
Sensitivity analysis by different data synthesis methods
| Outcome measures | Number of studies (number of patients) | Statistical model | Effect size (95% CI) | P -value (test for effect) | Heterogeneity |
|---|---|---|---|---|---|
| Acute kidney injury | 10 (1337) | RR, random-effects | 1.40 (1.06 to 1.83) | 0.02 | I 2 = 0% |
| OR, random-effects | 1.50 (1.07 to 2.09) | 0.02 | I 2 = 0% | ||
| OR, Peto | 1.48 (1.07 to 2.05) | 0.02 | I 2 = 0% | ||
| Initiation of renal replacement therapy | 5 (595) | RR, random-effects | 1.51 (1.09 to 2.11) | 0.01 | I 2 = 0% |
| OR, random-effects | 1.73 (1.13 to 2.65) | 0.01 | I 2 = 0% | ||
| OR, Peto | 1.73 (1.14 to 2.41) | 0.01 | I 2 = 0% |
RR, risk ratio; OR, odds ratio.
Figure 4 shows a funnel plot based on the primary outcome. The asymmetry of the funnel plot on visual inspection implied a lack of studies in which iNO increased the risk of AKI. This suggests that the pooled effect from the current data may underestimate the effect size of the risk. However, the statistical test for publication bias, Egger’s test (P = 0.33), did not reach statistical significance.
Figure 4.

Funnel plot based on the primary outcome.
The risk of AKI associated with iNO therapy varied among the different populations (Table 3). The risk was significantly increased in the patients with ARDS (RR, 1.55, 95% CI, 1.15 to 2.09, P = 0.005), but not in patients without ARDS (RR, 0.9, 95%CI, 0.49 to 1.67, P = 0.75). Among the patients with ARDS, the risk difference for AKI between iNO and control groups was 0.067 (95% CI, 0.000 to 0.135, P = 0.05, I2 = 50%), and the number needed-to-harm to cause one additional AKI was 15.
Table 3.
Subgroup analysis by study population
| Subgroups | Number of studies (number of patients) | Risk ratio of AKI (95% CI) | P -value (test for effect) | Heterogeneity |
|---|---|---|---|---|
| ARDS | 4 (919) | 1.55 (1.15 to 2.09) | 0.005 | I 2 = 0% |
| Non-ARDS | 6 (418) | 0.90 (0.49 to 1.67) | 0.75 | I 2 = 0% |
| Surgery | 4 (289) | 0.89 (0.45 to 1.75) | 0.73 | I 2 = 0% |
| Sepsis | 1 (49) | 1.77 (0.17 to 18.26) | 0.63 | Not applicable |
| Pediatric hypoxemic respiratory failure | 1 (80) | 0.67 (0.10 to 4.49) | 0.68 | Not applicable |
AKI, acute kidney injury; ARDS, acute respiratory distress syndrome.
To test the dose-response relationship between iNO and the risk of AKI, we performed stratified analysis by duration and dosage of iNO therapy. Prolonged use of iNO (>7 days) significantly increased the risk of AKI (RR, 1.55, 95% CI, 1.15 to 2.09, P = 0.005, four studies), whereas short-term use did not (RR, 0.90, 95% CI, 0.49 to 1.67, P = 0.75, six studies). Notably, the four studies involving the prolonged use of iNO are all ARDS studies. Table 4 summarizes the risk of renal dysfunction for different iNO exposure levels. We classified the included studies into three groups according to the cumulative dose in the stratified analysis. High cumulative dose of iNO significantly increased the risk of renal dysfunction but medium and low cumulative doses did not (Table 4). Figure 5 depicts the relationship between the risk of renal dysfunction and cumulative dose of iNO. Visual inspection suggested a possible association between the cumulative dose and risk of renal dysfunction but statistical test by meta-regression analysis was not significant due to small sample size (P = 0.10).
Table 4.
