

Abstract
Background
We performed a proof of concept trial to evaluate relative safety and efficacy of Rhodiola rosea (R. rosea) versus sertraline for mild to moderate major depressive disorder.
Hypothesis
We hypothesize that R. rosea would have similar therapeutic effects as sertraline but with less adverse events.
Study Design
Phase II randomized placebo controlled clinical trial
Methods
57 subjects were randomized to 12 weeks of standardized R. rosea extract, sertraline, or placebo. Changes over time in Hamilton Depression Rating (HAM-D), Beck Depression Inventory (BDI), and Clinical Global Impression Change (CGI/C) scores among groups were examined using mixed-effects models.
Results
Modest, albeit statistically non-significant, reductions were observed for HAM-D, BDI, and CGI/C scores for all treatment conditions with no significant difference between groups (p=0.79, p=0.28, and p=0.17, respectively). The decline in HAM-D scores was greater for sertraline (−8.2, 95% confidence interval [CI], −12.7 to −3.6) versus R. rosea (−5.1, 95% CI: −8.8 to −1.3) and placebo (−4.6, 95% CI: −8.6 to −0.6). While the odds of improving (versus placebo) were greater for sertraline (1.90 [0.44–8.20]; odds ratio [95% CI]) than R. rosea (1.39 [0.38–5.04]), more subjects on sertraline reported adverse events (63.2%) than R. rosea (30.0%) or placebo (16.7%) (p=0.012).
Conclusions
Although R. rosea produced less antidepressant effect versus sertraline, it also resulted in significantly fewer adverse events and was better tolerated. These findings suggest that R. rosea, although less effective than sertraline, may possess a more favorable risk to benefit ratio for individuals with mild to moderate depression.
Keywords: Rhodiola rosea, Sertraline, Depression, Complementary & Alternative medicine, Botanical psychopharmacology
Introduction
Depression is one of the most common and debilitating psychiatric conditions. With a lifetime prevalence rate of about 16%, depression is associated with a high risk of suicide and much medical co-morbidity (Kessler et al., 2003). Nearly 70% of patients with depression have incomplete response to initial therapy with conventional antidepressants (Rush et al., 2006). In addition, conventional antidepressants have substantial side effects and often result in premature treatment discontinuation. Furthermore, many individuals with more mild depressive symptoms weigh concerns over side effects alongside the limited benefits and costs of conventional antidepressant therapy (Zimmermann et al., 2013). Thus, it is not surprising that depressive symptoms are among the most common reasons cited by consumers to choose alternative therapy (Barnes et al., 2004).
Rhodiola rosea (R. rosea), also known as roseroot or golden root, belongs to the family Crassulaceae (Darbinyan et al., 2000). Traditional folk medicine used R. rosea to promote work endurance, increase longevity, and to promote resistance to high altitude sickness, fatigue, depression and other health conditions. R. rosea may enhance mood and affect via its complex effect on central biogenic amines and β-endorphins. For example, R. rosea appears to stimulate noradrenalin, serotonin, dopamine, and acetylcholine receptors in brain regions involved in mood and affect (Brown R, 2002; Lazarova et al., 1986; Petkov et al., 1986; Saratikov et al., 1968). In in-vitro bioassay studies, R. rosea has also been shown to inhibit monoamine oxidase A and B enzymes (van Diermen et al., 2009). Further, studies suggest that R. rosea may have antidepressant activity via its ability to increase endogenous β-endorphin levels while preventing stress-induced elevation of β-endorphin (Lishmanov Iu et al., 1987), and via its action in prolonging the ‘forced swim test’ in rats (Abidov et al., 2003; Panossian et al., 2007).
To inform the design of a definitive study of R. rosea for major depressive disorder (MDD), the primary aim of the current study is to gain preliminary safety and efficacy data on the relative antidepressant action of R. rosea versus sertraline in outpatients with mild to moderate MDD.
Materials and methods
Study Design
We performed a randomized, double-blind, placebo-controlled, 12-week, proof of concept study of R. rosea versus sertraline among patients with mild to moderate MDD. This study was approved by the Institutional Review Board (IRB) of the University of Pennsylvania. All participants provided written informed consent. The study was conducted using the Principles of Good Clinical Practice Guidelines, with oversight by the local Office of Human Research and by an independent Data & Safety Monitoring Board. A complete description of the study protocol has been published (Mao et al., 2014).
