

Abstract
Introduction:
The patient’s record maintains all the diagnostic information with regards to patients and contains valuable information that can be beneficial to the dentist as well as legal authorities during forensic human identification.
Aim:
Objective of the study was to compare dental records with an ideal dental record form, as well as to compare between dental records of private clinics and academic hospitals and to assess the awareness and the knowledge of the dentists regarding the maintenance of their dental records accurate for medico-legal purposes.
Material and Methods:
A comparative cross-sectional study between records kept in private clinics and academic teaching hospitals in Khartoum locality.
Results:
Our results showed that Students are more likely to encounter accurate dental records more than dentists in private clinics. In conclusion Students are more aware regarding medicolegal purposes of maintenance of dental records. Accurate maintenance of dental records is more among dental students. Therefore, private clinics encounter dental records as financial documents.
Keywords: dental records, forensic dental identification, dental students, dentists
1. INTRODUCTION
The dental record, also referred to as the patient’s chart, is the official dental office document that records all of the treatment done and all patient-related communications that occur in the dental office (1).
Dental records play an important role in identification of a dead body which has been grossly decomposed and is difficult to identify visually. When this occurs, a variety of methods of dental identification are used. This is due to the capability of dental tissues to withstand high temperature, humidity and pressure (2, 3).
The American Academy of Paediatric dentistry has addressed the major elements of record-keeping which include, General charting considerations, Initial patient record, Components of a patient record, Patient medical and dental histories, Comprehensive and limited clinical examinations, Treatment planning and informed consent, Progress notes; correspondence, consultations and Ancillary documents; and confidential notes (1).
The dental practitioner must be aware of the importance of a dental record due to legal circumstances and maintenance of an accurate record ensures a high quality patient health care and service. The accuracy of a record determines the vitality of a dental practice and its maintenance determines good clinical practice and indicates skillfulness (4).
Forensic Dentistry aids in identification of individuals who’s are difficult to be recognized visually or in case of absence of fingerprints, personal effects and others due to disastrous accidents (5, 6, 7, 8).
Many dentists are still using paper patient records stored in file cabinets and shelves. Increasingly, dentists are incorporating new technologies into their practice to manage the large number of existing records (9).
For children there’s a different manner of retaining records. They must be kept for a certain period after the child grows up to a certain age. There must be a certain policy undergone by the dental office with all the dental teamwork compliant with and able to understand (4).
Microfilm and microfiche must be the tools for preserving the dental record, Confidentiality is beneficial in triggering honesty during communication, making a strong dentist-patient relationship (4).
Original records are never to be released, including radiographs, to any other component. No matter how formal a request for the originals may seem, only copies should be sent, the original records must be kept in the dental office (9).
With regards to the quality of record keeping in primary dental care, in Scotland Morgan et al reported a comparison between forms completed by District reference officers and forms by general dental practitioners, it has been found that 48% of the charting have been kept the same implying that records made within first visit have not been updated (10).
Dental identification mainly depends upon comparing postmortem records with the antemortem ones. Teeth are considered the most surviving body tissues to the postmortem events that are undergone by the body tissues as a result of death (4).
The lack of dental information such as medical records or incomplete records, was indicated as the cause of the failure of dentistry examinations of human identification by dental means (4).
Postmortem records produced by the forensic dentist include careful dental charting, supported by radiographic images. There are no certain criteria required for positive identification. Its important that the dentist must have reach conclusions with satisfying conclusions (19).
In October 2013, Petro studied the Effective Accuracy of Dental Records in Forensic Dental Identification in Sudan. 180 records were examined in 2 major governmental hospitals, 2 major governmental clinics and 2 private dental hospitals covering Khartoum state. This study showed a total absence of complete dental charting prior to treatment in governmental clinics, with only 8.3% in private centers which is supposed to supply better patient care and good quality treatment. Governmental hospitals showed only 50% of the records had a dental charting. Regarding register of name of examining dentist, in governmental clinics was very satisfactory as 100% of records have had dentist’s name registered, while private clinics had only 15% of their records containing dentists name and 50% in governmental hospitals. With regard to the presence of radiographs the records of the governmental clinics contained no radiographs as these were given to the patients; 50% in governmental hospitals had good quality of radiographs compared to the private centers; out of the 21 radiographs examined 13 were of good quality. A medical history of the patient was relatively well documented in the records examined in the governmental hospitals scoring 50%; only 16.7% was found in private centers and an absence of a medical history in the governmental clinics, this is because there is no provision made in the records for medical history in governmental clinics and due to the orientation of the private sectors towards financial income and saving time by taking a brief history. It was concluded that the general record keeping in Sudan is poor compared to other countries (11).
