

Abstract
Introduction:
Numerous rehab protocols have been used in rehabilitation after ACL reconstruction. Isokinetic testing is an objective way to evaluate dynamic stability of the knee joint that estimates the quality of rehabilitation outcome after ACL reconstruction. Our investigation goal was to show importance of isokinetic testing in evaluation thigh muscle strength in patients which underwent ACL reconstruction and rehabilitation protocol.
Subjects and methods:
In prospective study, we evaluated 40 subjects which were divided into two groups. Experimental group consisted of 20 recreational males which underwent ACL reconstruction with hamstring tendon and rehabilitation protocol 6 months before isokinetic testing. Control group (20 subjects) consisted of healthy recreational males. In all subjects knee muscle testing was performed on a Biodex System 4 Pro isokinetic dynamo-meter et velocities of 60°/s and 180°/s. We followed average peak torque to body weight (PT/BW) and classic H/Q ratio. In statistical analysis Student’s T test was used.
Results:
There were statistically significant differences between groups in all evaluated parameters except of the mean value of PT/BW of the quadriceps et velocity of 60°/s (p>0.05).
Conclusion:
Isokinetic testing of dynamic stabilizers of the knee is need in diagnostic and treatment thigh muscle imbalance. We believe that isokinetic testing is an objective parameter for return to sport activities after ACL reconstruction.
Keywords: isokinetic test, ACL reconstruction, rehabilitation
1. INTRODUCTION
Isokinetic testing is a commonly utilized tool for the assessment of muscular strength in orthopedic and sports medicine setting abroad, but in our country or region were poor documented studies about it. In rehabilitation patients after ACL reconstruction isokinetic testing we use it for evaluation and treatment planning. Isokinetic is frequently chosen because of their inherent patient safety, objectivity and reproducibility in testing measures (1). Numerous research have documented clinical outcome studies utilizing peak torque parameters, especially the bilateral comparison ration of the quadriceps and hamstring muscles (2, 3). A few investigations have reported outcomes utilizing muscle performance parameters such as work, power and endurance (4).
2. OBJECTIVE
Aim of this paper is to present role of isokinetic testing in evaluation thigh muscle strength in patients which underwent ACL reconstruction and rehabilitation protocol.
3. PATIENTS AND METHODS
In prospective study, we evaluated 40 subjects which were divided into two groups, experimental and control. Experimental group consisted of 20 recreational males which underwent ACL reconstruction with hamstring tendon and rehabilitation protocol 6 month before isokinetic testing. Control group (20 subjects) consisted of healthy recreational males.
Knee muscle testing was performed on a Biodex System 4 Pro isokinetic dynamo-meter et velocities of 60°/s and 180°/s. All subjects included in this study had et least two prior testing on the Biodex System to familiarize them to the machine and testing sequence. The subjects were tested for knee extension and flexion strength using the following protocol: each subject performed a 6-minute active warm-up on stationary bicycle at a submaximal work level. The subjects were tested in a seated position, hip flexion et 110 to 125°, and stabilization straps were applied to the trunk and thighs. The resistance pad was placed at a level a proximally 3 cm proximal of medial malleolus. All subjects underwent testing of the uninvolved limb first. The range of motion of the knee joint during testing was set from 0-90° and all limbs were gravity compensated. Bilateral isokinetic (concentric/concentric) knee extension and flexion studies with the protocol of 60°/s (5 repetitions) and 180°/s (10 repetitions) were accomplished. Between two session subjects for 30 seconds. Vocal encouragement during the testing was consisted and standardized. Parameters which were followed, average power and H/Q ratios, automatically calculated by the device. In statistical analysis was used Student’s T test
4. RESULTS
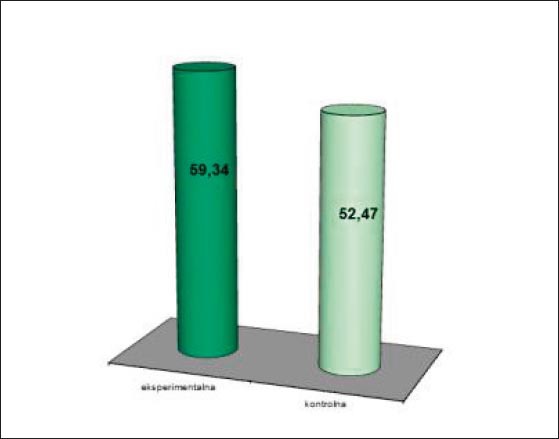
Statistically there are significant differences in the mean value of peak torque to body weight (PT/BW) in patients of experimental group et velocity 60°/s (p<0.01). (Figure 1). No significant differences were found in the mean value of PT/BW knee extensor muscle between evaluated groups et velocity 60°/sec (p>0.05) (Figure 2).