Dose-response relationship between inhaled nitric oxide and the risk of acute kidney injury
| Cumulative dose of inhaled nitric oxide | Numer of studies (number of patients) | Risk ratio of AKI (95% CI) | P -value (test for effect) | Heterogeneity | References |
|---|---|---|---|---|---|
| Low | 2 (109) | 0.56 (0.11 to 2.86) | 0.49 | I 2 = 0% | [22,25] |
| Medium | 3 (159) | 0.64 (0.23 to 1.81) | 0.40 | I 2 = 0% | [24,27,28] |
| High | 5 (1069) | 1.52 (1.14 to 2.02) | 0.004 | I 2 = 0% | [12,20,21,23,26] |
AKI, acute kidney injury.
Figure 5.
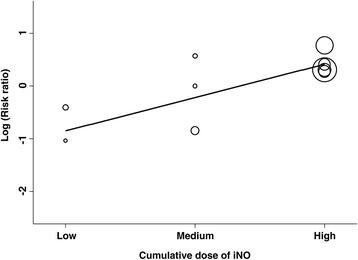
Bubble plot with fitted meta-regression line depicting the relationship between the risk of renal dysfunction and cumulative dose of inhaled nitric oxide (Ino).
Discussion
This meta-analysis updated the evidence on the renal safety of iNO therapy in ARDS and non-ARDS populations. The study suggested that the risk of iNO-associated renal dysfunction differed between ARDS and non-ARDS populations. The results showed that iNO therapy was associated with a 40% increased risk of renal dysfunction and the observed effect was mainly attributed to ARDS studies with prolonged use of iNO. If treating ARDS patients with iNO the number needed-to-harm to cause one additional AKI was 15. Sensitivity analysis by different data pooling methods revealed consistent effect estimates, and publication bias analysis suggested that the risk may be underestimated. Clinicians should be aware of this side effect when using iNO to treat patients. Our review also found that the safety outcome of renal dysfunction was not universally reported across iNO trials, especially in non-ARDS studies. We suggest that future trials of iNO should report renal safety outcomes.
The risk of renal dysfunction associated with iNO therapy was first reported in an RCT of patients with ARDS, in which iNO was found to double the risk of the need for renal replacement therapy compared with controls [20]. However, this adverse effect did not raise much attention because subsequent trials of iNO reported no significant increase in the risk of renal dysfunction [12,23]. In 2007, Adhikari and colleagues reported that iNO was associated with renal dysfunction in a meta-analysis [13]. This meta-analysis only included ARDS trials because the primary study interest was the efficacy of iNO on ARDS [13]. The strengths of our study are the comprehensive evaluations of iNO-related renal dysfunction among patients with and without ARDS, the influence of different endpoints of renal dysfunction, and the dose-response relationship. Although our analysis suggests that iNO may increase the risk of renal dysfunction, it is not clear whether the increased risk is ARDS-specific or related to prolonged use of iNO. We were unable to clarify this in study-level analysis because the ARDS studies all involved the prolonged use of iNO.
Generating awareness of the nephrotoxicity of iNO has important implications for preventing AKI in the intensive care unit. Previous studies have shown that the development of AKI significantly increased mortality in patients with ARDS [29]. We suggest that intensivists should be cautious about the concurrent use of iNO with other nephrotoxic agents such as certain antibiotics, when treating ARDS. Renal function should be regularly monitored during iNO therapy to detect possible AKI early. In addition, the nephrotoxicity of iNO may partly explain why iNO therapy improves oxygenation and attenuates inflammation but confers no benefit on mortality in patients with ARDS [3,30,31]. The benefits of iNO may be counterbalanced by the increased risk of renal failure, because organ failure is positively associated with mortality [32].