2. AIM OF THE STUDY
The aim of the study was to assess the accuracy and reliability of the dental records in 101 private dental clinics and three academic hospitals in Khartoum locality.
Specificifically to compare these records with the Australian Dental Association dental record form and to compare between records made in private and academic hospitals, for elements contributing to forensic identification and to assess the awareness and cognizance of the dentist regarding the maintenance of their dental records accurate for medico-legal purposes.
3. MATERIALS AND METHODS
Study was a Comparative Cross-sectional study conducted in Dental Teaching Hospitals and Private clinics in Khartoum locality; it was targeting Dentists working in private clinics and Dental Students studying in academic hospitals in Khartoum locality. Data was obtained from Dental hospitals including Academy Dental Teaching Hospital, University of Khartoum Dental Clinic and Khartoum College of Medical Sciences Dental Hospital. Total number of students from each college was obtained from their registration of each faculty. The major reason for choosing these hospitals is because they are the most attended academic teaching hospitals in Khartoum. Total number of students was 321. From Private, selection was done by Random Sampling Technique after determination of total number of dental clinics from Ministry Of Health, Khartoum state. Total Number of private clinics in Khartoum was obtained from the Ministry of health was 187.
Check list was prepared, as reference from the Australian Dental Association for dental records, including observation by Researcher focusing in their way of keeping records and emphasizing on the data that is relevant to the forensic identification process such as patient’s name, age, gender, date of appointment, photographs, radiographs, study models and full dental chart.
The study was approved by the researcher committee in the Ministry of health. Permission was obtained from the administration of different hospitals and dentists from private clinics, Dental students were informed consent to participate in the study. Those who refused to participate were excluded. Data was kept confidential.
4. RESULTS
Personal Data of the patient
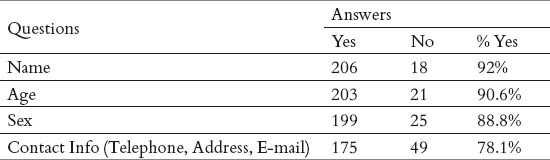
Table 1 demonstrates recording of personal of the patient which includes the patient’s name, age, sex and contact information. Patients name and age were most frequently recorded. (92%) recorded name of the patient. Regarding age, (90.6%) recorded patient’s age. Sex of patient was recorded by (88.8%). Regarding contact information, whether telephone, address or e-mail, (78.1%) recorded this information.
Table 1.
Distribution of the study sample according to (Personal Data of Patient)
Clinical details of patient:
The results of clinical details; date of appointment, date of visit, soft tissue examination and asking about presenting complain, full dental chart, diagnosis, medicine/drugs prescribed (name, quantity, instructions) and significant events (Adverse effects) was displayed on Table 2.
Table 2.
Distribution of the study sample according to (Clinical Details of Patient)
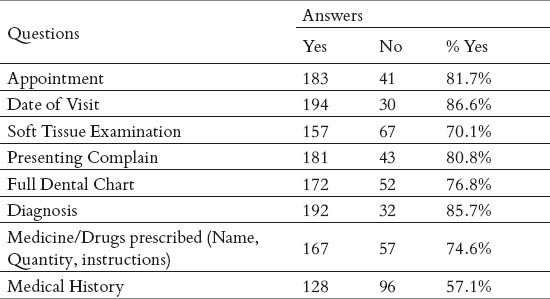
Table 3 illustrates comparison between recording periapical view as choice of radiograph in teaching hospitals and private clinics. P-Value of 0.002 i.e. P value > 0.05 was obtained indicating that there is statistical significance between academic hospitals and private clinics in recording periapical view as choice of radiograph.
Table 3.