Figure 1.
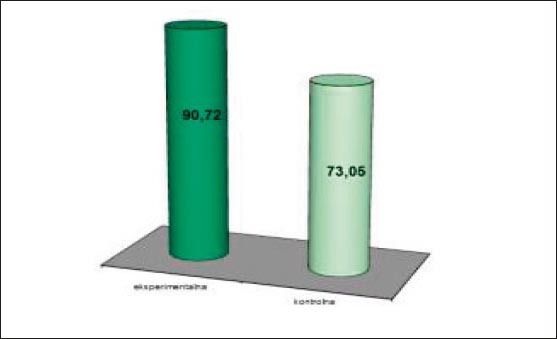
The mean value of PT/BW of knee flexors et velocity 60°/s
Figure 2.
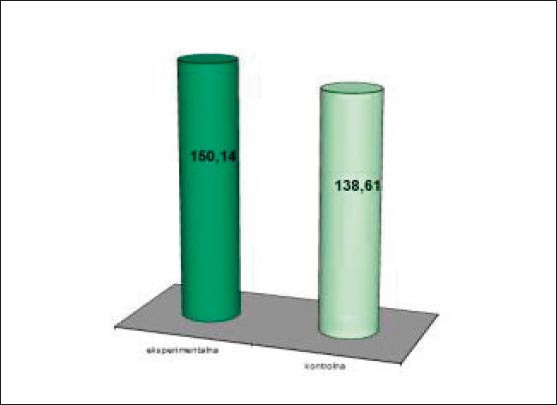
The mean value of PT/BW of knee extensors et velocity 60°/s
In addition, the endurance of dynamic stabilizers of the knee (extensor and flexor knee muscles) was statistically significant better in patients of experimental group versus control (p<0.01) (Figure 3 , 4.)
Figure 3.
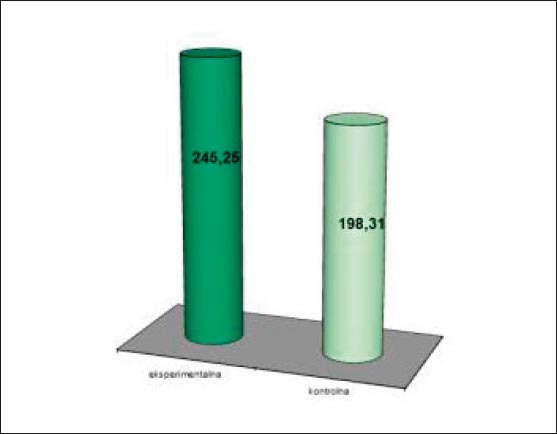
The mean value of PT/BW of knee extensors et velocity 180°/s
Figure 4.
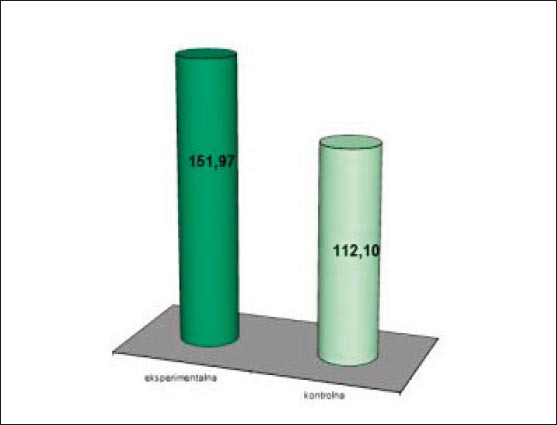
The mean value of PT/BW of knee flexors et velocity 180°/s
Observing the mean value of the classic H/Q ratio, there was statistically significant differences between evaluated group of patients in favor of experimental group (p<0.05) (Figure 5).
Figure 5.