The mechanism of iNO-related renal dysfunction remains unclear. Table 5 summarizes the findings of animal and physiological studies on this issue [9,33-38]. These studies all examined the effect of short-term exposure to iNO, and most reported that iNO had beneficial effects on renal function except for a swine study which reported that iNO promoted renal tubular apoptosis [33]. In this swine model, renal resorption capacity was significantly blunted by iNO, and this may have led to tubular and glomerular injury by means of tubuloglomerular feedback [33]. With respect to nitric oxide metabolites, nitric oxide inhalation increased serum levels of plasma cyclic guanosine monophosphate (cGMP), nitrate, and nitrite [39]. These nitric oxide metabolites may play a role in AKI development owing to the effects on protein nitrosation and raising oxidative load [40-42]. In an animal model of drug-induced nephrotoxicity, elevated nitrite and nitrate levels were observed with increasing oxidative activity [40]. The induced nephrotoxicity could be ameliorated by selective phosphodiesterase-5 inhibitor by suppressing oxidative activity and nitrite and nitrate levels [40]. In addition, from the pathways of chemical reactions of nitric oxide in the lung, we speculate that oxidative injury caused by highly oxidant nitrogen compounds may also play a role in iNO-related kidney injury. Reactive nitrogen species such as nitrogen dioxide (NO2) are highly oxidative compounds that are produced when iNO mixes with high concentrations of oxygen in the alveoli [3,11]. In patients with ARDS treated with iNO, the serum concentrations of NO2 have been positively associated with the dose of iNO administered [12]. It has also been shown that systemically circulating NO2 may lead to cytotoxic effects on renal parenchymal cells [43]. This hypothesis of oxidative injury by reactive nitrogen species may also explain why nephrotoxicity tends to develop in patients with ARDS receiving iNO therapy, as these patients usually receive high-concentration oxygen therapy, which may facilitate the production of reactive nitrogen species. Animal studies are needed to test this hypothesis.
Table 5.
Animal and human studies investigating the effects of inhaled nitric oxide (iNO) on the kidneys
| Study (year) | Species | Protocols of iNO | Main findings |
|---|---|---|---|
| Valvini (1995) [38] | Human | 40 ppm for 3 days followed by 90 ppm for 2 days | 1. Inhaling 40 ppm nitric oxide would result in a daily nitrogen oxide load of about 25 mmol. |
| 2. Impairment of renal function would cause an increase in serum nitrogen oxides. | |||
| Troncy (1997) [9] | Swine | 40 ppm iNO | Inhaled nitric oxide increased renal blood flow, glomerular filtration rate and urinary flow. |
| Preiser (1998) [37] | Human | 1 to 20 ppm | 1. Renal excretion of NO2 − and NO3 − was unaltered by nitric oxide inhalation. |
| 2. Long-term nitric oxide inhalation was associated with a consistent increase in the NO3 − plasma concentration. | |||
| Wraight (2001) [36] | Human | 40 ppm for 2 h | Inhaled nitric oxide may alter tubular salt and water resorbtion. |
| Kielbasa (2001) [35] | Rat | 49 or 107 ppm iNO for 4 h | High dose of iNO increased nitric oxide synthase III protein expression, and nitrotyrosine and phosphotyrosine immunoreactivity. |
| Da (2007) [34] | Swine | 30 ppm iNO for 3.5 h | Decreased swelling and necrosis of glomeruli. |
| Gozdzik (2009) [33] | Swine | 40 ppm iNO for 30 h | 1. Transient natriuretic effect. |
| 2. Renal tubular apoptosis promotion after 30 h of iNO treatment. | |||
| Göranson (2014) [44] | Swine | 30 ppm iNO for 30 h | Combined therapy with iNO and intravenous steroid is associated with partial protection of kidney function. |
Limitations
Our study has limitations. First, the included number of studies and the number of cases in individual studies are small for the non-ARDS trials. This may have limited the statistical power of our subgroup analysis and meta-regression. Second, although the level of statistical heterogeneity was very low in all of our analyses, the heterogeneity on exposure (treatment duration and dosage of iNO) should not be overlooked. Third, death was a competing risk factor in our analysis. However, we were unable to adjust for this competing risk in study-level analysis. Individual data are needed to conduct such analyses.