Participants
Participants were referred from the Department of Family Medicine & Community Health outpatient clinics at the University of Pennsylvania and from self-referrals via advertisements in radio and newspapers. All were ≥ 18 years old and had a DSM IV Axis I diagnosis of MDD that was ascertained using the Structured Clinical Interview for DSM IV (SCID) interview format (First, 2001). Patients had a minimum baseline total Hamilton Depression Rating (HAM-D)(Williams, 1988) score ≥ 10 and a baseline Clinical Global Impression Severity (CGI/S)(Guy, 1976) rating of 3 (‘mild’) or 4 (‘moderate’). Patients were excluded from the trial if they had a current diagnosis of severe MDD, bipolar disorder, psychosis, substance abuse or dependence disorder within the preceding 3 months, primary anxiety disorder (e.g., panic disorder), or dementia. Other exclusion criteria included: currently receiving antidepressant treatment; actively suicidal or requiring hospitalization; uncontrolled medical condition (e.g., diabetes); pregnant or nursing women; women of child-bearing potential not using a medically acceptable form of contraception; use of concurrent herbs, remedies or mineral supplements (except mineral supplements prescribed for medical purposes – e.g., osteoporosis); use of chemotherapy or other medication known to produce mood changes; sensitivity to R. rosea or sertraline; history of non-response to sertraline; MAO inhibitor use within 14 days of starting study drug; or use of antidepressant, mood stabilizer, or antipsychotic drug within ≥ 5 elimination half-lives of starting study drug.
Randomization and Masking
Permuted blocked randomization with varying block sizes was used to assign participants to each of the three groups using Stata software. The PI, participants, clinical assessors, data manager, and statisticians were blinded to treatment assignment.
Interventions
Identically appearing capsules containing either pharmaceutical grade R. rosea SHR-5 powdered extract 340 mg (standardized to a content of rosavin 3.07%/rhodioloside 1.95%) (Swedish Herbal Institute, Gothenburg, Sweden), sertraline 50 mg HCl (North Star Pharmaceuticals, Memphis, TN), or placebo (i.e., lactose monohydrate NF) (Spectrum® Quality Products, New Brunswick, NJ) was prepared. All SHR-5 product was administered under IND #105,063 issued by the US Food and Drug Administration.
Outcome evaluation
At baseline visit, a psychiatric history was obtained using the SCID interview format (First, 2001). A medical history, physical examination, and laboratory evaluation was performed that included complete blood count, electrolytes, hepatic, renal and thyroid panel, pregnancy test (in women of child-bearing potential), urinalysis, and urine drug screen. Structured symptom ratings were obtained by a clinician at each study visit using the 28-item Hamilton Depression (HAM-D) rating (Williams, 1988), which was used to determine the primary outcome of 17-item HAM-D score. Clinician-rated Clinical Global Impressions of Change (CGI/C) (Guy, 1976), and patient-reported Beck Depression Inventory (BDI) scores (Beck, 1988; Beck et al., 1961) were secondary outcomes. A standardized treatment emergent side effects profile was used to evaluate adverse events (Anonymous, 1985). Blood pressure, pulse, and weight were obtained at each study visit. All evaluations took place at the Depression Research Unit at the University of Pennsylvania.
Treatment Procedures
Study drug was administered in a dose-escalation fashion. Dosage was initiated at one capsule daily for the first 2 weeks. Patients with ≤ 50% reduction in the 17-item HAM-D score (versus baseline) after 2 weeks of therapy had their dose increased to 2 capsules daily during weeks 3 and 4 of therapy. Patients who continued to have ≤ 50% reduction in HAM-D score (versus baseline) after 4 weeks of therapy had their dose increased to 3 capsules daily during weeks 5 and 6 of therapy. Patients who continued to have ≤ 50% reduction in HAM-D score (versus baseline) after 6 weeks of therapy had their dose increased to 4 capsules daily during study weeks 6 through 12 of therapy. Patients who were unable to tolerate the assigned dose of study drug had their dosage reduced to a minimum of 1 capsule daily. Patients who were unable to tolerate 1 capsule daily were discontinued from the trial. Outcome measurements were obtained at baseline and after 2, 4, 6, 8 and 12 weeks of treatment.
Sample Size
Although not specifically powered to detect small, statistically significant differences, the study was powered to detect relatively large differences between treatment groups, as well as trends in the data that may inform future study design. For the proposed sample size of 48 subjects, (16 per treatment condition), a one-way analysis of variance (ANOVA) would have 80% power to detect (at the 0.05 level) an effect size of 0.46. This effect size is expressed as the standard deviation (SD) of the means across three groups in the alternative hypothesis relative to the within group SD. In addition, the detectable between-group mean difference from a two-sample t-test at the 0.05 level was 1 within group SD for 16 subjects per group (Mao et al., 2014).