The mean value of H/Q ratio in experimental and control group
5. DISCUSSION
Our primary finding was that patients after ACL reconstruction and underwent rehabilitation did not have muscle disbalance in knee fexors and extensor. A major area of focus in our study was to examine effect of rehabilitation protocol in this patients which we demonstrate by measurement muscle parameters of dynamic stabilizers of knee joint on isokinetic dynamo-meter Biodex 4 pro System. During the postoperative ACL rehabilitation we recommend hamstring strengthening exercises to reduce anterior tibial translation. There are studies that show adverse results about return strength of hamstring muscles after ACL reconstruction (5, 6). Some of them demonstrate relatively fast hamstring strength recovery, right after 12-14 weeks postoperatively on the preinjury level (5). On the other hand, Seto et all reported that hamstring strength in the reconstructed limb was significantly less in patients after ACL ligamentoplasty even after five years postoperatively (6). Results of our finding show complete recovery of the hamstrings muscles after 6 month postoperative and agrees to the study show by Wilk et all. Other than just of the recovery of hamstring muscle strength this all applies to endurance. Accelerated rehabilitation protocols after ACL reconstruction commonly employs immediate motion, weight bearing, neuromuscular electrostimulation and exercise to avoid inactivity and muscle hypothrophy of the quadriceps. We all know that the recovery of quadriceps muscle is very slow process. Up to 2 years may be needed to regain normal quadriceps muscle performance following ACL reconstruction (7). Even though, our results demonstrate that there are no significant differences in quadriceps strength muscle between ACL reconstructed patients and healthy recreational sportsmen. However, we showed that endurance of quadriceps muscle is significantly better in ACL reconstructed patients versus patients in control group, so we can conclude the positive outcome of adequate and continued rehabilitation. Our results do not agree with findings of Hoffman et al, but we must take in account that the study takes another surgical technique (patellar tendon graft) (8). The hamstring/quadriceps muscle strength ratio has been used as an indicator of normal balance between the knee flexors and extensors (9). It is some of very significant parameter in estimating the time of return to sports activities. Our ACL reconstructed patients after 6 months of the rehabilitation have the value of H/Q ratio in the recommended level which allows them to go back into sports activities.
6. CONCLUSION
Isokinetic testing of dynamic stabilizers of the knee is need in diagnostic and treatment thigh muscle imbalance after ACL injury and surgical intervention. It is an objective parameter for decision of return to sports activities after ACL reconstruction.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Saenz A, Avelanet M, Hijos E, Chaler J, Garreta R, Pujol E, Sandoval B, Buen C, Farreny A. Knee isokinetic test-retest: a multicentre knee isokinetic test-retest study of a fatigue protocol. Eur J Phys Rehabil Med. 2010 Mar;46(1):81–88. [PubMed] [Google Scholar]
- 2.de Carvalho Froufe Andrade AC, Caserotti P, de Carvalho CM, de Azevedo Abade EA, da Eira Sampaio AJ. Reliability of Concentric, Eccentric and Isometric Knee Extension and Flexion when using the REV9000 Isokinetic Dynamo-meter. J Hum Kinet. 2013 Jul;37:47–53. doi: 10.2478/hukin-2013-0024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Slider A, Thelen DG, Heiderscheit BC. Effects of prior hamstring strain injury on strength, flexibility, and running mechanics. Clin Biomech (Bristol, Avon) 2010 Aug;25(7):681–686. doi: 10.1016/j.clinbiomech.2010.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sanfilippo JL, Slider A, Sherry MA, Tuite MJ, Heiderscheit BC. Hamstring strength and morphology progression after return to sport from injury. Med Sci sports Exerc. 2013 Mar;45(3):448–453. doi: 10.1249/MSS.0b013e3182776eff. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wilk KE, Arrigo CA, Andres JR, et al. Anterior Cruciate Ligament reconstruction rehabilitation: a 12 week follow up of isokinetic testing in recreational athletes. Isokin Excer Sci. 1992;2(2):82–91. [Google Scholar]
- 6.Seto JL, Orofino AS, Morrissey MC, Medeiros JM, Mason WJ. Assesment of quadriceps/ hamstring strength, knee ligament stability, functional and sports activity levels five years after anterior cruciate ligament rehabilitaion. AM, J Sports Med. 1988 Mar-Apr;16(2):170–180. doi: 10.1177/036354658801600215. [DOI] [PubMed] [Google Scholar]
- 7.Risberg MA, Holm I, Tjomsland O, Ljuggren E, Ekland A. Prospective study of changes in impairments and disabilities after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1999 Jul;29(7):400–412. doi: 10.2519/jospt.1999.29.7.400. [DOI] [PubMed] [Google Scholar]
- 8.Hoffman M, Schrader J, Koceja D. An investigation of posteral control in postoperative anterior cruciate ligament reconstruction patients. J Ath Train. 1999 Apr;34(2):130–136. [PMC free article] [PubMed] [Google Scholar]
- 9.Hole CD, Smith GH, Hammond J, Kummar A, Saxton J, Cochrane T. Dynamic control and concentration strength ratio of the quadriceps and hamstrings in subjects with anterior cruciate ligament deficiency. Ergonomics. 2000 Oct;43(10):1603–1609. doi: 10.1080/001401300750004023. [DOI] [PubMed] [Google Scholar]