Conclusion
This meta-analysis updated the evidence on the renal safety of iNO therapy in ARDS and non-ARDS populations. Our results suggest that iNO therapy substantially increases the risk of renal dysfunction. It remains unclear whether this markedly increased risk is disease-specific in ARDS or related to prolonged use of iNO. Further studies are needed to clarify this issue. We suggest that renal function should be monitored during iNO therapy and that future clinical trials of iNO should evaluate renal safety.
Key messages
Previous studies have shown that iNO has a good safety profile and favorable effects on renal and splanchnic perfusion; however, iNO therapy has been reported to be associated with renal dysfunction.
This meta-analysis updated the evidence regarding renal safety of iNO therapy. The study suggested that the risk of iNO-associated renal dysfunction differed between ARDS and non-ARDS populations. Nitric oxide inhalation may increase the risk of renal dysfunction, especially with prolonged use and in patients with ARDS.
The safety outcome of renal dysfunction was not universally reported across iNO trials, especially in non-ARDS studies. We suggest monitoring renal function during iNO therapy, and that future trials of iNO should evaluate renal safety.
Acknowledgements
Dr Sheng-Yuan Ruan was supported in part by a research grant of the Ministry of Science and Technology in Taiwan (103-2314-B-002 -153 -MY3).
Abbreviations
- AKI
acute kidney injury
- ARDS
acute respiratory distress syndrome
- iNO
inhaled nitric oxide
- OR
odds ratio
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
randomized controlled trial
- RR
risk ratio
- RRT
renal replacement therapy
Additional files
Details of the search strategy and results.
Quality assessment using the Cochrane risk of bias tool.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Study concept and design: SYR and MSL. Acquisition of data: SYR and TMH. Analysis and interpretation of data: SYR, TMH, HYW, HDW, CJY and MSL. Drafting the article: SYR, TMH, HYW, HDW and CJY. All authors revised the manuscript for important intellectual content. All authors read and approved the manuscript.
Contributor Information
Sheng-Yuan Ruan, Email: syruan@ntu.edu.tw.
Tao-Min Huang, Email: taomin.huang@gmail.com.
Hon-Yen Wu, Email: honyenwu@ntu.edu.tw.
Huey-Dong Wu, Email: hdwu@ntuh.gov.tw.
Chong-Jen Yu, Email: jefferycjyu@ntu.edu.tw.
Mei-Shu Lai, Email: mslai@ntu.edu.tw.
References
- 1.Palmer RM, Ferrige AG, Moncada S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature. 1987;327:524–6. doi: 10.1038/327524a0. [DOI] [PubMed] [Google Scholar]
- 2.Pepke-Zaba J, Higenbottam TW, Dinh-Xuan AT, Stone D, Wallwork J. Inhaled nitric oxide as a cause of selective pulmonary vasodilatation in pulmonary hypertension. Lancet. 1991;338:1173–4. doi: 10.1016/0140-6736(91)92033-X. [DOI] [PubMed] [Google Scholar]
- 3.Griffiths MJ, Evans TW. Inhaled nitric oxide therapy in adults. N Engl J Med. 2005;353:2683–95. doi: 10.1056/NEJMra051884. [DOI] [PubMed] [Google Scholar]
- 4.Rimar S, Gillis CN. Selective pulmonary vasodilation by inhaled nitric oxide is due to hemoglobin inactivation. Circulation. 1993;88:2884–7. doi: 10.1161/01.CIR.88.6.2884. [DOI] [PubMed] [Google Scholar]