Data Analysis
Analysis was conducted under blinded conditions using STATA (Version 13; College Station, TX: STATA Corp LP) on an intention-to-treat basis. Testing was 2-sided with a significance level set at p < 0.05. Analysis of variance (ANOVA) or Pearson’s chi-squared test was used to compare baseline variables across 3 treatment groups. Our primary outcome was the change over time in 17-item HAM-D scores. A piece-wise linear mixed-effects model (Laird and Ware, 1982) was used to assess differences in the change over time of HAMD-17 from baseline to week 12. Time was considered as a continuous variable with two time segments corresponding to the 2 linear terms: 0 to 6 weeks and 6 to 12 weeks since baseline. Treatment condition, time, and an interaction term “visit week*treatment group” were included in the model. We also adjusted for baseline HAM-D value by including it as a covariate in the model. The test of intention-to-treat differences in HAM-D between treatment conditions over time was conducted by a joint Wald test for significance of the time by treatment group interaction terms in the model. Change in BDI over time between treatment conditions was also examined using mixed-effects models similar to the primary outcome variable. We examined the CGI/C binary outcome of improvement (i.e., CGI/C score of 1 = “very much improved” or 2 = “much improved” was considered “improvement”) using a generalized estimating equations (GEE) model, treating time as a continuous variable. The joint Wald test for significance of the treatment × time interaction term was conducted to assess for differences in improvement over time between treatment conditions. Odds ratios and 95% confidence intervals (CI) of change in CGI/C score at 12 weeks for sertraline versus placebo and for R. rosea versus placebo were calculated using model parameter estimates. Diagnostic plots were generated for model checking and no violations of model assumptions were found. Sensitivity analyses were conducted to explore the impact of missing values by performing completers analysis and last observation carried forward (LOCF) analyses.
Results
Between December 2010 and April 2013, we screened 271 patients (Fig. 1). Of those, 195 (72%) were not eligible and 19 (7%) declined participation. Fifty-seven patients were consented and randomized: R. rosea (n=20), sertraline (n=19), or placebo (n=18). By week 8, thirteen patients (22.8%) discontinued treatment: 2 (3.5%) were due to adverse events, both were in the sertraline group; 1 (1.7%) withdrew consent, 6 (10.5%) were lost to follow-up and 4 (7.0%) ended participation due to lack of efficacy. Study participant characteristics are seen in Table 1. Overall, 26(45.6%) were female, 18 (31.6%) were of non-White race/ethnicity. No statistically significant differences were found in baseline characteristics among treatment groups.
Figure 1.
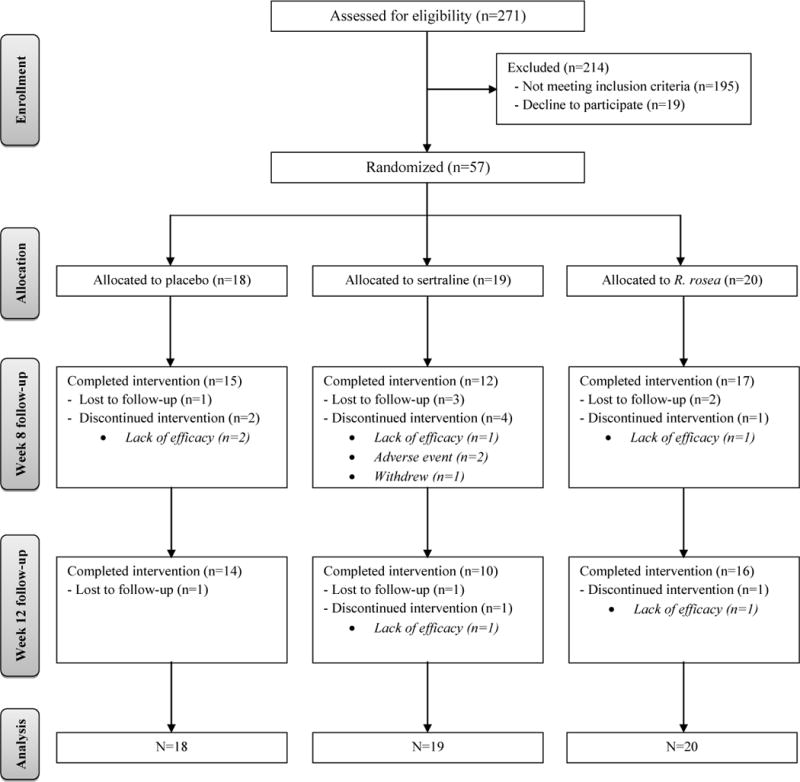
Screening, Randomization and Completion of 12-Week Evaluations
Table 1.