Compare between records made in Private Clinics & teaching hospitals in obtaining periapical view radiograph of patient
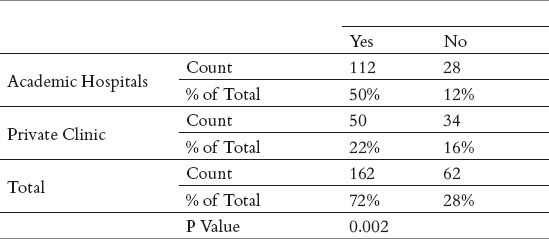
Table 4 illustrates comparison between recording a Panorama (OPG) as choice of radiograph in teaching hospitals and private clinics. P-Value of 0.004 i.e. P value > 0.05 was obtained indicating that there is statistical significance between academic hospitals and private clinics in recording OPG as choice of radiograph.
Table 4.
Compare between records made in Private Clinics & teaching hospitals in obtaining Panorama (OPG) radiograph of patient
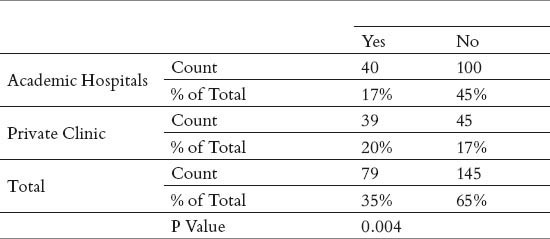
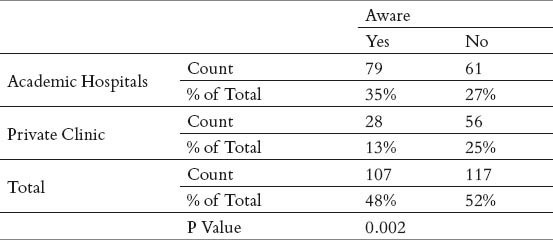
Table 5 illustrates comparison between record of full dental chart in teaching hospitals and private clinics. P-Value of 0.000 i.e. P value > 0.05 was obtained indicating that there is statistical significance between academic hospitals and private clinics in recording full dental charting. Table 6 illustrates assessment of awareness of the dentist regarding the maintenance of their dental records accurate for medico-legal purposes. P-Value of 0.002 i.e. P value > 0.05 was obtained indicating that there is statistical significance between academic hospitals and private clinics regarding awareness about the maintenance of their dental records accurate for medico-legal purposes.
Table 5.
Compare between records made in Private Clinics & teaching hospitals in recording full dental charting:
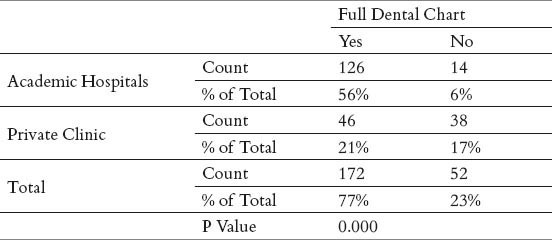
Table 6.
Comparison of Awareness between Students & Dentists regarding maintenance of dental records for medicolegal purposes:
5. DISCUSSION
The author in this study made a comparison between dental records made by students in academic teaching hospitals and dentists in private clinics with relevance to elements that contribute to forensic identification, such as name of the patient, age of patient, sex of patient, appointment, full dental charting, radiographs, photographs and cast/study models. In academic hospitals, students are taught the ideal maintenance of dental records of the patients. They are taught proper history taking and the importance of maintaining these records ideal for future referral. They are forced to follow the guidelines of recording all the information of their patients. This is because they will be assessed as requirements and examination; therefore they are obligated to obtain accurate records in order to obtain good marks and high degree.
In private clinics, practitioners tend to focus more on the income and the financial status of the clinic, therefore brief history is obtained in order to save time and admit more patients, thus increasing the income of the clinic. There has been a high significant level in negligence of the maintenance of dental records in private clinics. Private clinics encounter their records more of financial document rather than an accurate beneficial one, this saves their time in taking history in turn more patients are seen therefore increasing the income of their clinic.
Date of appointment is important for legal authorities in cases of a missing person or for instance, a suspect in the crime was seen, or needed to be identified at the last time and location seen (22, 23). This sort of information has been recorded by 55% of the students and only 27% of the private clinics, signifying a statistical significance of P value of 0.022, indicating that students have better record of patient’s appointments. Importance of recording appointment of the individual is to identify when the certain deceased individual or, a suspect was last seen.
The importance and value of radiographs must never be underestimated, as they play a major role in revealing tooth colored restoration and obtaining positive identification as well as they also play a role in age estimation, by number of teeth erupted (24, 25).