- 5.Spieth PM, Zhang H. Pharmacological therapies for acute respiratory distress syndrome. Curr Opin Crit Care. 2014;20:113–21. doi: 10.1097/MCC.0000000000000056. [DOI] [PubMed] [Google Scholar]
- 6.Gayat E, Mebazaa A. Pulmonary hypertension in critical care. Curr Opin Crit Care. 2011;17:439–48. doi: 10.1097/MCC.0b013e32834a7619. [DOI] [PubMed] [Google Scholar]
- 7.Kumar P. Use of inhaled nitric oxide in preterm infants. Pediatrics. 2014;133:164–70. doi: 10.1542/peds.2013-3444. [DOI] [PubMed] [Google Scholar]
- 8.McMahon TJ, Doctor A. Extrapulmonary effects of inhaled nitric oxide: role of reversible S-nitrosylation of erythrocytic hemoglobin. Proc Am Thorac Soc. 2006;3:153–60. doi: 10.1513/pats.200507-066BG. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Troncy E, Francoeur M, Salazkin I, Yang F, Charbonneau M, Leclerc G, et al. Extra-pulmonary effects of inhaled nitric oxide in swine with and without phenylephrine. Br J Anaesth. 1997;79:631–40. doi: 10.1093/bja/79.5.631. [DOI] [PubMed] [Google Scholar]
- 10.Ng ES, Jourd’heuil D, McCord JM, Hernandez D, Yasui M, Knight D, et al. Enhanced S-nitroso-albumin formation from inhaled NO during ischemia/reperfusion. Circ Res. 2004;94:559–65. doi: 10.1161/01.RES.0000117771.63140.D6. [DOI] [PubMed] [Google Scholar]
- 11.Weinberger B, Laskin DL, Heck DE, Laskin JD. The toxicology of inhaled nitric oxide. Toxicol Sci. 2001;59:5–16. doi: 10.1093/toxsci/59.1.5. [DOI] [PubMed] [Google Scholar]
- 12.Dellinger RP, Zimmerman JL, Taylor RW, Straube RC, Hauser DL, Criner GJ, et al. Effects of inhaled nitric oxide in patients with acute respiratory distress syndrome: results of a randomized phase II trial. Inhaled Nitric Oxide in ARDS Study Group. Crit Care Med. 1998;26:15–23. doi: 10.1097/00003246-199801000-00011. [DOI] [PubMed] [Google Scholar]
- 13.Adhikari NK, Burns KE, Friedrich JO, Granton JT, Cook DJ, Meade MO. Effect of nitric oxide on oxygenation and mortality in acute lung injury: systematic review and meta-analysis. BMJ. 2007;334:779. doi: 10.1136/bmj.39139.716794.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harrison RJ, Bradburn MJ, Deeks JJ, Harbord RM, Altman DG, Sterne JAC. Metan: fixed- and random-effects meta-analysis. The Stata Journal. 2008;8:3–28. [Google Scholar]
- 17.Bradburn MJ, Deeks JJ, Berlin JA, Russell LA. Much ado about nothing: a comparison of the performance of meta-analytical methods with rare events. Stat Med. 2007;26:53–77. doi: 10.1002/sim.2528. [DOI] [PubMed] [Google Scholar]
- 18.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lundin S, Mang H, Smithies M, Stenqvist O, Frostell C. Inhalation of nitric oxide in acute lung injury: results of a European multicentre study. The European study group of inhaled nitric oxide. Intensive Care Med. 1999;25:911–9. doi: 10.1007/s001340050982. [DOI] [PubMed] [Google Scholar]
- 21.Payen D, Vallet B, Group d’étude du NO dans l’ARDS Results of the French prospective multicentric randomized double-blind placebo-controlled trial on inhaled nitric oxide (NO) in ARDS [Abstract] Intensive Care Med. 1999;25:166. doi: 10.1007/s001340050811. [DOI] [PubMed] [Google Scholar]