Baseline characteristics of the study participants1
| Variables | Placebo (N=18) |
Sertraline (N=19) |
R. rosea (N=20) |
P-values |
|---|---|---|---|---|
| Gender- # of subjects (%) | 0.73 | |||
| Male | 10 (56) | 9 (47) | 12 (60) | |
| Female | 8 (44) | 10 (53) | 8 (40) | |
|
| ||||
| Race – # of subjects (%)2 | 0.58 | |||
| White | 14 (78) | 12 (63) | 13 (65) | |
| Non-white | 4 (22) | 7 (37) | 7 (35) | |
|
| ||||
| Age (years) | 46.7±15.2 | 41.4±14.6 | 46.9±16.9 | 0.48 |
|
| ||||
| Age at onset MDD (years) | 22.7±13.0 | 19.6±11.3 | 28.4±14.9 | 0.11 |
|
| ||||
| Illness duration (years) | 23.9±20.2 | 21.8±15.3 | 18.4±14.2 | 0.59 |
|
| ||||
| Episode duration (months) | 87.2±181.2 | 12.2±9.3 | 33.0±40.1 | 0.077 |
| - # (%) < 2 years | 12 (67) | 16 (84) | 10 (50) | |
| - # (%) >= 2 years | 6 (33) | 3 (16) | 10 (50) | |
|
| ||||
| # (%) of subjects with secondary diagnosis | 10 (56) | 16 (84) | 16 (80) | 0.10 |
|
| ||||
| Prior exposure to antidepressant- # of subjects (%) | 0.31 | |||
| - # (%) Never used | 6 (33) | 6 (32) | 9 (45) | |
| - # (%) Used 1 antidepressant | 2 (11) | 7 (37) | 4 (20) | |
| - # (%) Used 2 antidepressants | 6 (33) | 2 (10) | 2 (10) | |
| - # (%) Used >=3 antidepressants | 4 (22) | 4 (21) | 5 (25) | |
|
| ||||
| Family history of mood disorder- # of subjects (%) | 13 (72) | 14 (74) | 13 (65) | 0.82 |
|
| ||||
| Baseline HAM-D 17 | 14.4±2.1 | 15.4±3.9 | 14.4±3.7 | 0.59 |
|
| ||||
| Baseline HAM-D total | 19.4±2.6 | 20.8±4.1 | 19.0±4.2 | 0.30 |
|
| ||||
| Baseline CGI-S | 0.064 | |||
| - #(%) Mild | 1 (5) | 3 (16) | 7 (35) | |
| - #(%) Moderate | 17 (95) | 16 (84) | 13 (65) | |
|
| ||||
| Baseline BDI | 19.4±8.0 | 24.6±8.8 | 23.7±7.9 | 0.13 |
Abbreviations: HAM-D (Hamilton Depression Rating Scale); CGI-S (Clinical Global Impression Symptom Severity); BDI (Beck Depression Invenotry)
Plus-minus values are means ± SD unless otherwise noted.
Race was reported by the subjects.
Efficacy Outcomes
There was no statistically significant difference in change over time in HAM-D 17 scores among treatment groups (p=0.79) (Fig. 2). Overall, the decline in HAM-D 17 scores by week 12 of treatment was somewhat greater for sertraline (−8.2, 95% confidence interval [CI], −12.7 to −3.6) versus R. rosea (−5.1, 95% CI: −8.8 to −1.3) and placebo (−4.6, 95% CI: −8.6 to −0.6). There was no statistically significant difference in change over time in BDI (Fig. 3) or CGI/C scores among treatment conditions (p=0.28 and p=0.17, respectively). However, there were clinically meaningful odds ratios (95% CI) of global improvement by week 12 (versus placebo) of 1.39 (0.38–5.04) and 1.90 (0.44–8.20) for R. rosea and sertraline, respectively. This indicates that patients taking R. rosea had 1.4 times the odds of improvement, and patients on sertraline had 1.9 times the odds of improvement, by week 12 of treatment versus those taking placebo. Both completers-only and LOCF sensitivity analyses provided similar results as in original analyses.
Figure 2.
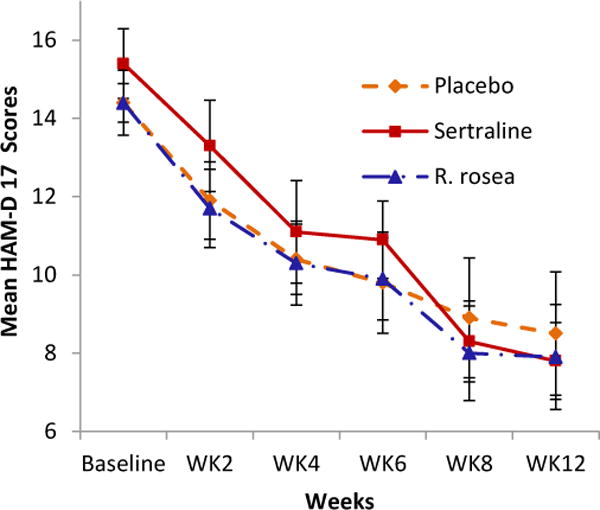
Mean change in HAM-D 17 scores among treatment groups
Figure 3.