The presence of different types of dental radiographs in the records, predominantly the periapical view, was found 100% of the records. Choice of bitewing radiograph has not been in favour by both students and dentists, as only 8% of students and 6% of dentists obtained bitewing radiographs. This may be owed to the limited information provided by bitewing radiograph in only showing proximal caries, rather than showing the periapical area which frequently the most sites encountering pathologies.
The Panorama (OPG) was encountered at a similar rate between students and dentists, with slight higher rate in private clinics. This may be encountered as its use in viewing an overall condition of the patient’s dentition and bone, as well as any existing pathology. They also play a role in the process of age estimation especially in young children when seeing the amount of teeth erupted to the occlusal plane.
Photographs are important in identification of an individual visually, as the Countess of Salisbury has been identified visually by her gold denture (26). It has been noticed that dentists are not aware of this matter since only 8% recorded photographs of their patients. Students with a significantly higher rate of recording photographs of 28%, owing a statistical significance of P value 0.000. This maybe attributed that students might want to notice the difference before and after treatment to be evaluated in their performance by themselves or their superior guiders.
Casts and study models are very beneficial in the process of identifying an individual through the process regarded to as Rugoscopy as every individual in the world possesses a unique pattern and is considered a reliable method in post-mortem cases, but is considered impossible without antemortem records. Therefore, encountering casts and study models can be very beneficial (27). Statistically, 49% of students obtained cast and study models of their patients while only 21% of the dentists obtained them, indicating a statistical significance of P value of 0.001 between students and dentists in obtaining casts and study models of their patients. The low percentage of obtaining casts is may be attributed to the cost of materials, trays and time.
With regards to assessment of awareness of students and dentists about maintenance of their records for medico-legal purposes, 35% of students were aware and only 13% of dentists were aware, with a statistical significant of P value of 0.002 was obtained, indicating students are more aware regarding maintenance of records. This may be attributed to their compliance to their superior supervisors in maintaining these records accurate. As well as the absence of the clear guidelines from the health authorities leads to improper maintenance of records in private clinics.
6. CONCLUSION
The maintenance of accurate dental records is beneficial for both the dentists himself for future referral as well as the legal authorities in identification of a deceased individual in a less time consuming manner.
It has been revealed that students were more aware with regarding the maintenance of their dental records for medico-legal purposes and they are more likely to maintain an accurate dental record and are more reliable to refer to in cases of identification through dental records. This is attributed to the process of learning the ideal record and the strict obligations by the administration of the faculty in encountering and maintaining their records accurate.
Dental identification is one of the most important methods. Reliability and validation of dental records obtained facilitates a positive identification.
Recommendations
Quality assurance programmes must be annually or semi annually conducted to emphasize and increase the awareness of dental records. Educate students to maintain their knowledge and attitude towards dental records even after they are qualified dentists.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.American Academy of Pediatric Dentistry. Guideline on Record keeping. Pediatr Dent. 2004;34(special issue):132–136. [Google Scholar]
- 2.Fereira JL, Fereira AE, Ortega AI. Methods for the analysis of hard dental tissues exposed to high temperature. Forensic Sci Int. 2008;178(2):119–124. doi: 10.1016/j.forsciint.2007.12.009. [DOI] [PubMed] [Google Scholar]