- 22.Kinsella JP, Walsh WF, Bose CL, Gerstmann DR, Labella JJ, Sardesai S, et al. Inhaled nitric oxide in premature neonates with severe hypoxaemic respiratory failure: a randomised controlled trial. Lancet. 1999;354:1061–5. doi: 10.1016/S0140-6736(99)03558-8. [DOI] [PubMed] [Google Scholar]
- 23.Taylor RW, Zimmerman JL, Dellinger RP, Straube RC, Criner GJ, Davis K, Jr, et al. Low-dose inhaled nitric oxide in patients with acute lung injury: a randomized controlled trial. JAMA. 2004;291:1603–9. doi: 10.1001/jama.291.13.1603. [DOI] [PubMed] [Google Scholar]
- 24.Perrin G, Roch A, Michelet P, Reynaud-Gaubert M, Thomas P, Doddoli C, et al. Inhaled nitric oxide does not prevent pulmonary edema after lung transplantation measured by lung water content: a randomized clinical study. Chest. 2006;129:1024–30. doi: 10.1378/chest.129.4.1024. [DOI] [PubMed] [Google Scholar]
- 25.Fernandes JL, Sampaio RO, Brandao CM, Accorsi TA, Cardoso LF, Spina GS, et al. Comparison of inhaled nitric oxide versus oxygen on hemodynamics in patients with mitral stenosis and severe pulmonary hypertension after mitral valve surgery. Am J Cardiol. 2011;107:1040–5. doi: 10.1016/j.amjcard.2010.11.030. [DOI] [PubMed] [Google Scholar]
- 26.Potapov E, Meyer D, Swaminathan M, Ramsay M, El Banayosy A, Diehl C, et al. Inhaled nitric oxide after left ventricular assist device implantation: a prospective, randomized, double-blind, multicenter, placebo-controlled trial. J Heart Lung Transplant. 2011;30:870–8. doi: 10.1016/j.healun.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 27.Trzeciak S, Glaspey LJ, Dellinger RP, Durflinger P, Anderson K, Dezfulian C, et al. Randomized controlled trial of inhaled nitric oxide for the treatment of microcirculatory dysfunction in patients with sepsis. Crit Care Med. 2014;42:2482–92. doi: 10.1097/CCM.0000000000000549. [DOI] [PubMed] [Google Scholar]
- 28.Lang JD, Jr, Smith AB, Brandon A, Bradley KM, Liu Y, Li W, et al. A randomized clinical trial testing the anti-inflammatory effects of preemptive inhaled nitric oxide in human liver transplantation. PLoS One. 2014;9:e86053. doi: 10.1371/journal.pone.0086053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Soto GJ, Frank AJ, Christiani DC, Gong MN. Body mass index and acute kidney injury in the acute respiratory distress syndrome. Crit Care Med. 2012;40:2601–8. doi: 10.1097/CCM.0b013e3182591ed9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Adhikari NK, Dellinger RP, Lundin S, Payen D, Vallet B, Gerlach H, et al. Inhaled nitric oxide does not reduce mortality in patients with acute respiratory distress syndrome regardless of severity: systematic review and meta-analysis*. Crit Care Med. 2014;42:404–12. doi: 10.1097/CCM.0b013e3182a27909. [DOI] [PubMed] [Google Scholar]
- 31.Afshari A, Brok J, Moller AM, Wetterslev J. Inhaled nitric oxide for acute respiratory distress syndrome and acute lung injury in adults and children: a systematic review with meta-analysis and trial sequential analysis. Anesth Analg. 2011;112:1411–21. doi: 10.1213/ANE.0b013e31820bd185. [DOI] [PubMed] [Google Scholar]