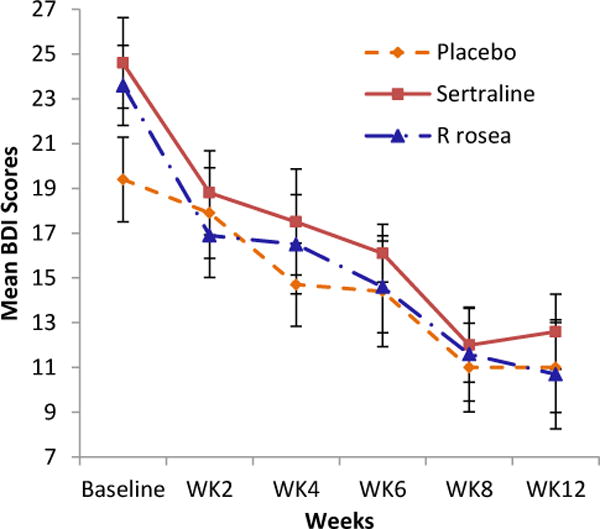
Mean change in BDI scores among treatment groups
Safety
There were no treatment-related serious adverse events. More patients reported study-related adverse events using sertraline (63.2%) versus R. rosea (30.0%) or placebo (16.7%) (p=0.012) (Table 2). Two patients discontinued sertraline treatment because of adverse events: one for palpitations and one for headache, insomnia, and sexual dysfunction. No patient prematurely discontinued R. rosea or placebo therapy. There were no clinically meaningful differences in changes in systolic and diastolic blood pressure, pulse rate, or weight in either R. rosea or sertraline groups. No significant changes were observed in any laboratory values for any treatment group.
Table 2.
Adverse events profiles among treatment groups
| Placebo (N=18) |
Sertraline (N=19) |
R. rosea (N=20) |
P-value | |
|---|---|---|---|---|
| # (%) of subjects experienced AE | 3 (17) | 12(63) | 6 (30) | 0.012 |
|
| ||||
| Total # of AEs experienced* | 14 | 52 | 12 | |
| -Nausea | 0 | 10 | 0 | |
| -Sexual dysfunction | 0 | 7 | 0 | |
| -Appetite change | 0 | 4 | 0 | |
| -Insomnia | 0 | 4 | 0 | |
| -Palpatations | 0 | 3 | 0 | |
| -Gastrointestinal disturbance | 0 | 3 | 0 | |
| -Yawning | 0 | 3 | 0 | |
| -Dry mouth | 0 | 2 | 0 | |
| -Fatigue | 0 | 2 | 0 | |
| -Headache | 0 | 2 | 0 | |
| -Nervousness | 2 | 2 | 2 | |
| -Dizziness | 0 | 0 | 2 | |
Only adverse events experienced by more than 1 subject were listed in the table.
Discussion
This study represents the first randomized, double-blind, placebo-controlled, comparison trial of oral R. rosea extract versus conventional antidepressant therapy of mild to moderate MDD. Although the study was not specifically powered to detect small statistically significant differences between treatment groups for the primary outcome measure, we nonetheless found clinically meaningful (albeit non-significant) reductions over time in HAM-D scores for both R. rosea extract and sertraline. While overall efficacy did not differ from that of placebo, there were significantly more side effects reported with sertraline (p=0.012) and more premature treatment discontinuation with sertraline, resulting in a potentially more favorable benefit to risk ratio for R rosea.
Our study adds to a very small body of research of R. rosea in humans (Panossian et al., 2010). Olsson (Olsson et al., 2009) et al. examined the effect of R. rosea on stress-induced fatigue in 30 subjects taking R. rosea extract versus 30 subjects on placebo. Significant reductions in fatigue, depression, and performance ratings occurred in both groups; while significant group differences favoring R. rosea occurred for the fatigue and performance ratings. In an open-label study of 10 subjects, Bystritsky et al. (2008) reported a positive anxiolytic benefit for R. rosea (Rhodax®) after 10 weeks, with a significant reduction in mean depression rating score (p=0.001). In a 6-week randomized trial, Darbinyan et al. (2007) studied the safety and efficacy of R. rosea SHR-5 extract in mild to moderate major depressive episode in 31 subjects taking SHR-5 340 mg/day, 29 taking SHR-5 680 mg/day, and 29 taking placebo. SHR-5 was reported to produce significant reductions in depressed mood as compared to placebo.