- 3.Holden JL, Clement JG, Phakey PP. Age and temperature related changes to the ultrastructure and composition of human bone mineral. J Bone Miner Res. 1995;10(9):1400–1409. doi: 10.1002/jbmr.5650100918. [DOI] [PubMed] [Google Scholar]
- 4.Charangowda BK. Dental records: An overview. J Forensic Dent Sci. 2010 Jan-Jun;2(1):5–10. doi: 10.4103/0974-2948.71050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brannon RB, Kessler HP. Problems in mass disaster dental identification: a retrospective review. J Forensic Sci. 1999;44(2):123–127. [PubMed] [Google Scholar]
- 6.Alexander CJ, Foote GA. Radiology in forensic identification: the Mt. Erebus disaster. Australas Radiol. 1998;42(1):321–326. doi: 10.1111/j.1440-1673.1998.tb00531.x. [DOI] [PubMed] [Google Scholar]
- 7.Chapenoire S, Schuliar Y, Corvisier JM. Rapid, efficient dental identification of 92% of 13 train passengers carbonized during a collision with a petrol tanker. Am J Forensic Med Pathol. 1998;19(1):352–355. doi: 10.1097/00000433-199812000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Clark DH. An analysis of the value of forensic odontology in ten mass disasters. Int Dent J. 1994;44(2):241–250. [PubMed] [Google Scholar]
- 9.Leeuw W. CDA, maintaining proper dental records, at dentalcare.com Continuing Education Course 2013 July; 11. 2013:1–25. [Google Scholar]
- 10.Morgan RG. Quality evaluation of clinical records of a group of general dental practitioners entering a quality assurance programme. Br Dent J. 2001;19(1):436–441. doi: 10.1038/sj.bdj.4801201. [DOI] [PubMed] [Google Scholar]
- 11.Petro W, Philips VM. Cape Town South Africa: 2014. Jun 24, Effective accuracy of dental records in forensic dental identification in Sudan, Paper presented at: General Session of IADR international association of dental research. [Google Scholar]
- 12.Hincleff J. Forensic odontology, part 1. Dental identification, British Dental Journal. 2011 Mar;210(5):219–224. doi: 10.1038/sj.bdj.2011.146. [DOI] [PubMed] [Google Scholar]
- 13.Ratnakar P, Singaraju GS. Methods of identification in forensic dentistry. 2010 Jan;2(1):26–28. [Google Scholar]
- 14.Phillips VM, Stuhlinger M. The uniqueness of amalgam restorations for identification. J Forensic Odonto Stomatol. 1983;1(2):33–38. [PubMed] [Google Scholar]
- 15.Ahlqvist FJ. The use of dental radiographs for identification of children with un-restored dentitions. The Journal of Forensic Odonto-Stomatology. 2006 Dec;24(2):42–46. [PubMed] [Google Scholar]
- 16.Shekar BRC, Reddy CVK. Role of dentist in person identification. Indian J. Dent. Res. 2009;20(3):356–360. doi: 10.4103/0970-9290.57377. [DOI] [PubMed] [Google Scholar]
- 17.Thomas CJ, Kotze TW., Jr The palatal rugae pattern in six Southern African human populations. J Dent Assoc South Africa. 1983;38:547–553. [PubMed] [Google Scholar]
- 18.Lawney M. For the Record. Understanding Patient Recordkeeping. N Y State Dent J. 1998;64:34–43. [PubMed] [Google Scholar]
- 19.Pretty A, Sweet D. A Look at Forensic Dentistry - Part 1: The Role of Teeth in the Identification of Human Identity. Br Dent J. 2001;190(7):359–366. doi: 10.1038/sj.bdj.4800972. [DOI] [PubMed] [Google Scholar]
- 20.Zahrani A. Identification of unidentified human remains - validity od dental records. Pakistan Oral & Dent Jr. 2005 Jun;25(1):3–6. [Google Scholar]
- 21.Dierickx A, Seyler M, de Valck E, Wijffels J, Willems G. Dental Records: A Belgium Study. The Journal of Forensic Odonto-Stomatology. 2006;24(1):22–31. [PubMed] [Google Scholar]
- 22.Nelson GV. Records, charting, and problem areas in documentation: Part II. Pediatr Dent. 1989;2(3):240–242. [PubMed] [Google Scholar]
- 23.Mcdonald RE, Avery DR, Dean JA. 9th ed. St. Louis, Mo: Mosby; 2011. Examination of the mouth and other relevant structures; pp. 1–18. [Google Scholar]
- 24.American Academy of Pédiatrie Dentistry. Guideline on adolescent oral health care. Pediatr Dent. 2011;33(special issue):129–136. [Google Scholar]
- 25.American Academy of Pediatric Dentistty. Guideline on infant oral health care. Pediatric Dent. 2012;34(special issue):132–136. [Google Scholar]
- 26.American Academy of Pédiatric Dentistry. Guideline on periodicity of examination, preventive dental services, antieipatty guidance, and oral treatment for children. Pediatr Dent. 2011;33(special issue):102–109. [Google Scholar]
- 27.American Academy of Pédiatric Dentistty. Guideline on acquired temporomandibular disorders in infants, children, and adolescents. Pediatric Dent. 2011;33(special issue):248–253. [Google Scholar]