- 32.Sakr Y, Lobo SM, Moreno RP, Gerlach H, Ranieri VM, Michalopoulos A, et al. Patterns and early evolution of organ failure in the intensive care unit and their relation to outcome. Crit Care. 2012;16:R222. doi: 10.1186/cc11868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gozdzik W, Albert J, Harbut P, Zielinski S, Ryniak S, Lindwall R, et al. Prolonged exposure to inhaled nitric oxide transiently modifies tubular function in healthy piglets and promotes tubular apoptosis. Acta Physiol (Oxf). 2009;195:495–502. doi: 10.1111/j.1748-1716.2008.01908.x. [DOI] [PubMed] [Google Scholar]
- 34.Da J, Chen L, Hedenstierna G. Nitric oxide up-regulates the glucocorticoid receptor and blunts the inflammatory reaction in porcine endotoxin sepsis. Crit Care Med. 2007;35:26–32. doi: 10.1097/01.CCM.0000250319.91575.BB. [DOI] [PubMed] [Google Scholar]
- 35.Kielbasa WB, Fung HL. Systemic biochemical effects of inhaled NO in rats: increased expressions of NOS III, nitrotyrosine-, and phosphotyrosine-immunoreactive proteins in liver and kidney tissues. Nitric Oxide. 2001;5:587–94. doi: 10.1006/niox.2001.0386. [DOI] [PubMed] [Google Scholar]
- 36.Wraight WM, Young JD. Renal effects of inhaled nitric oxide in humans. Br J Anaesth. 2001;86:267–9. doi: 10.1093/bja/86.2.267. [DOI] [PubMed] [Google Scholar]
- 37.Preiser JC, De Backer D, Debelle F, Vray B, Vincent JL. The metabolic fate of long-term inhaled nitric oxide. J Crit Care. 1998;13:97–103. doi: 10.1016/S0883-9441(98)90012-0. [DOI] [PubMed] [Google Scholar]
- 38.Valvini EM, Young JD. Serum nitrogen oxides during nitric oxide inhalation. Br J Anaesth. 1995;74:338–9. doi: 10.1093/bja/74.3.338. [DOI] [PubMed] [Google Scholar]
- 39.Lukaszewicz AC, Mebazaa A, Callebert J, Mateo J, Gatecel C, Kechiche H, et al. Lack of alteration of endogenous nitric oxide pathway during prolonged nitric oxide inhalation in intensive care unit patients. Crit Care Med. 2005;33:1008–14. doi: 10.1097/01.CCM.0000163233.00458.DD. [DOI] [PubMed] [Google Scholar]
- 40.Morsy MA, Ibrahim SA, Amin EF, Kamel MY, Rifaai RA, Hassan MK. Sildenafil ameliorates gentamicin-induced nephrotoxicity in rats: role of iNOS and eNOS. J Toxicol. 2014;2014:489382. doi: 10.1155/2014/489382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Blanchard B, Dendane M, Gallard JF, Houee-Levin C, Karim A, Payen D, et al. Oxidation, nitrosation, and nitration of serotonin by nitric oxide-derived nitrogen oxides: biological implications in the rat vascular system. Nitric Oxide. 1997;1:442–52. doi: 10.1006/niox.1997.0147. [DOI] [PubMed] [Google Scholar]
- 42.Whitaker RM, Wills LP, Stallons LJ, Schnellmann RG. cGMP-selective phosphodiesterase inhibitors stimulate mitochondrial biogenesis and promote recovery from acute kidney injury. J Pharmacol Exp Ther. 2013;347:626–34. doi: 10.1124/jpet.113.208017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Han M, Guo Z, Li G, Sang N. Nitrogen dioxide inhalation induces genotoxicity in rats. Chemosphere. 2013;90:2737–42. doi: 10.1016/j.chemosphere.2012.11.057. [DOI] [PubMed] [Google Scholar]
- 44.Goranson SP, Gozdzik W, Harbut P, Ryniak S, Zielinski S, Haegerstrand CG, et al. Organ dysfunction among piglets treated with inhaled nitric oxide and intravenous hydrocortisone during prolonged endotoxin infusion. PLoS One. 2014;9:e96594. doi: 10.1371/journal.pone.0096594. [DOI] [PMC free article] [PubMed] [Google Scholar]