Several caveats should be considered in the interpretation of the present findings. This study was designed to generate preliminary efficacy and safety data to determine sample size estimates for a future, fully-powered study. As a result, we anticipated that we would not be able to detect small, statistically significant differences between groups. The limited sample size also affected the equal distribution of clinical covariates among treatment groups during the randomization process. For example, the sertraline group had slightly higher HAM-D scores at baseline. This difference in symptom severity may have contributed to the greater efficacy of sertraline versus R. rosea (compared to placebo). In this regard, several prior studies have shown conventional antidepressants to be more effective in more severely ill patients (Elkin et al., 1995). Thus, sertraline may have produced greater efficacy than R. rosea because the subjects in the sertraline group were more severely ill. To partially address this difference, we adjusted for baseline HAM-D and BDI scores in our main analyses.
One might interpret our data as showing that neither study drug was efficacious relative to placebo. Conversely, one could also conclude that sertraline and R. rosea were both relatively effective (albeit R. rosea to a much lesser extent). In this regard, we would note that by week 12, sertraline produced a 3.6 point more reduction in the HAM-D 17 score than placebo whereas R. rosea produced only a 0.5 point more reduction than placebo. We would further acknowledge that, while the difference in HAM-D 17 reduction between treatments favored sertraline, it would be difficult to extrapolate from the small sample size and the limited power whether or not R. rosea would ultimately demonstrate a clinically relevant difference from placebo in more mildly depressed individuals.
The inclusion of a placebo control was necessary for assessing the relative benefit to risk ratios among study drugs.
Several large scale clinical trials have suggested that conventional antidepressants may be less effective in mild (versus more severe) forms of depression and produce more side effects (Fournier et al., 2010). In the current trial, we believe that we may have shown a potentially more favorable benefit to risk ratio for R. rosea subjects (even though sertraline demonstrated a greater efficacy), and others have shown similar results for hypericum and other botanicals in mild to moderate depression (Roder et al., 2004; Sayyah et al., 2006; Schrader, 2000).
For the large population of patients with mild to moderate depressive symptoms, a better risk/benefit ratio will not only be an important factor in a patient’s decision to initiate treatment, but also in their ability to maintain adherence sufficiently to experience sustained benefit (Zimmermann et al., 2013). For example, the two subjects in the sertraline group withdrew due to intolerable adverse events despite experiencing clinical benefit.
R. rosea may have produced a more robust antidepressant response if we had employed a larger dose of the extract. The selection of the R. rosea dose was based upon prior studies of healthy volunteers treated for short durations (Shevtsov et al., 2003; Walker et al., 2007) and one prior antidepressant trial (Darbinyan et al., 2007). The paucity of pharmacokinetic and pharmacodynamic profiles of R. rosea (or its constituents), made it difficult to determine the optimal dosing strategy. Furthermore, because we used a dose-escalation design, we were unable to determine whether or not there might be a dose-response relationship for R. rosea extract in reducing depression.
Patients enrolled in the study had more mild MDD symptoms and may have qualitatively differed from populations of more severely ill patients included in other MDD trials of conventional antidepressant agents. It is possible that the beneficial effect of R. rosea seen in this study is limited to individuals with mild to moderate MDD, and patients with more severe MDD would not benefit from R. rosea therapy. We would note, however, that the improvement in MDD symptoms in the present study was not limited to patients with milder MDD. Finally, the treatment duration of the current study was limited to 12 weeks, and future studies of longer duration will be needed to more fully assess the durability of R. rosea’s antidepressant effect.
Conclusion
The identification of a safe and effective alternative therapy for mild to moderate MDD would be of public health relevance for many individuals unable, or unwilling, to use conventional antidepressant therapy. The current double-blind, placebo-controlled study represents the first controlled efficacy and tolerability study of R. rosea extract versus a conventional antidepressant for mild to moderate MDD. Despite the limitations of this preliminary study, the present findings suggest that R. rosea may possess modest antidepressant effects in some patients with mild to moderate MDD. R.rosea may be better tolerated than sertraline, which suggests its potential as a treatment alternative for patients who are intolerant to the adverse effects of conventional anti-depressants.
Acknowledgments
We thank Alexander Panossian, PhD of the Swedish Herbal Institute for his support and assistance in obtaining IND approval for R. rosea SHR-5 extract from the U.S. Food and Drug Administration. We also thank The Swedish Herbal Institute (Gothenburg, Sweden) for providing R. rosea SHR-5 extract for the study. The Swedish Herbal Institute had no role in design, conduct or report of the study. We thank the staff of the Depression Research Unit and Investigational Drug Service of the University of Pennsylvania for their dedication to our research. We also thank our Data Safety and Monitoring Board members Drs. Andy Nierenberg, Sara Ratcliffe and Jan Fawcett for volunteering their time and expertise. Finally, we thank all the study participants for their time and contribution to clinical research.
Funding: This work was supported in part by the National Institutes of Health Center for Complementary and Alternative Medicine (NCCAM) grant R21 AT005230 and by the Jack Warsaw Fund for Research in Biological Psychiatry, University of Pennsylvania. Dr. Mao is supported by NCCAM K23 AT004112.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Financial Disclosures
None of the authors are a member of any pharmaceutical or industry-sponsored advisory board or speaker’s bureau, and none of the authors have any financial interest in any pharmaceutical or herbaceutical company.
References
- Abidov M, Crendal F, Grachev S, Seifulla R, Ziegenfuss T. Effect of extracts from Rhodiola rosea and Rhodiola crenulata (Crassulaceae) roots on ATP content in mitochondria of skeletal muscles. Bulletin of experimental biology and medicine. 2003;136:585–587. doi: 10.1023/b:bebm.0000020211.24779.15. [DOI] [PubMed] [Google Scholar]
- Anonymous. National Institute of Mental Health. TESS (Treatment Emergent Symptom Scale–Write In) Psychopharmacol Bull. 1985:1069–1072. [Google Scholar]
- Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Advance data. 2004:1–19. [PubMed] [Google Scholar]
- Beck A, Steer R, Carbin M. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review. 1988:77–100. [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of general psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Brown R, G P, Ramazanov Z. Rhodiola rosea: a phytomedicinal overview. HerbalGram. 2002:40–52. [Google Scholar]
- Bystritsky A, Kerwin L, Feusner JD. A pilot study of Rhodiola rosea (Rhodax) for generalized anxiety disorder (GAD) Journal of alternative and complementary medicine (New York, NY) 2008;14:175–180. doi: 10.1089/acm.2007.7117. [DOI] [PubMed] [Google Scholar]
- Darbinyan V, Aslanyan G, Amroyan E, Gabrielyan E, Malmstrom C, Panossian A. Clinical trial of Rhodiola rosea L. extract SHR-5 in the treatment of mild to moderate depression. Nordic journal of psychiatry. 2007;61:343–348. doi: 10.1080/08039480701643290. [DOI] [PubMed] [Google Scholar]
- Darbinyan V, Kteyan A, Panossian A, Gabrielian E, Wikman G, Wagner H. Rhodiola rosea in stress induced fatigue–a double blind cross-over study of a standardized extract SHR-5 with a repeated low-dose regimen on the mental performance of healthy physicians during night duty. Phytomedicine: international journal of phytotherapy and phytopharmacology. 2000;7:365–371. doi: 10.1016/S0944-7113(00)80055-0. [DOI] [PubMed] [Google Scholar]
- Elkin I, Gibbons RD, Shea MT, Sotsky SM, Watkins JT, Pilkonis PA, Hedeker D. Initial severity and differential treatment outcome in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. Journal of consulting and clinical psychology. 1995;63:841–847. doi: 10.1037//0022-006x.63.5.841. [DOI] [PubMed] [Google Scholar]
- First M, Spitzer R, Gibbon M, et al. In: Structured Clinical Interview for DSM-Research Version, Patient IV-TR Axis I Disorders, Edition with Psychotic Screen (SCID-I/P W/PSY Screen) Institute, N.Y.S.P., editor. Biometrics Research; New York, NY: 2001. [Google Scholar]
- Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam JD, Shelton RC, Fawcett J. Antidepressant drug effects and depression severity: a patient-level meta-analysis. Journal of the American Medical Association. 2010;303:47–53. doi: 10.1001/jama.2009.1943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guy W. In: ECDEU Assessment Manual for Psychopharmacology. US Department of Health, E.a.W, editor. Rockville, MD: 1976. [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang PS. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) Journal of the American Medical Association. 2003;289:3095–3105. doi: 10.1001/jama.289.23.3095. [DOI] [PubMed] [Google Scholar]
- Laird NM, Ware JH. Random-effects models for longitudinal data. Biometrics. 1982;38:963–974. [PubMed] [Google Scholar]
- Lazarova MB, Petkov VD, Markovska VL, Petkov VV, Mosharrof A. Effects of meclofenoxate and Extr. Rhodiolae roseae L. on electroconvulsive shock-impaired learning and memory in rats. Methods and findings in experimental and clinical pharmacology. 1986;8:547–552. [PubMed] [Google Scholar]
- Lishmanov Iu B, Trifonova Zh V, Tsibin AN, Maslova LV, Dement’eva LA. Plasma beta-endorphin and stress hormones in stress and adaptation. Biulleten’ eksperimental’noi biologii i meditsiny. 1987;103:422–424. [PubMed] [Google Scholar]
- Mao JJ, Li QS, Soeller I, Xie SX, Amsterdam JD. Rhodiola rosea therapy for major depressive disorder: a study protocol for a randomized, double-blind, placebo- controlled trial. Journal of clinical trials. 2014;4:170. doi: 10.4172/2167-0870.1000170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsson EM, von Scheele B, Panossian AG. A randomised, double-blind, placebo-controlled, parallel-group study of the standardised extract shr-5 of the roots of Rhodiola rosea in the treatment of subjects with stress-related fatigue. Planta medica. 2009;75:105–112. doi: 10.1055/s-0028-1088346. [DOI] [PubMed] [Google Scholar]
- Panossian A, Hambardzumyan M, Hovhanissyan A, Wikman G. The adaptogens rhodiola and schizandra modify the response to immobilization stress in rabbits by suppressing the increase of phosphorylated stress-activated protein kinase, nitric oxide and cortisol. Drug target insights. 2007;2:39–54. [PMC free article] [PubMed] [Google Scholar]
- Panossian A, Wikman G, Sarris J. Rosenroot (Rhodiola rosea): traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine: international journal of phytotherapy and phytopharmacology. 2010;17:481–493. doi: 10.1016/j.phymed.2010.02.002. [DOI] [PubMed] [Google Scholar]
- Petkov VD, Yonkov D, Mosharoff A, Kambourova T, Alova L, Petkov VV, Todorov I. Effects of alcohol aqueous extract from Rhodiola rosea L. roots on learning and memory. Acta physiologica et pharmacologica Bulgarica. 1986;12:3–16. [PubMed] [Google Scholar]
- Roder C, Schaefer M, Leucht S. Meta-analysis of effectiveness and tolerability of treatment of mild to moderate depression with St. John’s Wort. Fortschritte der Neurologie-Psychiatrie. 2004;72:330–343. doi: 10.1055/s-2003-812513. [DOI] [PubMed] [Google Scholar]
- Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, Niederehe G, Thase ME, Lavori PW, Lebowitz BD, McGrath PJ, Rosenbaum JF, Sackeim HA, Kupfer DJ, Luther J, Fava M. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. The American journal of psychiatry. 2006;163:1905–1917. doi: 10.1176/ajp.2006.163.11.1905. [DOI] [PubMed] [Google Scholar]
- Saratikov AS, Lomov NI, Syrneva NV, Chernova NA, Prushchep TP, Lavrent’eva LN, Shchipkova LG. Physiological activity and some physico-chemical properties of acyl derivatives of pyrazolone. Farmakologiia i toksikologiia. 1968;31:437–441. [PubMed] [Google Scholar]
- Sayyah M, Sayyah M, Kamalinejad M. A preliminary randomized double blind clinical trial on the efficacy of aqueous extract of Echium amoenum in the treatment of mild to moderate major depression. Progress in neuro-psychopharmacology & biological psychiatry. 2006;30:166–169. doi: 10.1016/j.pnpbp.2005.10.005. [DOI] [PubMed] [Google Scholar]
- Schrader E. Equivalence of St John’s wort extract (Ze 117) and fluoxetine: a randomized, controlled study in mild-moderate depression. International clinical psychopharmacology. 2000;15:61–68. doi: 10.1097/00004850-200015020-00001. [DOI] [PubMed] [Google Scholar]
- Shevtsov VA, Zholus BI, Shervarly VI, Vol’skij VB, Korovin YP, Khristich MP, Roslyakova NA, Wikman G. A randomized trial of two different doses of a SHR-5 Rhodiola rosea extract versus placebo and control of capacity for mental work. Phytomedicine: international journal of phytotherapy and phytopharmacology. 2003;10:95–105. doi: 10.1078/094471103321659780. [DOI] [PubMed] [Google Scholar]
- van Diermen D, Marston A, Bravo J, Reist M, Carrupt PA, Hostettmann K. Monoamine oxidase inhibition by Rhodiola rosea L. roots. Journal of ethnopharmacology. 2009;122:397–401. doi: 10.1016/j.jep.2009.01.007. [DOI] [PubMed] [Google Scholar]
- Walker TB, Altobelli SA, Caprihan A, Robergs RA. Failure of Rhodiola rosea to alter skeletal muscle phosphate kinetics in trained men. Metabolism: clinical and experimental. 2007;56:1111–1117. doi: 10.1016/j.metabol.2007.04.004. [DOI] [PubMed] [Google Scholar]
- Williams JB. A structured interview guide for the Hamilton Depression Rating Scale. Archives of general psychiatry. 1988;45:742–747. doi: 10.1001/archpsyc.1988.01800320058007. [DOI] [PubMed] [Google Scholar]
- Zimmermann TM, Clouth J, Elosge M, Heurich M, Schneider E, Wilhelm S, Wolfrath A. Patient preferences for outcomes of depression treatment in Germany: a choice-based conjoint analysis study. Journal of affective disorders. 2013;148:210–219. doi: 10.1016/j.jad.2012.11.062. [DOI] [PubMed] [Google Scholar]